
Abstract
Nasal obstruction resulting from inferior turbinate hypertrophy was treated by Nd-YAG laser inferior turbinectomy (laser IT). The effectiveness of the procedure was assessed and compared with both functional endoscopic turbinoplasty (turbinoplasty) and conventional partial turbinectomy (conventional IT).
Materials and methods
A retrospective analytic study was carried out for 53 patients suffering from inferior turbinate hypertrophy. Twenty patients underwent Nd-YAG Laser IT (Group 1), 24 patients underwent turbinoplasy (Group 2) and 9 patients underwent conventional IT (Group 3). Improvement in nasal symptoms were assessed. Intra-operative bleeding, duration of hospital stay, and post-operative medications and instrumentation were compared between the three groups.
Results
The symptoms of sneezing, hyposmia and rhinorhoea were significantly reduced post-operatively among patients in the three groups and there were no differences statistically between them.
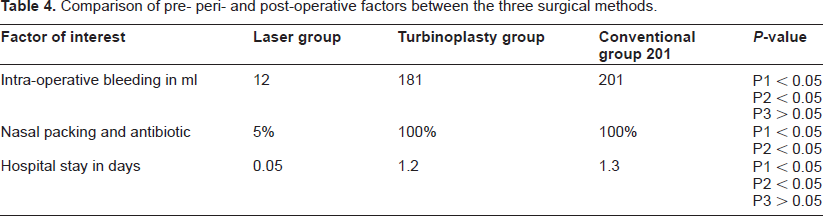
The Nd-YAG laser turbinectomy group showed marked reduction in blood loss (average = 12 ml per patient) compared to the turbinoplasy group (average = 181 ml per patient) and conventional IT group (average 201 ml per patient).
Hospital stay was much shorter in the laser IT group (average = 0.05 days) compared to Group 2 (1.2 days) and Group 3 (1.3 days). Only one patient in the laser IT group required nasal packing, whereas all patients in the other two groups required nasal packing routinely.
Conclusions
Nd-YAG laser IT was effective in reducing the symptoms of nasal obstruction, as well as other nasal symptoms without significant complications. The Nd-YAG laser is recommended as an alternative method, when applicable, in treating patients with nasal obstruction resulting from inferior turbinate hypertrophy.
Keywords
Introduction
Background
During the last few decades, laser technology has enabled innovative advancements in the field of medicine in general and has revolutionized surgery in many fields, including the field of otolaryngology.1,2
Lasers have many advantages. A laser beam is targeted precisely at diseased tissues, while sparing normal tissue nearby; a lower rate of inflammatory reaction is expected at surgical site, resulting in fewer side effects; and the heat produced by lasers sterilizes the surgery site, thus reducing the risk of infection. 3
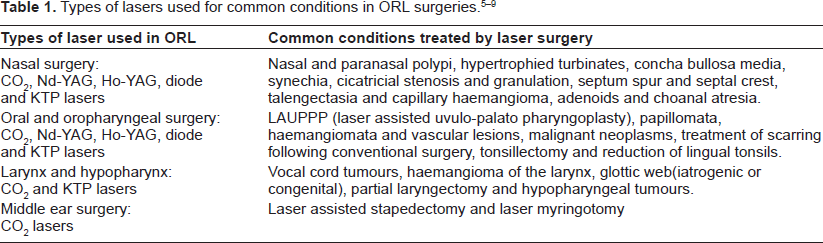
A laser beam is characterized by certain parameters that describe the amount of energy delivered at the tissue, penetration depth and effects on neighbouring tissues. 4 Knowing this is of paramount importance as each type of laser is more suitable for particular tissues and procedures, as shown in Table 1.
Nasal obstruction is a very common complaint in the practice of otolarynglogy that results from many causes. Inferior turbinate hypertrophy constitutes considerable percentage of these obstructions. There is a strong need to adopt a surgical method that is cost-effective in terms of hospital stay and, if possible, can be carried out under local anesthesia. 10 In this study, the advantages of laser in this regard are disclosed.
Study objectives
This study aimed to:
Identify the optimal parameters for partial inferior turbinectomy using the Nd-YAG laser, supplied by Dornier Company, Germany;
Verify improved symptoms in patients following Nd-YAG inferior turbinectomy (laser IT) and compare these results with those obtained following endoscopic inferior turbinectomy (turbinoplasy) and conventional partial turbinectomy (conventional IT);
Compare post-operative discomfort and hospital stay after Nd-YAG laser IT, turbinoplasty and conventional IT.
Materials and Methods
Study design
Retrospective cross-sectional study.
Study subjects and settings
We selected patients who had allergic or vasomotor rhinitis, and were scheduled to undergo reduction of the inferior turbinates. Patients who complained of mainly bilateral nasal obstruction were included. Exclusion criteria:
Patients who had headaches and/or rhinorhoea without nasal obstruction,
Patients with nasal polyps,
Patients with previous nasal surgery.
Partial inferior turbinectomy was done for 53 patients during the period May 2006 to Jan 2008. Conventional and turbinoplasty surgery was performed at the ENT-Khartoum Teaching Hospital. Laser IT procedures were performed at the Laser Clinic, Sudan University of Science and Technology.
Procedures
Patients were divided into three groups:
Group 1 included 20 patients who were operated on using the Nd-YAG laser. The procedure was carried out under local anesthesia for 19 patients. One patient underwent laser inferior turbinectomy under general anesthesia.
Group 2 included 24 patients who underwent turbinoplasty. Patients were selected to match the age, sex and duration of symptoms of the former group; they were selected from the outpatient clinic of ENT Khartoum Teaching Hospital. The procedure was carried out under general anesthesia.
Group 3 includes nine patients who were operated on by conventional surgical tools used for classical partial inferior turbinectomy; they were matched with Group 1 for age, sex and duration of symptoms. The procedure was carried out under general anesthesia.
Data collection and analysis
Data was collected and analyzed in spreadsheets. Statistical significance (P-value) was calculated using the Chi-square test and P value was regarded as significant when less than 0.05.
Results
Patients details
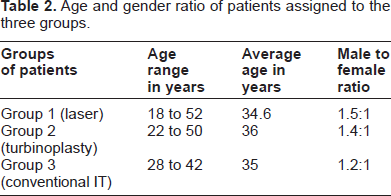
Patients in this study were categorized into three groups, as mentioned above. Each group was subjected to a different surgical method. Their ages ranged from 18 to 52 years. The study included 31 males and 22 females (see Table 2).
Age and gender ratio of patients assigned to the three groups.
Comparison between the three surgical methods
Laser was applied to Group 1 subjects in the form of continuous wave Nd-YAG laser in a contact mode. The power applied to debulk the inferior turbinates was between 9 and 11 W.
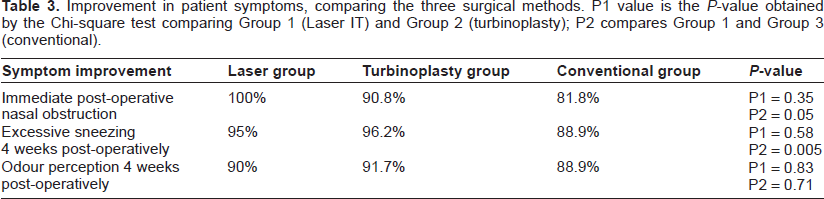
Improvement in symptoms and perioperative events, including blood loss and hospital stay, are summarized in tables 3 and 4.
Improvement in patient symptoms, comparing the three surgical methods. P1 value is the P-value obtained by the Chi-square test comparing Group 1 (Laser IT) and Group 2 (turbinoplasty); P2 compares Group 1 and Group 3 (conventional).
Comparison of pre- peri- and post-operative factors between the three surgical methods.
Discussion
Management of the enlarged inferior turbinates is done by different surgical tools. Controversy still exists as to the best or most appropriate method for surgical reduction of the inferior turbinate. Different surgical methods for turbinate hypertrophy include: cryotherapy, diathermy coagulation, radiofrequency, conventional, functional endoscopic sinus surgery (FESS) IT and coblation assisted partial turbinectomy10–12
When the Nd-YAG laser was applied in a power range less than 9 W, it was found to be insufficient to cause coagulation of bleeding vessels. Higher power (more than 11 W) causes discomfort and pain to the patient, probably due to an increased penetration depth of laser beam.
Regarding improvement in nasal obstruction, Nd-YAG IT showed a 100% success rate. The difference between Nd-YAG IT (100%) and turbinoplasty (90.8%) is statistically insignificant. The availability of pre- and post-operative rhinomanometric evaluation will be helpful as an objective measurement of nasal symptoms.
Improvement of sneezing was satisfactory in all groups, being slightly lower following Nd-YAG IT compared to turbinoplasty and conventional inferior turbinectomy, although the difference is not significant statistically. This could be due to the fact that laser is a very precise surgical tool that has a minimal effect on the mucosa compared to the other two tools. Although laser ablation of the turbinate was found to be effective in improving nasal obstruction, it disturbed the mucociliary function significantly in a study carried out by Sapci et al when compared with the partial turbinectomy technique. 13
Most of the patients showed improvement in odour perception; this coincides with improvement in nasal obstruction, as it is the proposed etiological factor for hyposmia and anosmia.
Surgical turbinate intervention demonstrates a benefit in controlling symptoms of allergic rhinitis other than nasal obstruction. We advocate Nd-YAG inferior turbinectomy as an adjuvant modality of treatment in cases of allergic and vasomotor rhinitis that are refractory to pharmaco- and immunotherapeutic measures.
A marked reduction of blood loss intra-operatively when performing Nd-YAG IT was noted. The results of our study are in agreement with those achieved by et al. 14 This is a great advantage of laser surgery. Blood loss is estimated to be much higher in turbinoplasty and in conventional IT; the latter two are comparable to each other in this regard.
All patients treated by functional endoscopic turbinoplasty and conventional surgery required nasal packing for 24 hrs, at least, and hence antibiotic cover. Only one patient, a diabetic 52-year-old male, required nasal packing in the Nd-YAG group; this was on the third day postoperatively, as he developed epistaxis and consequently was given antibiotic therapy to guard against infection.
Nd-YAG laser IT was carried out as day surgery, where surgery is performed as an outpatient procedure under topical anesthesia, with patients leaving hospital two hours post-operatively. This is a great advantage over turbinoplasty and conventional surgery, where both are performed only under general anesthesia.
The main disadvantage of Nd-YAG laser IT is that patients must be carefully selected. They should have only inferior turbinate hypertrophy, and no other lesions such as a deviated nasal septum and/or nasal polypi. For these conditions, conventional methods, with or without FESS, are superior, as all these pathologies can be corrected at one session since the operation is carried under general anesthesia.
Conclusions
From the results obtained, we conclude that Nd-YAG inferior turbinectomy has many advantages over turbinoplasty and conventional turbinectomy.
Inferior turbinectomy using laser is minimally invasive, it can be done under local anesthesia, it is carried as day surgery with much less blood loss and, usually, there is no need for nasal packing post-operatively. For all these reasons, it is more convenient to the patients.
The outcome of laser inferior turbinectomy depends on good selection of patients, who should have inferior turbinate hypertrophy as the only cause of nasal obstruction.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.