
Abstract
Background
Nasal preparation prior to flexible laryngoscopy is a common ENT practice. Co-phenylcaine is increasingly used because it is safe and has both anaesthetic and vasoconstrictive properties. Lidocaine 4% and epinephrine 1:1000 nasal packing is another method used in our department.
Methods
A prospective case series was performed on eighty-one patients requiring flexible laryngoscopy. Patients were enrolled into either a co-phenylcaine or a lidocaine/epinephrine packing group. Visual analogue scales (VAS) were used to record unpleasantness of nasal preparation and flexible laryngoscopy. Decongestion and ease of endoscope passage were recorded by the doctors.
Results
Bad taste was statistically significantly worse when using cophenylcaine for nasal preparation (P = 0.001). However, there was no statistically significant difference in overall unpleasantness from nasal preparation or from subsequent flexible laryngoscopy between the two groups. There was no statistically significant difference in degree of decongestion or ease of endoscope passage between the two groups.
Conclusion
There is no statistically significant advantage of using cophenylcaine spray over non-proprietary lidocaine 4% and epinephrine 1:1000 nasal packing. However cost and bad taste is less with nasal packing.
Introduction
Prior to flexible laryngoscopy topical nasal preparation is traditionally used to reduce patient discomfort and ease passage of the scope. The ideal nasal preparation should be comfortable for the patient, produce adequate anaesthesia and widen nasal patency. Cocaine was popular for many years due to its potent analgaesic and vasoconstrictive properties. However controlled drug regulations and safety concerns have led to alternatives. Co-phenylcaine is a commercially available solution of 5% lidocaine and 0.5% phenylephidrine, and has become increasingly popular in the last decade. Co-phenylcaine has been shown to be safe 1 and as effective as cocaine for both flexible 2 and rigid nasendoscopy.3,4 Compared with lidocaine spray alone, co-phenylcaine was found to provide an easier passage and better view for rigid nasendoscopy, 5 and less unpleasantness for flexible nasendoscopy. 6 This is due to the vasoconstrictive properties of phenylephidrine. Another advantage of co-phenylcaine is that it is available in a single use disposable spray device (basic NHS price £8.73), avoiding contamination of the nozzle tip or “suckback” of secretions that may occur with multiple-use spray devices. 7 One disadvantage of co-phenylcaine is the bad taste it produces, which can paradoxically make the procedure more uncomfortable than placebo. 8 Use of co-phenylcaine for nasendoscopy remains a contentious issue with two studies suggesting it confers no benefit over no preparation,9,10 although these studies have been criticised for using a sub-therapeutic dose resulting in ineffective topical anaesthesia. Further research has shown that co-phenylcaine spray is more effective if 10 minutes is allowed for it to take effect. 11
Lidocaine 4% and epinephrine 1:1000 administered using cotton pledget nasal packing is an alternative method which also has anaesthetic and vasoconstrictive properties, but is significantly cheaper and associated with less wastage and packaging than single use co-phenylcaine.
Materials and Methods
Eighty-one patients requiring flexible laryngoscopy as part of laryngeal examination were invited to take part in this prospective audit over 4 months between April and July 2008 in the ENT outpatients department, Craigavon Hospital (Craigavon, Northern Ireland). Hospital Ethics Committee approval was granted prior to the study and written informed consent was obtained from every patient by the doctor with the aid of standardised forms explaining the nature of the study and the voluntary nature. Patients were excluded from the study if they required endoscopic examination of the nasal cavity, if they were pregnant, allergic to the preparations used or not capable of consent. Choice of spray or packing was at the discretion of the surgeon, but generally co-phenylcaine spray was used during the first two months, changing to lidocaine and epinephrine packing in the final two months.
The null hypothesis was that there is no difference between co-phenylcaine spray and lidocaine 4% and epinephrine 1:1000 nasal packing for preparing the nose prior to flexible laryngoscopy in terms of (1) patient comfort; and (2) degree of decongestion and ease of endoscope passage.
After obtaining consent, the nose was prepared with either 5 sprays of co-phenylcaine or packed with a moist cotton pledget soaked in an equal mixture of lidocaine 4% and epinephrine 1:1000.
The size of the cotton pledget was dependant on the size of the nasal cavity. Care was taken to ensure that the cotton pledget was moist and not dripping when inserted.
After at least 10 minutes, any nasal packs were removed and flexible laryngoscopy was performed using a Karl Storz 3.7 mm unsheathed and lubricated nasendoscope. In the presence of septal deviation, the least deviated side was chosen. A visual analogue scale (VAS) was used to record patient experiences of the nasal preparation, flexible laryngoscopy and combined unpleasantness of preparation and laryngoscopy. A score of 100 was considered to be the maximal unpleasantness or other outcome a patient could possibly experience. A score of 0 was considered as no recordable unpleasantness or negative experience from the procedure.
Nasal preparation comprised bad taste, pain, anxiety and overall unpleasantness. Flexible laryngoscopy comprised pain, anxiety, gagging and overall unpleasantness.
The surgeon used a visual analogue scale to record:
Degree of decongestion
Ease of endoscope passage
Other details: including Cottle's grading of septal deviation of side scoped and time given for preparation to take effect.
A mulitfactorial analysis of variance was performed using statistical software package SPSS version 16. The SPSS analysis for the General Linear Model with Type III sums of squares was used to undertake a separate analysis of variance for each type of visual analogue scale score accounting for the factors Method, Sex, Surgeon, Lubricant, and Passage direction.
Results and Analysis
Eighty-one patients were recruited, 39 male and 42 female, aged between 19 and 86 years. No patient declined to take part in the study. Forty two patients received co-phenylcaine spray and 39 patients lidcocaine 4% and epinephrine 1:1000 cotton wool pledget nasal packing (see Table 1).
Numbers of patients.
Bad taste was found to be statistically significantly worse with co-phenylcaine spray (P = 0.001), with a mean value of 32 (95% CI 24.7–39.7) associated with co-phenylcaine spray versus 7.2 from nasal packing (95% CI –0.2–14.6). There was no statistically significant difference in pain or anxiety between the two methods (P = 0.67 and P = 0.11 respectively) (see Fig 1).
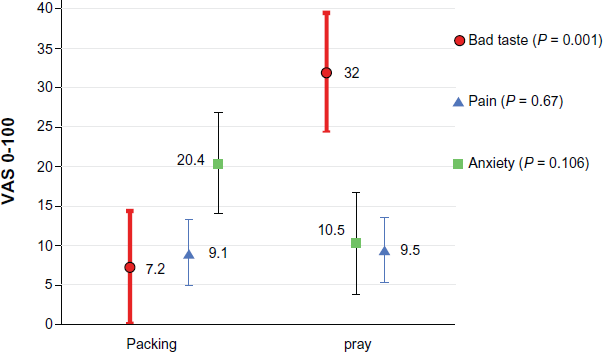
Mean values of patient experiences from nasal preparation with 95% CI.
Overall unpleasantness was greater in the co-phenylcaine group with mean values of 23.1 versus 12.0 with lidocaine and epinephrine group, but this did not reach statistical significance (P = 0.057; 95% CI 5.6–18.3) (see Fig 3).
There was no statistically significant difference in gagging, pain, anxiety or overall unpleasantness associated with flexible laryngoscopy between the two methods (P = 0.37, P = 0.87, P = 0.06 and P = 0.21 respectively) (see Fig 2 and Fig 3).
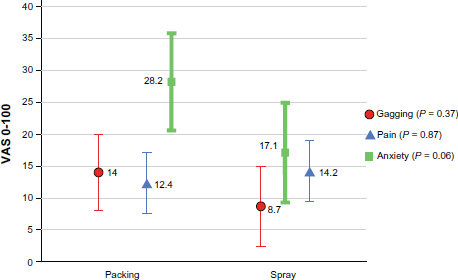
Mean values of patient experiences of flexible laryngoscopy with 95% CI.
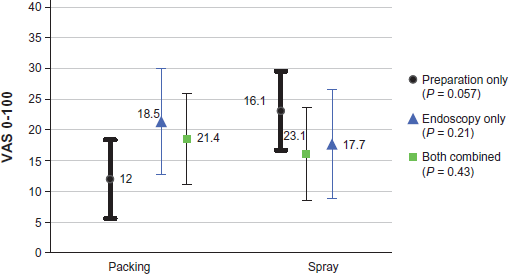
Mean values of unpleasantness from procedures with 95% CI.
There was no statistically significant difference in overall combined unpleasantness with mean values of 23.1 for cophenylcaine and 21.4 for lidocaine and epinephrine (P = 0.428) (see Fig 3).
There was no statistically significant difference in the degree of decongestion with spray and packing achieving mean values of 59 and 68 respectively (P = 0.12).
There was no statistically significant difference between methods on ease of endoscope passage (P = 0.64). However there was a significant relationship between the increasing septal deviation and ease of insertion (P = 0.003).
Discussion
This audit has shown no advantage in using co-phenylcaine spray over lidocaine 4% and epinephrine 1:1000 cotton pledget nasal packing for flexible laryngoscopy. There is statistically significantly worse bad taste associated with co-phenylcaine spray compared with lidocaine and epinephrine packing. There was no statistical significance that overall unpleasantness is higher using co-phenylcaine, (P = 0.057). As mean values for pain from nasal preparation were low with both methods, and anxiety was lower with co-phenylcaine, bad taste is probably the main factor for unpleasantness from cophenylcaine spray.
Neither method was superior for decreasing pain, anxiety, gagging or overall unpleasantness associated with subsequent flexible laryngoscopy. The design of this study did not contain a placebo arm to determine if this was due to similar efficacy or no efficacy of the active treatments.
Both preparations resulted in similar decongestion and there was no difference in ease of endoscope passage between the methods.
This prospective study has inherent bias, particularly as it was non-blinded and non-randomised (ethical approval was not granted to allow randomisation of patients). Whilst application of co-phenylcaine is a relatively non-operator dependant procedure; nasal packing and flexible laryngoscopy are by their nature quite operator dependant, and the skill of the surgeon performing the procedure may be more important than the actual method chosen to prepare the nose. Because the distribution of patients was not equal amongst the surgeons this may have skewed results. Similarly as the study was not randomised, and method was chosen at the discretion of the surgeon, it is possible that the procedural technique of the individual surgeon may have changed over the 4 month study time, or that method chosen may have been dependant on the doctors opinion of the patient, or other factors like convenience and personal preference. The assessor was not blinded to group assignment as it was an audit of current practice, and blinding was not practical in a busy outpatient clinic setting where a second doctor was not always available.
Whether nasal preparation is actually beneficial for nasendoscopy remains a contentious issue. Although a review by Pothier et al, 12 attempts to draw conclusions, studies on this topic are of relatively small sample size with differing methodologies and results, making cumulative analysis difficult. A common theme is that local anaesthesia alone has no benefit over placebo,8–10 but that addition of a vasoconstrictor may have a clinical benefit in preparing the nose for nasendoscopy. 5 Indeed, vasoconstriction alone may be the most important factor, since the addition of lidocaine can actually make the experience more unpleasant for the patient. 6
Our study is the only study that compares lidocaine and epinephrine packing with co-phenylcaine spray for flexible laryngoscopy. A nasendoscopy study by Kasemsuwan et al 13 concluded that lidocaine 4% and epinephrine 1:1000 in spray form is as effective as cocaine 10% spray in producing local anaesthesia and vasoconstriction.
Lidocaine 4% and epinephrine 1:1000 are readily available. Cotton pledget nasal packing is a simple ENT procedure requiring minimal equipment. The cost of providing this preparation and sterilizing the instruments should not exceed that of purchasing co-phenylcaine and disposing of the relatively bulky packaging.
Conclusion
Lidocaine 4% and epinephrine 1:1000 cotton pledget nasal packing is preferable to co-phenylcaine spray prior to flexible laryngoscopy. Co-phenylcaine has significantly worse bad taste and is not better in reducing unpleasantness from flexible laryngoscopy, nor does it give better decongestion or ease of endoscope passage than lidocaine 4% and epinephrine 1:1000 nasal packing.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
Acknowledgements
Thanks to Michael Parker, at the Clinical Research Support Centre (CRSC), at The Royal Hospitals, Belfast, for his assistance with the statistical analysis.