
Abstract
Aim
To compare the effect of different treatment regimens (oral hypoglycemic agents [OHGs], insulin therapy, and combination of both) on glycemic control and other cardiometabolic risk factors in type 2 diabetes mellitus (T2DM) patients in Saudi.
Subjects and Methods
Patients with T2DM, but no serious diabetic complications, were randomly recruited from the diabetes clinics at two large hospitals in Jeddah, Saudi Arabia, during June 2013 to July 2014. Only those without change in treatment modality for the last 18 months were included. Blood pressure and anthropometric measurements were measured. Treatment plan was recorded from the patients' files. Fasting blood sample was obtained to measure glucose, HbA1c, and lipid profile.
Results
A total of 197 patients were recruited; 41.1% were men and 58.9% were women. The mean (±SD) age was 58.5 ± 10.5 years. Most patients (60.7%) were on OHGs, 11.5% on insulin therapy, and 27.7% were using a combination of insulin and OHGs. The mean HbA1c was lower in patients using OHGs only, compared with means in those using insulin, or combined therapy in patients with disease duration of #10 years (P = 0.001) and also in those with a longer duration of the disease (P < 0.001). A lower mean diastolic and systolic blood pressure was found among patients on insulin alone (P < 0.01). No significant differences were found in lipid profiles among the groups.
Conclusion
Insulin therapy, without adequate diabetes education, fails to control hyperglycemia adequately in Saudi T2DM patients. There is a challenge to find out reasons for poor control and the ways as to how to improve glycemic control in T2DM.
Keywords
Introduction
Diabetes mellitus is “a complex chronic illness requiring continuous medical care with multifactorial risk reduction strategies beyond glycemic control”. 1 Type 2 diabetes mellitus (T2DM) occurs mainly due to insulin resistance in the peripheral tissue, which causes an increase in insulin secretion, and thus a state of hyperinsulinemia. 1 Diabetes has serious complications that can affect the patient's life quality. These complications include diabetic retinopathy, nephropathy, neuropathy, and cardiovascular disease. 2 Diabetes and its complications have increased the economic expenses at the level of health-care systems to cover the expenditure needed for hospital admissions and emergency care. 3 Effective glycemic control is the crucial element of diabetes management to limit the development of its macrovascular and microvascular complications and improve quality of life for the affected individuals.4,5 According to a diabetic care report published in January 2014, the aim of diabetes management is to keep the glycated hemoglobin (HbA1c) <7.0%, 2 preprandial capillary plasma glucose between 70 and 130 mg/dL, and peak postprandial capillary plasma glucose <180 mg/dL to prevent, or at least delay, further complications. 6 In addition to the American Diabetes Association (ADA) and the European Association for the Study of Diabetes position statement in 2012, the goal of diabetes control has individualized both treatment target and treatment strategies to each patient according to many factors. 7 If the patient is diabetic for a long time, 8 has limited life expectancy, severe hypoglycemic episodes, 9 advanced complications, or extensive comorbidities, the goal of HbA1c level was modified to 8%.3,4
In order to achieve optimal glycemic control, a multidisciplinary approach needs to be taken. This includes lifestyle modification (diet and exercise), which is the first line of management, followed by oral hypoglycemic agents (OHGs) and insulin therapy. OHGs are considered the mainstay of treatment and have been proven to achieve effective and early glycemic control, 10 with reduction of cardiovascular events. 4 Regardless of the usefulness of lifestyle modification and OHGs, the majority of patients will eventually need insulin, which has been reported to be superior to other modalities among patients with T2DM, to achieve adequate glycemic control. 11 However, patients' education and adherence to the treatment regimen are considered the cornerstone in diabetes management. A randomized clinical trial has shown improved outcome among patients undergoing pharmacotherapeutic care plan and diabetes education over the group receiving standard care. 12 The latest “Saudi National Reference For Diabetes Mellitus Guidelines In Primary Health Care” recommends the use of insulin in patients who are not able to reach HbA1c level of 7.0% with other treatment regimens. 13 Insulin will be made freely available in all primary health-care centers, leading to more physicians prescribing it. However, these guidelines were based on the American 1 and the Canadian Clinical Practice Guidelines 2013, 14 without any studies being conducted on the local population.
Therefore, we aimed to compare the effect of different treatment regimens (OHGs, insulin therapy, and combination of both) on glycemic control and other cardiometabolic risk factors in T2DM Saudi patients.
Methods
A cross-sectional study was conducted between the two centers. The study complied with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Committee on the Ethics of Human Research at the “Faculty of Medicine, King Abdulaziz University”, and the Committee on the Ethics of Medical Research at King Fahad Armed Forces Hospital (KFAFH). Patients diagnosed with T2DM were randomly recruited from the diabetes outpatient clinics during the course of 13 months (June 2013 to July 2014). Patients who were willing to participate were asked to sign an informed consent form before inclusion in the study. Exclusion criteria included: patients recently diagnosed with diabetes (less than one year period), patients on the same treatment regimens for less than six months, pregnancy, having any other severe chronic illness, or diabetic complications (ie, end-stage renal disease, liver disease, recent myocardial infarction, etc.). Anthropometric measurements were taken for all patients. Height was measured bare footed to the nearest 0.5 cm using a stationary stadiometer. Weight was measured to the nearest 0.5 kg, while wearing light street clothing using a portable calibrated scale (Omron BF511). Both measurements were used to calculate body mass index (BMI). Waist measurement was taken at the level of the umbilicus, and hip measurement at the maximal protrusion of the gluteal muscles, both to the nearest 0.5 cm. Blood pressure was measured following the recommendations of the Joint National Committee using a standard mercury sphygmomanometer with the cuff on the right upper arm. 15 Two blood pressure readings were taken, one minute apart, while the subject was seated for 10 minutes, and the mean of the two readings was calculated. BMI was used to classify patients as being normal (BMI = 18.5–<25), overweight (BMI = 25–<30), or obese (BMI ≤ 30). In addition, a questionnaire covering demographic information and the management plan followed by the patient was filled during face-to-face interview. Treatment plan was recorded as lifestyle modification (ie, diet and exercise), OHGs, insulin, or any combination of them. Fasting blood sample was obtained for the measurement of glucose and HbA1c. Glucose and HbA1c were estimated using automated enzymatic methods (Dimension Vista 1500T Intelligent Lab System from Siemens Company) at the biochemistry laboratory in the respective hospital. HbA1c < 7% was considered controlled and HbA1c > 7% was considered uncontrolled, in accordance to the ADA guidelines. 1
Data were entered, coded, and analyzed using SPSS version 20. One-way analysis of variance was used to test for differences between the means of different treatment groups. Chi-square test was used for categorical variables to test for differences between groups. All P-values <0.05 were deemed statistically significant.
Results
A total of 197 patients were recruited from both locations (41.1% were males and 58.9% were females). None of the patients were managed by lifestyle modification alone. Only 18.3% of the sample had adequate glycemic control. Almost half of the patients were hypertensive and the majority had dyslipidemia. High systolic blood pressure (SBP) was found in 33.0% of the patients, while 47.7% had high diastolic blood pressure (DBP). In addition, 78.7% of the patients had high LDL, and 31.0% and 51.3% had high triglycerides and low HDL, respectively. Characteristics of the study group are presented in Table 1.
Characteristics of the study group presented as mean ± SD or the number and percentage of total.

The majority (60.9%) of the patients used oral hypoglycemic agents (OHGs) only, in comparison with insulin alone (11.7%) and combined therapy (27.4%). There were no significant differences in the mean BMI and in the percentages of patients treated with statins or antihypertensive drugs among the different management groups (Table 2).
HbA1c, lipid profile, blood pressure (mean ± SD), and use of antihypertensive drugs and statins (% of total) in groups of patients using different management modalities according to duration of disease and use of statins and/or antihypertensive drugs.
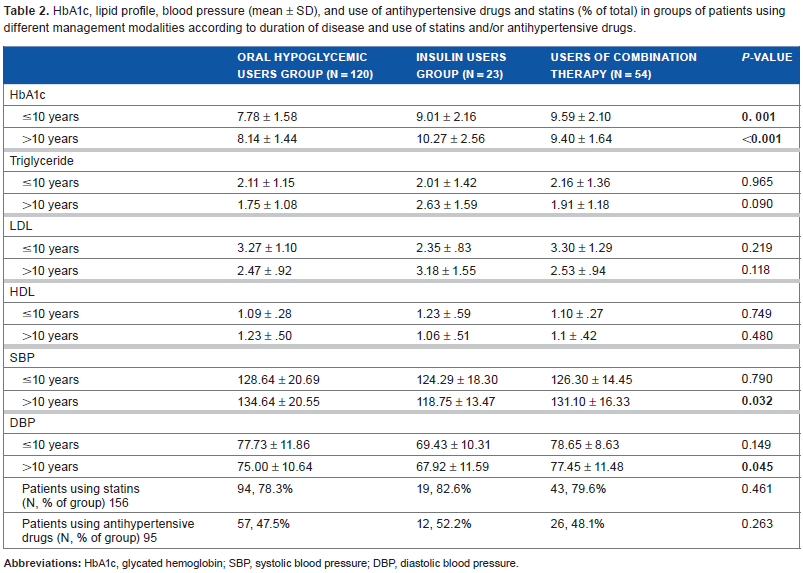
Even though the mean HbA1c was high in each patient group, there was a significant difference between the different management methods of DM. The mean HbA1c was lower in patients with disease duration of ≥10 years using OHGs only than in those using insulin or combined therapy (P = 0.001) and in those with longer duration of the disease (P = 0.001; Table 2).
We found no significant differences between the means of lipid profile components, namely, triglyceride, LDL, and HDL, among the different diabetes management groups (Table 2).
SBP and DBP were lower in patients with >10 years DM duration in the group taking insulin only (P = 0.032, and 0.045, respectively).
Discussion
In spite of various reports showing a better glycemic control in T2DM patients using insulin therapy alone, 16 or combined with OHGs,17–20 this was not noted in our study; the mean glycated hemoglobin was the highest among all management modalities. Patients with diabetes are advised and expected to follow an altered healthier lifestyle that could be different to what they are used to practice. This includes compliance to healthy diet, physical activity plans, and self-glucose monitoring. Such adjustments could be too complicated, and hence, not feasible to follow by many patients. Indeed, the fact that insulin did not improve glycemic control even in combination with OHGs might signify a lack of patients' awareness regarding self-management and compliance to therapy. Patients' awareness and their compliance to therapy were not assessed in this pilot study and need further investigations before firm conclusions are drawn about the reasons for the present findings.
In an earlier report, compliance to OHG treatment was reported to be higher than that to insulin, 21 but this issue has not been studied in Saudi Arabia so far. Multiple factors are involved in the compliance to insulin therapy, including interference with patient's daily activities and plans, immediate negative experience after insulin injection (pain and embarrassment), low income of patients, high insulin cost, 22 age of the patient, the frequency of hypoglycemic attacks or other side effects, and the complexity of management regimen (method of administration, number of injections/day, and duration of insulin use).22–25 Furthermore, the worry about hypoglycemia episodes may lead to patients eating more and decreasing the insulin dose that will eventually lead to worse glycemic control. 22 Indeed, a study conducted in 2005, in Eastern U.S., showed that diabetic patients use approximately 77% of insulin dose prescribed by the health-care providers, which could predispose patients to more frequent and severe hypoglycemia episodes as heath-care providers try to improve glycemic control by increasing the insulin dose. 26 Our future research in Saudi Arabia will attempt to cover all these points while investigating compliance among our patients, in the hope of better management of T2DM.
Several factors have been shown to be associated with improved compliance to insulin therapy. For example, insulin pen is significantly easier to use and less painful than the conventional vial/syringe, hence helping to improve compliance. 27 Furthermore, behavioral adherence and self-monitoring of blood glucose was correlated with a better glycemic control as the daily measurements of blood glucose act as a constant reminder for the patient to receive his therapeutic dose before getting his reading. 21
However, among all factors, active patient education, including lifestyle modification, has been proven to be the main determinant of adherence to therapy worldwide and leading to improved glycemic control. 12 A meta-analysis showed that lifestyle intervention was also associated with significantly improved cardiovascular risk factor levels including HbA1c, BMI, SBP, DBP, and to a better quality of life.28–32 Another meta-analysis concluded that diabetes self-management education results in improved clinical, lifestyle, and psychological outcomes. 33
In Saudi Arabia, a study conducted in 2005 in the Asir region investigated the availability of diabetes health educators and diabetes educational material, and reported that only for 8% of the patients, a diabetes educator and less than 50% diabetes education materials were available. 34 Another recent Saudi study showed a significant association between diabetes education and glycemic improvement. 35 Patients included in this study were actually part of a larger population recruited from medical centers in Egypt, Iran, Jordan, and Saudi Arabia in a multicenter, prospective observational study, aiming at examining whether individualized Pre-Ramadan education resulted in improved clinical outcomes and a safer fast for people with T2DM. 36 Patients from King Abdulaziz University Hospital received individualized teaching on the needed dietary and lifestyle adjustments, while those from KFAFH were given routine instructions. The noted improvement in the group receiving individualized teaching implies that the reasons for our findings of poor glycemic control in insulin users include a lack of compliance and inadequate knowledge of self-management. It also reflects the inadequacy of the present diabetes management system and indicates the urgent need for well-constructed, locally developed diabetes education programs in Saudi Arabia. The present system for the management of T2DM in the country does not result in adequate glycemic control, since insulin therapy either alone or combined OHGs are not superior to OHGs in achieving glycemic control. Education programs aiming at increasing patients' awareness about diabetes self-management, stressing the importance of compliance to insulin therapy, and the correct methods for its application, as well as information about the consequences of poor glycemic control, are highly recommended.
Admittedly, the sample size in our study was not large, mainly due to the exclusion criteria, and details of insulin therapy (whether conventional needles or insulin pins) were not taken. Nevertheless, we believe that our findings are of interest to treating physicians and endocrinologists and will help to lay down better Saudi guidelines for the management of T2DM based on local evidence rather than international recommendations. Our future work will aim at correcting the limitations in this study by increasing the sample size, taking more detailed information regarding insulin therapy, as well as assessing patients' knowledge regarding self-management.
Author Contributions
Conceived and designed the experiments: SMB, WA, MAsiri, ABA, MAhmed, KA, AH, and SB. Analyzed the data: WA, ABA, AB, AAlghamdi, GA. Wrote the first draft of the manuscript: WA, BA, RK, ABS, OB, and AAlamoudi. Contributed to the writing of the manuscript: MAsiri, AAljahdali, NA, HP, MB, SMB, GA, AB, and JT. Agree with manuscript results and conclusions: SMB, MAhmed, KA, SB, AAlhozali, and JT. Jointly developed the structure and arguments for the paper: WA, MAsiri, BA, RK, ABA, ABS, AAlamoudi, AAljahdali, OB, MB, NA, and SMB. Made critical revisions and approved final version: SMB and JT. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
We would like to thank all the following for their help while conducting our study: nurses who helped in selecting the appropriate patients and laboratory staff who performed the biochemical analysis.