
Abstract
Background
Invasive fungal rhinosinusitis is an uncommon disease with high mortality rates. There is currently no consensus on the best treatment timing. We studied the impact of the treatment timing on the survival of patients experiencing invasive fungal rhinosinusitis.
Methods
We conducted a retrospective study of patients suffering from invasive fungal rhinosinusitis. The duration of symptoms, clinical presentations, clinical signs, diagnoses, treatments, and outcomes were collected.
Results
It was observed that more than 70% of the mortalities occurred within the subgroup of patients who exhibited symptoms of the disease within 14 days before admission.
After adjusting for the confounders, the time taken to treat the patients was the most statistically significant predictor for mortality (P = 0.045). We found no significant relationships between mortality and its significant covariates, which included the underlying diseases (P = 0.91) or complications (P = 0.55).
Conclusions
Our study demonstrates that the time taken to treat the patients is an important determinant for the survival of patients who are afflicted with invasive fungal rhinosinusitis. The appropriate treatments should be administered within 14 days from the time the symptoms begin to manifest.
Introduction
Invasive fungal rhinosinusitis is an uncommon disease with high mortality rates. Up to 80% of invasive fungal rhinosinusitis patients experienced death or further morbidities after the treatment of the disease was completed (ranging from 20 to 80%).1–3 The aggressive and progressive nature of the disease necessitates that diagnosis and treatment must occur rapidly. The histologic evidence of fungi in hyphal forms invading the sinus mucosa and beyond, such as the submucosa, the blood vessels, or the bone, was needed to make the diagnosis of invasive fungal rhinosinusitis. The standard treatment usually comprises surgical debridement and anti-fungal therapy.
Invasive fungal rhinosinusitis can be subdivided into acute and chronic invasive fungal rhinosinusitis. Some authors created a further subdivision within chronic invasive fungal rhinosinusitis by defining certain cases as granulomatous invasive fungal rhinosinusitis;4,5 however, the pathological distinction between chronic and granulomatous invasive fungal rhinosinusitis does not change the management of the disease.
The pathogenesis of acute invasive fungal rhinosinusitis was from the aggressive pathogenic fungi in the nasal or sinus cavities invading the mucosa. The fungal cells can spread to surrounding structures such as the eyes and the brain via the blood vessels. The histology of acute invasive fungal rhinosinusitis usually shows that it is a highly necrotic, abundantly neutrophilic and angiotrophic process.6,7 Acute invasive fungal rhinosinusitis is classified differently from chronic invasive fungal rhinosinusitis, with a period of less than 4 weeks separating the two types of diseases. 8 Chronic invasive fungal rhinosinusitis results from a less aggressive spreading of the fungal cells, in comparison with acute invasive fungal rhinosinusitis. The histology usually consists of a low-grade mixed cellular infiltrate in affected tissues.6,7
The invasion of the fungi usually spreads beyond the sinus cavity into the orbit and the intracranial space. Orbital complications include preseptal cellulitis, orbital cellulitis, subperiosteal abscesses, and orbital abscesses. Intracranial complications include epidural or subdural abscesses, brain abscesses, meningitis, encephalitis, and cavernous sinus thrombosis.
The diagnosis of invasive fungal rhinosinusitis is usually delayed because the detection of fungal cultures or pathological results requires a few days to a few weeks to complete. Therefore, the presentations and the clinical findings obtained from the patients are important determinants. An early detection of fungal invasion will allow for better management and better prognosis for the patient.
There was no consensus on the best treatment timing. We studied the impact of the treatment timing on survival of the patients with invasive fungal rhinosinusitis. We hypothesize that an earlier treatment would be associated with improved survival. This study could also be useful for the rhinosinusitis workgroups to work with.
Methods
Study design and setting
We retrospectively reviewed a cohort of patients afflicted with invasive fungal rhinosinusitis. Data spanning a period of 11 years were extracted from the university hospital database (1997–2008). This hospital is the most prominent university hospital in the northeastern region of Thailand. Most patients suffering from invasive fungal rhinosinusitis were referred to our hospital.
Case definition
Rhinosinusitis was defined as an inflammation of the nasal cavities and the paranasal sinuses and is characterized by two or more symptoms, which should be a nasal blockage, an obstruction, a congestion, or a discharge (anterior/posterior nasal drip), which may have accompanying facial pain/pressure and reduction, or loss, in the sense of smell. These symptoms should be supported by a demonstrable disease that includes any of the following observations: endoscopic signs of nasal polyps, mucopurulent discharge primarily from the middle meatus, edema/mucosal obstruction primarily in the middle meatus, or imaging of mucosal changes within the ostiomeatal complex and/or sinuses.9,10
Invasive fungal rhinosinusitis was defined as the pathological results indicating the invasion of fungi into the nasal mucosa, sinus mucosa, or deeper tissues.
Data collection
We collected the data from our rhinosinusitis registry, outpatient department cards, and admission records. The duration of symptoms, clinical presentation, clinical signs, diagnoses, treatments, and treatment outcomes were noted in a standardized checklist.
Statistical analysis
The categorical variables were presented in the form of frequencies and percentages. The association between categorical variables was assessed using the chi-square test. The continuous variables were presented in the form of means. The Cox proportional hazards regression was used to adjust for potential confounding in the association between time to treatment and in-hospital mortality. We considered underlying diseases and complications as potential covariates, with a P value of less than 0.05 being considered statistically significant. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS Inc., Chicago, IL) software program, Version 20.0.
Ethics
The Khon Kaen University Ethics Committee for Human Research approved this project before it was initiated.
Results
From 1997 to 2008, 59 patients were diagnosed with invasive fungal rhinosinusitis. Forty-five patients suffered from acute invasive fungal rhinosinusitis, while the other 14 suffered from chronic invasive fungal rhinosinusitis (76.3 and 23.7%, respectively). The male and female proportion within the patients was not significantly different (26 male vs 33 female). The ages of the patients ranged from 16 to 78 years, with a mean age of 51.7 years. More than 60% of patients also suffered from diabetes mellitus as an underlying disease. Most of the 59 patients were found to have the fungi spreading beyond the nasal and sinus cavities (76.2%). The complications ranged from orbital cellulitis to cavernous sinus thrombosis (Table 1).
Baseline characteristics of patients.
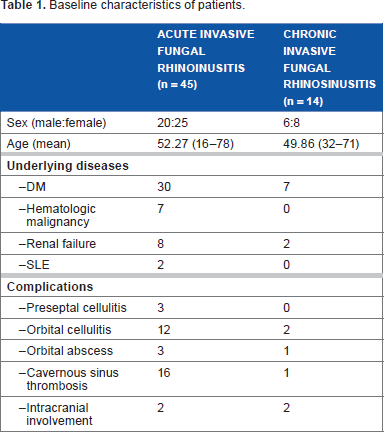
All patients received the standard treatment of endoscopic or external approach debridement and intravenous amphotericin B. One-third of the patients in the acute invasive fungal rhinosinusitis group did not survive the disease (31.1%), while all patients in the chronic invasive fungal rhinosinusitis group survived.
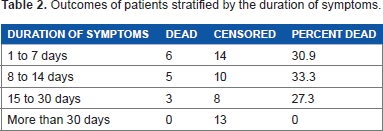
The majority of the events occurred within the subgroup of patients who exhibited symptoms of the disease within 14 days before admission. In the group of patients who exhibited the symptoms for 1–7 days before admission, 6 out of 20 patients did not survive (30%). In the group of patients who exhibited the symptoms for 8–14 days before admission, 5 out of 15 patients did not survive (33.3%), as is shown in Table 2.
Outcomes of patients stratified by the duration of symptoms.
The survival function graph analyzed the probabilities of surviving at any specific point in time. We found that the probability of survival decreased rapidly within the first 14 days (Fig. 1).
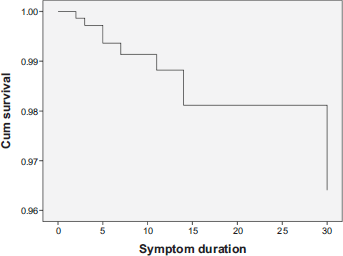
Survival function of invasive fungal rhinosinusitis patients.
After adjusting for the confounders in the Cox proportional hazards regression model, the time to treatment was the statistically significant predictor for mortality (P = 0.045). For the covariates, we found no relationship between the underlying diseases (P = 0.91) and complications (P = 0.55) as the significant covariates for mortality.
Discussion
Invasive fungal rhinosinusitis is a disease that is difficult to treat. Our recent studies11,12 and other reviews13,14 have found that invasive fungal rhinosinusitis can present itself with a wide variety of symptoms and signs. These different signs and symptoms make the initial diagnosis of the disease difficult. 12 A complete history taking, a knowledge of any underlying diseases (especially for patients who have their immunities compromised), a physical examination, and an awareness of these conditions will eventually lead to a diagnosis and rapid treatment of this aggressive disease.
However, the question of how prioritized the treatment should be has gone unanswered. We have usually regarded this disease as an urgent condition that needs aggressive surgical debridement and antifungal therapy, but there has not been any definitive cutoff point that has been suggested thus far.
We hypothesize that an earlier treatment would be associated with an improved survival rate. We examined the time taken to treat patients suffering from and their subsequent survival rates and found that the time taken to treat the patients was the most statistically significant predictor for mortality (P = 0.045). The cutoff point at 14 days should be used as the time frame where definitive treatment has to be conducted.
Other underlying diseases such as diabetes mellitus and immunocompromised diseases are also important factors that contribute to the mortality rate.11,12 Our results indicate that there was no statistically significant impact on the survival of patients when the underlying diseases were regarded as the covariate for the time taken to treat these patients. The lack of covariance could be explained by the characteristics of this cohort of patients, where the most common underlying disease was diabetes mellitus, which is a predisposing factor that is reversible and can be rapidly managed. Another explanation was a small sample size of patients because of the rarity of this disease. A large-scale multicenter study is necessary to address this problem.
Conclusions
Our study demonstrates that the time taken to treat patients suffering from invasive fungal rhinosinusitis is an important determinant in their outcome. Appropriate treatment should be administered within 14 days from the start of symptoms.
Author Contributions
Conceived and designed the experiments: PP, ST. Analyzed the data: PP. Wrote the first draft of the manuscript: PP. Contributed to the writing of the manuscript: PP, ST. Agree with manuscript results and conclusions: PP, ST. Jointly developed the structure and arguments for the paper: PP, ST. Made critical revisions and approved final version: PP, ST. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
The authors thank the staff and nurses at Srinagarind Hospital for their excellent care of the patients and Joel Yong for revision of the manuscript.