
Abstract
Background
Laryngopharyngeal reflux disease can present with a varied symptomatology because of the involvement of multiple sub-sites of the upper aero-digestive tract. It is a very common disease to be encountered in routine practice by both medical and ENT personnel. Its association with multiple pathologies including malignancy warrants an early diagnosis and management. The lack of cost effective and non-invasive tests constitutes a major hurdle in its early management.
Objectives
1. To define the “at risk” population, prone to developing laryngopharyngeal reflux. 2. To formulate major and minor risk factors for the clinical diagnosis of patients with laryngopharyngeal reflux. 3. To evaluate the efficacy of lifestyle management alone as a treatment option. 4. To formulate a treatment protocol for the management of patients and to prevent recurrence.
Study Design
We performed a prospective analysis of 234 patients diagnosed with laryngopharyngeal reflux. Patients were randomized into study and control groups based on the treatment protocol, using a computer generated randomization table and were single blinded to the type of therapy received. A complete analysis of the possible risk factors, symptoms, and signs was performed with statistical analysis.
Results and Conclusion
The data has helped us define the “at risk” population and formulate the criteria to diagnose cases of laryngopharyngeal reflux, clinically. The results emphasize the non-requirement of invasive or costly investigations for all patients and indicate the probable protocol to be followed prior to considering further investigation. The role of long term proton pump inhibitor treatment along with lifestyle modification in the initial phase of treatment, as mentioned in the literature, was re-confirmed by our study. However, in addition to the initial treatment, the study establishes the need for continuing lifestyle modification further for at least six months after the cessation of proton pump inhibitor therapy to prevent early recurrence of symptoms.
Background
In the recent past laryngopharyngeal reflux has been implicated as an etiological factor in multiple pathologies of the head and neck. The association of laryngopharyngeal reflux and gastroesophageal reflux disease (GERD) with patients of head and neck cancers in the range of about 62–67% has suggested its probable role in carcinogenesis also. 1 This makes the early diagnosis and management of the entity very critical. Koufman, in 1991, described laryngopharyngeal reflux as a separate entity 2 and till date no specific guidelines or treatment protocols have been formulated for its management. Although ambulatory 24 hour double-probe pH monitoring is currently considered the gold standard technique for the diagnosis of laryngopharyngeal reflux, it is far from being an ideal test, because the reported sensitivity of pH-metry is only in the range of 50–80%.3,4 The proportion of false-negative results can also be as high as 50%. 5 The high cost and invasive nature of the investigation, along with the lack of adequate sensitivity renders pH estimation, not cost effective in centers with high patient load. Unlike the classic GERD, the response to proton pump inhibitor therapy in the laryngopharyngeal reflux population is unpredictable and ranges from 60–98%. 6 So we conducted this study with the aim of defining the “at risk” population, formulating major and minor risk factors to aid in the diagnosis and testing the importance of lifestyle modification as a treatment option.
Materials and Methods
A prospective analysis of suspected laryngopharyngeal reflux patients presenting to our institution was performed between the periods of November 2006 and May 2008. After institutional ethical clearance, all patients who gave informed written consent were included in the study. The patients attending our outpatient department with three or more of the symptoms mentioned in the reflux symptom index 7 were recruited for the study. The scoring of the reflux symptom index was done by the patients and those having a severity score of higher than 13 were included in the study and those with a score less than 13 were excluded. 7 The patients after inclusion were randomized based on a computer generated randomization table.
Exclusion criteria for the study were patients already taking proton pump inhibitors or with history of rhinosinusitis, evident otological/sinonasal/psychological pathology, which can mimic the above mentioned symptoms.
Evaluation included detailed history with special focus on possible risk factors. Systemic examination was done to rule out any major pathology. Local examination of the nose, ear, oral cavity, oropharynx, and endolarynx was done. Clinical evaluation was supplemented by rigid endoscopy. The history, symptoms, and signs were noted and tabulated. Patients, if required, were further subjected to X-ray of paranasal sinuses, barium swallow, ultrasound of the abdomen and pelvis, and a psychological evaluation. Upper gastrointestinal endoscopy was limited to patients not responding to treatment (response score <2, less than 75% improvement).
Patients were randomly allocated into two groups as follows:
Group A–-in the study group, patients were treated with lifestyle modification and proton pump inhibitors (Omeprazole 20 mg twice daily).
Group B–-in the control group, patients were treated with lifestyle modification alone.
All patients were administered treatment for a total period of 90 days and also subjected to a detailed clinical evaluation at each visit.
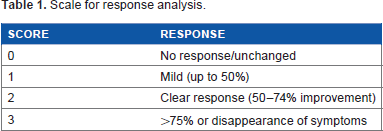
Follow up was done at 30, 60, and 90 days and the response of symptoms and signs to the treatment administered in both groups was noted at each visit as per the scale suggested by Woosuk Park et al 6 (Table 1). A response score of 0 suggested a response of less than 50% and such patients were considered non-responders and patients with a response score of 3 with greater than 75% improvement or disappearance of symptoms were considered to have good response. The follow up was continued for a period of six months after the cessation of medical therapy (62 patients with lifestyle modification and 55 patients without lifestyle modification) in the study group to detect the recurrence of symptoms. A reflux symptom index score of 13 or above was considered as a recurrence.
Scale for response analysis.
Observation and Results
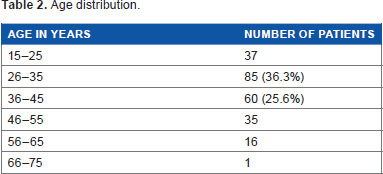
Out of 300 patients recruited for the study, 66 patients were lost to follow up or did not comply with the required guidelines of treatment and were excluded from the study. A total of 234 cases were divided into control and study groups. The age of the patients ranged from 16–68 years with an average age of 36.9 years, majority being female patients (119 patients) (Table 2 enumerates the age distribution).
Age distribution.
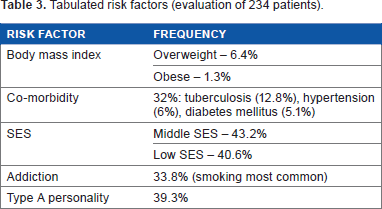
All the symptoms (Fig. 1) were analyzed by Chi square test and all the parameters were comparable in the control and study groups, excepting the symptoms of non-productive cough (P-value – 0.031) and pain in the throat (P-value – 0.018). The patient's risk factors were noted and tabulated (Table 3). Of the 75 patients with associated comorbidity, pulmonary tuberculosis (12.8%) was the most commonly associated followed by hypertension (6%) and diabetes mellitus (5.1%) (Table 4 depicts the signs noted on clinical evaluation).
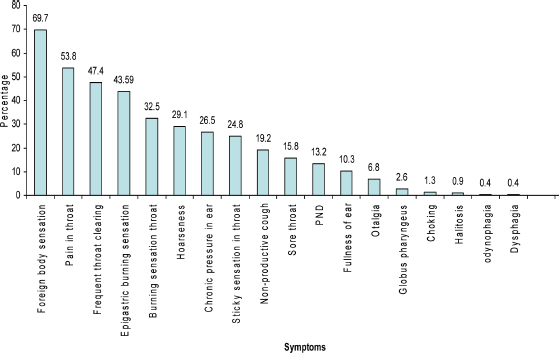
Bar diagram depicting the symptoms noted and their percentage (many patients had multiple symptoms).
Tabulated risk factors (evaluation of 234 patients).
Significant signs noted.
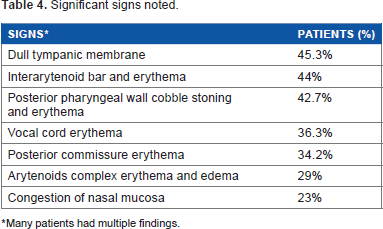
Many patients had multiple findings.
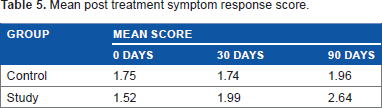
After the completion of treatment for three months the response score was noted for both the study and the control groups (Table 5). The average response score of the study group treated with proton pump inhibitors was better than that of the control group. On statistical analysis of the median with Mann-Whitney test, the difference was found to be statistically significant (P value – 0.009). Clinically, no significant difference was noted in the laryngeal, otological, and nasal signs pre and post treatment. Over all, 39 patients did not show significant improvement after treatment (response score
Mean post treatment symptom response score.
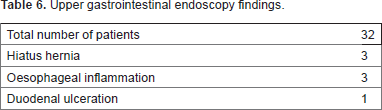
Upper gastrointestinal endoscopy findings.
Discussion
Laryngopharyngeal reflux signs and symptoms are caused by the noxious effects of gastric juices on the mucosal surfaces of the tracheobronchial tree, laryngopharynx, middle ear, and sinonasal complex. With the evolving research, laryngopharyngeal reflux has been implicated in many diseases, including malignancies. Regarding the gold standard investigation, the American Gastroenterological Association has taken the following position with regard to extraesophageal reflux: “There are presently no prospective data showing that ambulatory esophageal pH monitoring can identify either patients with laryngitis or asthmatics that are likely to respond to anti-reflux therapy”. 8 With the huge patient load and lack of cost effectiveness in available tests, a clinical diagnosis with a trial of medical management stands out as an effective option.
Increased prevalence of the disease was noted in the age group of 26–45 years (61.9 %), with decrease in prevalence in the extremes of the age range. The increased prevalence in the age group of 26–45 years, could signify the “at risk population”, in which one should have a high index of suspicion. In literature the most common symptoms were hoarseness (71%), cough (51%), globus (47%), and throat clearing (42%), 2 but in our study the common symptoms were foreign body sensation (69.7%), pain in throat (53.8%), and frequent throat clearing (47.4%). The possible cause for the difference in symptoms of presentation could be cultural and social differences. Although GERD has always been associated with increased body mass index, some studies showed no co-relation between isolated obesity and laryngopharyngeal reflux. 9 Our study confirms and reinforces this thought. The occurrence of laryngopharyngeal reflux mainly in the low and medium socio economic status (Modified Kuppuswamy's Socioeconomic Status Scale) as opposed to the GERD population, justifies our search for disease specific risk factors. Our evaluation of risk factors suggests addiction, co-morbid illness, and Type A personality to be factors of importance. Although physical findings are important in diagnosing the disease, in our study only 103 (44.02%) patients had significant physical findings. This is supported in literature by studies showing that physical findings do not corroborate with either the pretreatment or the post treatment symptom status. 10 So though one can look for findings, one should also be aware that they are neither sensitive nor specific indicators of diagnosis or response to treatment. Animal 11 and pediatric studies 12 have shown the presence of pepsin in middle ear effusion, suggesting a possible association between laryngopharyngeal reflux and pathogenesis of otitis media with effusion due to recurrent exposure of the Eustachian tube to acid reflux. In our study, dull tympanic membrane was the most common finding seen in 45.3% of patients, suggesting it as a probable early indicator to diagnosis, significance of which needs to be further evaluated.
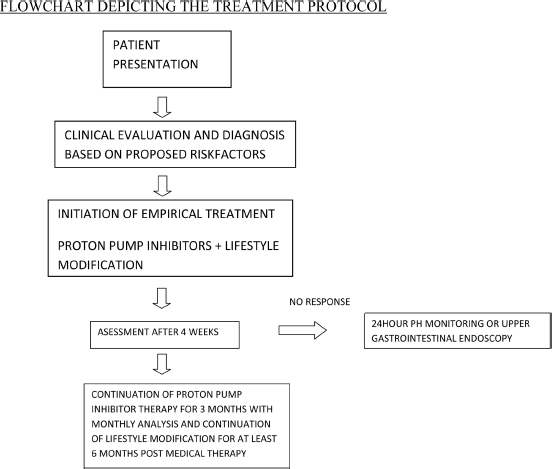
The treatment followed by us was as suggested by studies in literature. 13 We had a response rate of 86.3% (>2 or 3 score after 90 days of treatment), which is at par with the expected results. The high rates of recurrence of symptoms in patients not complying with lifestyle modification suggest the importance of continuing lifestyle modification for at least six months post proton pump inhibitor treatment. The proton pump inhibitors take time to produce significant relief and should be continued at least for three months as in our study. The detection of pathologies on upper gastrointestinal endoscopy implicates the grey area of interception where one can misdiagnose a GERD as a laryngopharyngeal reflux. The patients detected to have pathologies were accordingly managed by the gastroenterologists of our institution. We suggest an early endoscopy in patients with non-response to conventional management. Even though the results of upper gastrointestinal endoscopy are not statistically significant, one should have a very low threshold to fall back on upper gastrointestinal endoscopy in case of any doubt about the diagnosis.
Conclusion
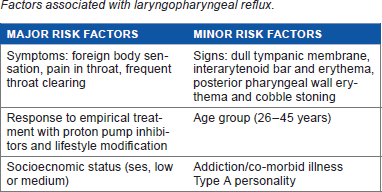
There is a need to categorize the at risk population that can be treated empirically. The invasive and costly tests should be restricted to the population that is not at risk, but are highly suspicious of having laryngopharyngeal reflux. Even though proton pump inhibitors and lifestyle modification are universally accepted modes of management for laryngopharyngeal reflux patients, lifestyle modification should not be used as a single modality of treatment in medically untreated cases of laryngopharyngeal reflux. We propose that lifestyle modification needs to be continued for at least six months post medical therapy to prevent recurrence. We suggest an early endoscopy in patients with no response to conventional management. We propose the following risk factors and treatment protocol based on our finding. Owing to the probable social and cultural differences, we emphasize the need for further long-term trails to confirm its efficacy universally.
Factors associated with laryngopharyngeal reflux.
Abbreviations
LPR, laryngopharyngeal reflux; PPI, proton pump inhibitor; GERD, gastroesophageal reflux disease; OPD, out patient department; OME, otitis media with effusion; UGIE, upper gastrointestinal endoscopy; SES, socio-economic status.
Author Contributions
Conceived and designed the experiments: RCD, RK, PC, AS. Analyzed the data: PC, RK, VC, RCD. Wrote the first draft of the manuscript: PC. Contributed to the writing of the manuscript: RK, KS. Agree with manuscript results and conclusions: PC, RK, RCD, VC, AS, KS. Jointly developed the structure and arguments for the paper: PC, RK, RCD, VC, AS, KS. Made critical revisions and approved final version: RK. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.