
Abstract
This work assess serum levels of soluble Fas form (sFas) in patients with different stages of laryngeal squamous cell carcinoma(LSCC) to investigate its prognostic significance. We correlate its levels with the morphological changes of peripheral blood cells via buffy coat examinatin. The study population included 70 patients clinically diagnosed and pathohistologically confirmed LSCC in addition to 20 healthy controls. According to TNM classification 33(47.1%) patients were in stage I (group I) and 24(34.3%) in stage II (group II), 13(18.5%) in stage III (group III). The results revealed that the mean serum level of sFas (pg/ml) in the control group was 51.2, in group I was 66.33, in group II was 81.33 and in group III was 112.45. Statistical analysis of the mean of sFas by ELISA test in the patients' groups in comparison to the control revealed a significant increase of both group II and III in comparison to the control group (P < 0.01) but there was no significant difference (P > 0.05) between group I in comparison to either the control or group II. There was a significant difference (P < 0.05) between group I in comparison to group III. LM examination revealed massive extent of the apoptotic cells in group III when compared to both group I and group II. EM examination of the buffy coat revealed apoptotic changes, mainly in the peripheral blood mononuclear cells (PBMNCs), represented by surface membrane ruffles and blebs with clumped nuclear chromatin and vacuolated cytoplasm. In conclusion, this study may help us to better understand one of the escape mechanisms in cancer larynx. This mechanism is represented by the significant increase in both the serum level of sFas and the morphological apoptotic changes that detected in PBMNCs. Soluble Fas may contribute to the progression of laryngeal cancer. It can be used as an attractive target for anticancer therapy and may be considered as a marker of disease progression and poor prognosis in laryngeal cancer.
Keywords
Introduction
Squamous cell carcinoma of the head and neck (SCCHN), including those of the oral cavity, pharynx, and larynx, is the sixth most frequently occurring cancer and the seventh leading cause of cancer-related deaths worldwide. 1 Although tobacco smoking and alcohol use are the major risk factors in the etiology of SCCHN, only a proportion of exposed individuals develops SCCHN in their life span, suggesting individual susceptibility to exposure-related carcinogenesis. 2
Laryngeal cancer is the most common cancer of the upper aerodigestive tract. The incidence of laryngeal tumors is closely correlated with smoking, as head and neck tumors occur 6 times more often among cigarette smokers than among nonsmokers. The age-standardized risk of mortality from laryngeal cancer appears to have a linear relationship with increasing cigarette consumption. Death from laryngeal cancer is 20 times more likely for the heaviest smokers than for nonsmokers. 3
Apoptosis is a biological process that regulates physiologic cell death, varies in different tissues and organisms 4 and plays an important role in maintaining homeostasis. Accumulating evidence suggests that abnormal regulation of apoptosis is likely to contribute to the pathogenesis of a variety of human diseases, including cancer. 5
Fas, also known as TNFRSF6/CD95/APO-1, is a cell surface receptor that is involved in apoptotic signaling in many cell types. 6 Fas ligand (FasLG), also known as TNFSF6/CD95LG, is a member of the tumor necrosis factor superfamily that can trigger the apoptotic cell–death cascade by cross-linking with its receptor, FAS. 7 Therefore, the Fas/FasLG pathway plays a crucial role in regulating apoptosis and maintaining cellular homeostasis. Studies have shown that dysregulation of this pathway leads not only to reduced Fas expression but also to aberrant FasLG expression in a variety of tumors, including SCCHN. 8 Fas and its specific ligand (Fas-L), both of which are involved in apoptosis, exist in membrane-bound and soluble forms(sFas). 9
Because of the role of the Fas genes in regulating cell death, and because abnormal expression of Fas have been observed in a variety of tumors, including SCCHN, we assess serum sFas levels in patients with different stages of laryngeal squamous cell carcinoma (LSCC) according to TNM classification to investigate its prognostic significance, we also correlate its level with the host immune response via the ultrastructural study of the buffy coat.
Subjects and Methods
The study population included 70 patients with newly diagnosed (no history of taking chemotherapy) and pathohistologically confirmed LSCC (laryngeal squamous cell carcinoma) at Kasr El Aini Hospital and 20 cancer-free control subjects recruited between May 2005 and May 2008.
Diagnosis is made by the physicians on the basis of a careful medical history, physical examination and special investigations which include MRI and tissue biopsy.
The physical exam includes a systematic examination of the whole patient to assess general health and to look for signs of associated conditions and metastatic disease. The neck and supraclavicular fossa are palpated to feel for cervical adenopathy, other masses, and laryngeal crepitus. The oral cavity and oropharynx were examined under direct vision. The larynx was examined by indirect laryngoscopy. Fibre-optic nasal endoscopy where a thin and flexible endoscope is inserted through the nostril to clearly visualise the entire pharynx and larynx.
If there was a suspicion of cancer, biopsy was performed, under general anaesthesia. This provides definitive histological proof of cancer type and grade. If the lesion appears to be small and well localised, excision biopsy was undertaken, where an attempt was made to completely remove the tumour at the time of first biopsy. In this situation, the pathologist could not only be able to confirm the diagnosis, but could also comment on the completeness of excision. A full endoscopic examination of the larynx, trachea, and esophagus was often performed at the time of biopsy.
Tumour staging was completed by scanning the head and neck region to accurately assess the local extent of the tumour and any pathologically enlarged cervical lymph nodes.
Cancer-free control subjects were recruited from persons who were not hospital patients or seeking health care, and who accompanied the case patients to the clinics. We first surveyed potential control subjects at the clinics by using a screening sheet to determine their willingness to participate in research studies and to obtain information on demographics, smoking status, and personal history of cancer. We then selected the frequency-matched eligible subjects to the cases by age (x5 years) and sex.
Sample Collection
Blood samples (10 ml) were collected from all subjects at the time of biopsy. One part (5 ml) of blood was centrifuged and serum was freezed at –85 oC till used in detection of soluble Fas (sFas) by ELISA technique. 11
The second part was collected on EDTA tubes for separation of buffy coat to be examined by the electron microscope. The cells were fixed in 4% glutaraldhyde with sodium cacodylate for two hours then postfixed in 2% osmium tetraoxide, dehydrated with ascending concentration of alcohol and embedded in epoxy resin. Semi-thin and ultrathin section sections were cut with a Leika ultra microtome. Semi-thin sections (1 micron)were stained with methylene blue and azure II for detection of morphological features of apoptosis by
Statistical analysis
Version 10 SPSS statistical package (SPSS software Chicago IL) was used to analyze the data. Descriptive statistics included the mean ± SD. Analytical statistics included comparison between variables among groups using student t- test. The data were considered significant if p values were ≤0.05. Correlation study was done using Pearson's correlation.
Results
The cases and controls seemed to be well matched on age and sex: the mean age was 56.0 years for the cases (±10.9 years; range, 23–78 years) and 55.3 years for the controls (±10.6 years; range, 22–75 years), and 76.9% and 22.1% of the cases and 71.1% and 21.9% of the controls were men and women, respectively. As expected, however, there were more current smokers (64.8%) among the cases compared with controls (25.4%) and these differences were statistically significant (P < 0.001).
Among the 70 patients with primary LSCC who were included in the analysis, 47 (67.2%) had cancers of the glottis, 15 (21.2%) had cancers of the supraglottis, and 8(5%) had cancers of the subglottis. According to TNM classification 33(47.1%) patients were in stage I (group I) and 24(34.3%) in stage II (group II), 13(18.6%) in stage III (group III).
SFAS by ELISA
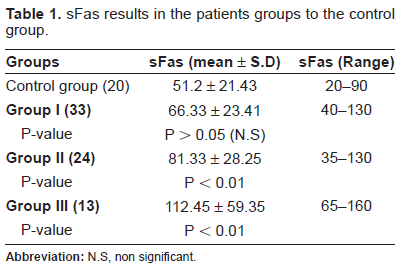
The results revealed that the mean of sFas (pg/ml) in the control group was 51.2 and SD 21.43 with a range of (20–90), the mean of sFas (pg/ml) in group I was 66.33 and SD 23.41 with a range of (40–130), in group II was 81.33 and SD 28.25 with a range (35–130) but in group III was 112.45 and SD 59.35with a range (65–160) (Table 1), (Fig. 1). Statistical analysis of the mean of sFas by ELISA test in the patients' groups in comparison to the control revealed a significant increase of both group II and III in comparison to the control group (P < 0.01) but there was no significant difference (P > 0.05) between group I in comparison to either the control or group II. There was a significant difference (P < 0.05) between group I in comparison to group III.
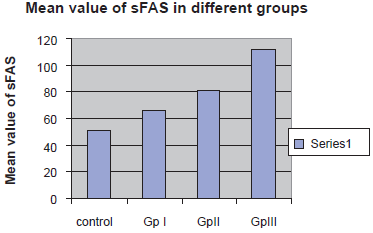
Mean value of sFAS test in the different groups. Statistical analysis of the mean of sFas in the different groups.
sFas results in the patients groups to the control group.
Results of Light Microscope
Examination by light microscope helped us to estimate the extent of the affected cells and to choose the area of ultrathin section for EM examination. The examination revealed massive extent of the apoptotic cells in group III when compared to group I and II (Fig. 2).
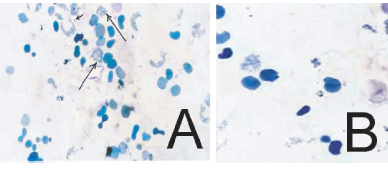
Semithin section of buffy coat from patient with cancer larynx showing the massive extent of the apoptotic cells in group III
Results of Electron Microscope
By EM examination of the buffy coat the apoptotic changes could be detected mainly in the PBMNCs (peripheral blood mononuclear cells) and represented by surface membrane ruffles and blebs with clumped nuclear chromatin and vacuolated cytoplasm (Fig. 3).
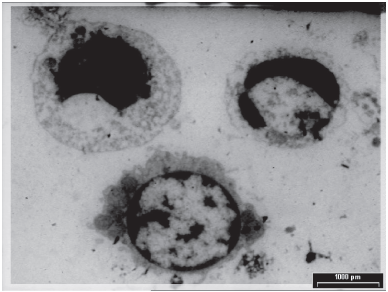
PBMNCs in patient with laryngeal squamous cell carcinoma, showing clumped nuclear chromatin and vacuolated cytoplasm (x 2300).
Discussion
Cell death by the apoptotic pathway is essential for maintaining the normal function of cells, but it can be initiated or inhibited by a variety of stimuli. 14 It has been shown that alterations of Fas expression decrease the apoptotic capacity of cancer cells that become refractory to this apoptotic regulatory signal and thus do not undergo apoptosis under appropriate conditions. 15 Also Pignataro et al 9 found that the loss of Fas receptors is a common feature of most human malignancies and are associated with the progression of cancers, including SCCHN. Therefore, the variants of the Fas could be expected to have an effect on cell death, and thus, carcinogenesis.16,17
Through the present study, we found association between the serum level of sFas and the extend of the lesion. We found a significant increase (P < 0.01) between each of group II and III in comparison to the control and between group I in comparison to group III (P < 0.05) but there was no significant difference (P > 0.05) between group I in comparison to the control or in comparison to group II.
There are several lines of evidence that support our findings. Teppo et al 18 demonstrated that invasive tumour growth of the larynx coincides with an increase of both cellular proliferation and apoptosis. Both parameters, however, affected various tumour areas differently. While there was a preferential expression of the Ki-67 antigen, coincide with cell proliferation, at the tumour–-stroma interface, apoptotic figures could be found randomly distributed in the tumour. This indicates that the replication of tumour cells and tumour cell decay are differently distributed and possibly are independently regulated. Since a particularly strong increase of cell proliferation at the tumour–-stroma interface was observed which outnumbered the corresponding rate of apoptosis by far, the enhanced cell proliferation at the tumour border seems to be a main factor for tumour growth. They also found a significant correlation between the apoptotic index and the degree of tumour cell differentiation, indicating that a high rate of apoptosis coincides with a high level of tumour cell differentiation. In the same time they found the up-regulation of Fas expression in laryngeal carcinoma seems to have a stimulatory effect on the immune cell infiltration of the stromal tissue and its expression level was coincident with the clinical staging and the degree of damage. Kim et al 19 stated that soluble Fas, soluble Fas ligand, and soluble MHC class I–-related chain A proteins although deposited at the primary tumor site, these secreted factors could extend immunosuppressive effects into the local lymph nodes and the spleen, promoting invasion and metastasis. They also found these proteins are secreted mainly by T-Lymphocyte, Macrophage, endothelial cell and cancer cells.
The mechanisms of the interplay between lymphocytes and tumor cells were further elucidated by the identification of tumor antigens by T lymphocytes 20 and the molecular mechanisms of the natural killer (NK) cell. 21 In brief, cytotoxic T lymphocytes (CTLs) can recognize tumor-specific antigens restricted by major histocompatibility complex (MHC) molecules and kill tumor cells. In addition, tumor cells that lack the expression of one or more MHC class I alleles become targets for NK-mediation of the cell lysis. 22
LM examination of buffy coat revealed massive extent of the apoptotic cells in group III when compared to group I and II and EM examination revealed that the apoptotic changes are mainly in the PBMNCs.
Our results can be explained by Das et al 16 and Shimonish et al. 17 who found a significant increase of Fas receptors on the immune cells in laryngeal carcinoma. Also Zhang et al 23 reported that the Fas/FasLG pathway participate in the immunosuppression process observed in head and neck cancer via loss or mutation of its receptors on tumour cells or might be due to an inhibition of intracellular Fas signal transduction, which represents a frequent strategy of tumor cells to escape Fas-mediated apoptosis. Conforming with our results Zou 24 and Whiteside 25 who stated that cancer cells can grow by escaping from the attack of immune cells, thus, disrupting the host immune system, which is progressively suppressed as a result of tumor progression and metastasis.
Our data is in agreement with Elliott et al 15 who suggest that the Fas/FasLG pathway may play an important role in the development and progression of SCCHN because cancer cells become refractory to this regulatory signal and thus do not undergo apoptosis under appropriate conditions.
In conclusion, this study may help us to better understand one of the escape mechanisms in cancer larynx. This mechanism is represented by the significant increase in both the serum level of sFas and the morphological apoptotic changes that detected in PBMNCs in malignant cases. Also, sFas can be used as an attractive target for anticancer therapy and may be considered as a marker of disease progression and poor prognosis in laryngeal cancer.
Disclosure
The authors report no conflicts of interest.