
Abstract
Background
The controversial roles played by major adipocytokines such as resistin, leptin and adiponectin in obesity and insulin resistance were extensively studied. This study aims to explore for the first time the possible effect of a family history of type 2 diabetes mellitus and smoking on non-diabetic individuals and associations to other metabolic parameters.
Results
In females there were significantly lower adiponectin levels among those with family history compared to those without (p 0.045); BMI and family history of type 2 diabetes contributed significantly to adiponectin levels with 43.7% variance (r 2 19.1; p 0.018). In males there was a significant decrease in resistin levels of those with smoking history (p 0.05). Linear regression showed a correlation between log resistin and LDL, and ApoA1 in all subjects (p-values 007, 0.0009 and R 2 0.12, 0.08 respectively).
Conclusion
This study showed for the first time that among the three adipocytokines, adiponectin was the only one to exhibit variations in females alone with regard to a family history of type 2 diabetes; the rest were independent of smoking. This study supports the view that adiponectin is a potential risk marker for type 2 diabetes.
Background
Adipose tissue is known to produce a vast array of adipocyte-derived factors, known as adipoctyokines. Although under normal conditions adipocytokines may play an influential role in energy homeostasis, triglyceride storage and the mobilization of fat, these processes can be substantially deregulated when adiposity increases specifically central adiposity.
Resistin belongs to a family of secreted peptides (Lee et al. 2003; Gerber et al. 2005) which share a cysteine-rich COOH-terminus and form disulfide-linked homodimers (Steppan et al. 2001). Resistin was identified in the mouse by screening differentiated adipocytes for genes repressed by the antidiabetic drug rosiglitazone, a member of the class of insulin-sensitizing drugs known as thiazolidinediones (TZDs), which are thought to target peroxisome proliferator-activated receptors (PPAR)-γ. Mouse resistin is expressed exclusively in adipocytes (Heilbronn et al. 2004; Utzschneider et al. 2005) and inhibits their differentiation in culture. Circulating levels of resistin are increased after high-carbohydrate meals (Utzschneider et al. 2005) and in genetically and diet-induced obesity (Heilbronn et al. 2004). In mice fed with a high-fat diet, anti-resistin antibodies improved blood glucose and insulin action (Heilbronn et al. 2004). Human resistin is expressed only at low levels in adipose tissue (Arner, 2005; Chen et al. 2005), and its contribution to these disease states is unclear.
Adiponectin, the gene product of the adipose most abundant gene transcript 1 (apM1) (Maeda et al. 1996) is in contrast a protein produced exclusively by adipocytes known to have putative insulin sensitizing and anti-atherogenic properties (Shand et al. 2003). It has been suggested that adiponectin may function as an adipostat in regulating energy balance and that its deficiency may contribute to the development of obesity and type 2 diabetes mellitus (Bajaj et al. 2004). Its low serum levels have been shown to be associated with peripheral insulin resistance and laboratory manifestations of the metabolic syndrome, while elevated levels are associated with insulin sensitivity (Bajaj et al. 2004; Weyer et al. 2001).
Lastly, we have leptin. This has been reported to increase energy expenditure and reduce adiposity in leptin-deficient states (Degawa-Yamauchi et al. 2003; Silha et al. 2003). It is thought to be an important link between nutrition and reproductions, acting as a signal from adipose tissue that adequate nutritional store are available to support reproductive function (Silha et al. 2003). It also appears to have effects on pancreatic ß-cell function and may be important in regulating insulin sensitivity (Koebnick et al. 2006). Correlations between leptin and insulin sensitivity have been documented (Kusminski et al. 2005; Yannakoulia et al. 2003).
Given the above established effects of these major adipocytokines on obesity and type 2 diabetes mellitus we aimed to correlate, for the first time, the effects of their serum levels on other major risk factors such as a family history of type 2 diabetes, personal smoking history and other metabolic parameters in a non-diabetic Saudi population, owing to the growing prevalence of diseases related to these conditions in the Kingdom of Saudi Arabia.
Methods
Ninety male subjects (BMI 27.03 ± 5.2) and sixty-seven female (BMI 28.76 ± 7.02) non-diabetics were recruited from the primary care of King Abdul-Aziz University Hospital to be included in this cross-sectional study.
Subjects were evaluated at the initial screening visit, which involved a full medical history and physical examination including blood pressure, weight and height. Blood pressure was measured twice using a standardized mercurial sphygmomanometer; the mean of the two readings was recorded. BMI was calculated as weight in kilograms divided by height in squared meters. Subjects were excluded if they are known type 2 diabetics, had personal history of cardiovascular disease, stroke or transient ischemic attack, uncontrolled hypertension, liver disease, renal disease, severe dyslipidemia (triglycerides >600 mg/dl or cholesterol >350 mg/dl), or any other serious chronic disease requiring active treatment and diabetes. Written informed consent was provided by all participants before being enrolled in the study. The study was approved by the Human Ethical Review Committee of the Faculty of Medicine at King Khalid University Hospital, King Saud University Riyadh, Saudi Arabia.
Blood samples were obtained after an overnight fast (∼10 h) and sera were collected. Levels of glucose, triglycerides, HDL-cholesterol and total cholesterol were measured using a chemical analyzer (Konelab, Finland). LDL-cholesterol was calculated using the Friedewald equation (LDL-cholesterol = total cholesterol–-HDLc–-[triglycerides (in mmol/L)/2.17 or triglycerides (in mg/dL)/5]) (Wagner et al. 2000). Hormone concentrations were measured as follows: human adiponectin, resistin and leptin (Linco Research, St. Charles, MO); insulin was analyzed by a solid phase enzyme amplified sensitivity immunoassay (Medgenix INS-ELISA, Biosource, Belgium). To minimize variability, hormone levels were measured in one assay for all the subjects. HOMA-IR was calculated as the product of insulin (µIU/ml) and glucose (mmol/L) divided by 22.5 (Kanauchi et al. 2003).
Statistical Analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS for Windows, version 10). Variables which exhibited a positive skew were log transformed in order to normalize the distribution. Groups were compared by a student's unpaired t-test or, if not normally distributed, by the Mann-Whitney U test. Multiple regression analysis was performed to determine relationships between the variables of interest.
Results
Table 1 summarizes the anthropometric, clinical and metabolic parameters of the 157 adult Saudi patients enrolled in this cross-sectional study. They were divided into two groups: Males (N = 90, age 35.29 ± 14.37, BMI 27.03 ± 5.20) and females (N = 67, age 32.78 ± 13.13, BMI 28.76 ± 7.02), and were further categorized under those with family history of type 2 diabetes (Male = 49, Female = 40), and those without (Male = 35, Female = 25). Males had significantly higher values in terms of systolic blood pressure, glucose, triglycerides, insulin resistance, and insulin (p-values 0.02, 0.001, 0.005, 0.001, and 0.009 respectively) than females. However, females had statistically higher values than males with respect to their levels of leptin, adiponectin, HDL-cholesterol and resistin (p-values 0.002 and 0.0001 respectively).
Clinical characteristic and metabolic parameters of male and female subjects.
Data presented as mean (SD) except with
as mean (range);
p-value ≤0.05;
p-value < 0.001.
The rest of the metabolic characteristics had no significant differences from one another.
Table 2 shows the comparison of clinical characteristics in the presence of family history of diabetes. All variables were comparable and did not differ significantly from one another.
Clinical characteristic and metabolic parameter of subjects with and without family history of type 2 diabetes.

Data presented as mean (SD) except with
as mean (range); no significant differences were elicited.
A total of 89 (56.7%) subjects, 49 (31.2%) males and 40 (25.5%) females had a family history of diabetes, which was defined as having diabetes mellitus been diagnosed in any first-degree relative. 20 of the participants were smokers and all these were male. From these data we further investigated the impact a family history of type 2 diabetes on the levels of resistin, adiponectin and leptin in both sexes; while the effect of smoking history on adipocytokines was confined to male subjects only. Adipocytokine levels in males were not significantly different with one another regardless of the presence or absence of family history of type 2 diabetes mellitus (Table 3). However, the results showed that in females, there is a significantly lower adiponectin levels among those with a family history of type 2 diabetes than in those without (p-value 0.045) as shown in Table 4. It is noteworthy that in males there is a significant decrease in the resistin levels of smokers compared to non-smokers (p-value 0.05) as shown in Table 5.
Adipocytokine levels of male subjects with and without family history of type 2 diabetes.

Data presented as mean (range); no significant differences were elicited.
Adipocytokine levels of female subjects with and without family history of type 2 diabetes.

Data presented as mean (range);
p-value ≤ 0.05.
Adipocytokine levels of male subjects with and without smoking history.

Data presented as mean (range);
p-value ≤ 0.05.
Linear regression showed a correlation between log resistin and LDL-cholesterol, and ApoA1 in all subjects (p-values 0.007, 0.0009 and R 2 0.12, 0.08 respectively). Stepwise regression analysis was done using the different adipocytokines as dependent variables and known indicators such as BMI, HDL-cholesterol, triglycerides, insulin resistance, smoking and family history of type 2 diabetes as independent variables. In males, smoking history and HDL-cholesterol levels are the significant predictors for resistin (r 2 = 0.27; p < 0.001) with 47.7% of the variance perceived; for both leptin and adiponectin, BMI was the sole significant predictor (r 2 0.22, 0.06; p < 0.001, 0.025 respectively) with 47.1% and 25.1% variances respectively (not shown in Table).
Moving on to females, BMI and family history of type 2 diabetes contributed significantly to adiponectin levels with 43.7% variance (r 2 19.1; p 0.018). No significant predictors were elicited using resistin and leptin as dependent variables (not shown in Table).
In stepwise regression, we found a significant association between log resistin and LDL-cholesterol and diastolic blood pressure (P-value 0.000 and R 2 0.33) in all subjects. In females, however, only LDL-cholesterol was significantly associated with log resistin (p-value 0.001 and R 2 0.28), whereas in males, HDL-cholesterol, ApoB, diastolic blood pressure and smoking are associated with log resistin (p-value 0.0001 and R 2 0.54) (not shown in Table).
We then evaluated the effect of resistin on selected lipids, as presented in Figures 1 and 2; linear regression showed a correlation between log resistin and LDL, and ApoA1 in all subjects (p-values 0.007, 0.0009 and R 2 0.12, 0.08 respectively) (Fig. 1 and 2).

Inverse correlation between Log resistin and LDL-cholesterol.
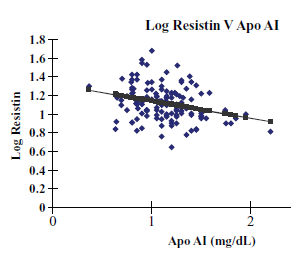
Inverse correlation between Log resistin and Apo AI.
Discussion
This is probably the first, or at least one of the first, human studies to specifically document the effect of a family history of type 2 diabetes on levels of selected adipocytokines which include resistin, leptin and adiponectin. Based on the still-evolving theory that these adipocytokines are linked to obesity and diabetes mellitus, we hypothesized that people who are genetically predisposed to develop such diseases may have significantly different levels of these adipocytokines from those without such a family history.
In a study by Jansson and his colleagues, they observed near-significant higher circulating leptin levels in men who are genetically predisposed to develop type 2 diabetes mellitus than in well-matched control subjects (Jansson et al. 2002). This supports our findings, which show higher serum leptin levels in both males and females with a family history of type 2 diabetes though these did not reach statistical significance either.
Unfortunately, there is little information available on the circulating levels of resistin among people who are most likely to inherit type 2 diabetes mellitus. To our knowledge, this is the first study to document the effect of a family history of type 2 diabetes and smoking on resistin levels among men. We were able to elicit a significant effect of a family history of type 2 diabetes on male subjects (but not on females) (P-values 0.19 and 0.49) and we found a decreased level of resistin in males with history of smoking (p-value 0.05. With respect to a gender difference in serum resistin levels, this study confirms the findings of Yannakoulia et al. (Yannakoulia et al. 2003), who also found significantly higher resistin levels in females than in males but at the same time refutes the findings of Stejskal et al. who found no correlation between serum resistin and gender (Stejskal et al. 2002).
One of the highlights of this research is that there was significant correlation of serum resistin to HDL-cholesterol and smoking history which is incompatible with many reviews of the unclear status of resistin towards lipids (Farvid et al. 2005; Bloomgarden, 2002). Resistin is arguably elevated in obese as opposed to lean subjects (Degawa-Yamauchi et al. 2003) and the serum resistin is not a significant predictor of insulin resistance in humans (Rea and Donnelly, 2004) and nor are adiposity, blood pressure and most lipid profiles, as shown in previous reports (Chen et al. 2005). Our results also show decreased and significant levels of resistin to males exposed to smoking, which refutes the finding that resistin is elevated in subjects exposed to oxidative stress (Bo et al. 2007). Although there is high discrepancy, these differences may be attributed to the diverse expressions and translations of the resistin gene which greatly affect its secretory rates, not to mention the different methodological limitations which can result either in variations among serum concentrations, or may simply indicate that resistin has no role at all in obesity and the lipids (Kusminski et al. 2005). It is noteworthy, however, that type 2 diabetes mellitus, which has a strong propensity to be inherited, was found to be closely associated with the G/G genotype of a resistin single nucleotide polymorphism at –420, the primary variant determining type 2 diabetes susceptibility (Osawa et al. 2004).
Adiponectin in contrast, also one of the novel hormones of the white adipose tissue, was found in our study to be significantly decreased only in females with a family history of type 2 diabetes (P-value 0.045). This confirms the findings of Behre and his colleagues in their recent report, which concludes that a family history of type 2 diabetes is associated with hypoadiponectinemia independent of obesity, glycemia, and insulin sensitivity and that its statistically significant difference remains the same even after adjusting for BMI, WHR, C-peptide, HOMA-IR, CRP and glycemia (Behre et al. 2006). Their study however did not include other significant adipocytokines such as leptin and resistin, which is included in this study. Adiponectin among women is cross-sectionally proven to be associated with estrogens, androgens, sex hormone binding globulin (SHBG), prolactin, c-peptide, and insulin-like growth factor-1 (IGF-1), hormones which influence insulin resistance, which probably explains why the significant effect of a genetic predisposition to develop type 2 diabetes was more pronounced to female subjects (Tworoger et al. 2007). Furthermore, the variability of adiponectin in our subjects with a family history of type 2 diabetes can be partly but not fully explained by the following: that adiponectin is known to be inversely related to insulin resistance; that a single nucleotide polymorphisms of the adiponectin gene was found to be associated with IGT and hypoadiponectinemia (Gonzales-Sanchez et al. 2005); and that mutations in the adiponectin gene served as a common background for the development of metabolic syndrome and coronary artery disease (Ohashi et al. 2004) but not in every case (Salmenniemi et al. 2005).
Adiponectin, with the rest of the adipocytokines emphasized in this research, did not show a statistical difference in terms of the level found in male smokers. Other studies however, reveal a close association of hypoadiponectinemia with smoking in men (Iwashima et al. 2005; Kim et al. 2006).
The authors acknowledge some limitations. The absence of female subjects with smoking history in this study denotes that the significant difference in resistin levels apply only to male subjects. Waist-hip ratio which is a surrogate marker for visceral obesity and is more associated to the adipocytokines measured was not included in this study as well as environmental factors such as diet and physical activity since the study was more focused on the genetic predisposition to develop type 2 diabetes and its association to adipocytokines rather than the mentioned variables which are already proven to influence adipocytokines. Lastly, the cross-sectional design of the study makes it difficult to make a causal inference as to whether the subjects will eventually develop type 2 diabetes. Further studies are definitely required in a larger population and in a prospective approach to confirm current findings.
In summary, adiponectin is the only adipocytokine to exhibit alterations in levels among healthy female patients with a family history of diabetes. Resistin and leptin did not show association in terms of a family history of diabetes and the levels of all three hormones were independent of smoking. Screening for patients at risk of diabetes is a major logistical challenge. For identification purposes, current studies suggest adiponectin as a suitable marker for the risk of diabetes.
Conclusion
This research on non-diabetic subjects revealed that serum adiponectin is the only adipocytokine to exhibit variations in non-diabetic females alone, with regard to a family history of type 2 diabetes, and that serum resistin levels are significantly decreased in male subjects with smoking history. Additional investigation on a larger scale and in a prospective approach is definitely needed to check the probability that these major adipocytokines may reveal an effect if conducted among a wider population.
Footnotes
Acknowledgements
The authors acknowledge: the trusted staff of the research unit in the Diabetic Center, King Abdul-Aziz Hospital, for their help in the sampling and data collection; the research center of King Saud University (project no. Bio/24-25/14) for the generous funding; and Dr. Shaun Louie Sabico for his support in the statistical analysis and his contributions to the overall outcome of this study.