
Abstract
Objectives
To investigate whether planned visits improve glycemic, blood pressure and lipid control among patients with type 2 diabetes mellitus (DM).
Methods
The study was conducted from July 2007 to February 2008 at a primary care clinic in Rancho Cordova, California. One hundred eighty-three patients were invited to come to a planned visit. On the day of the visit, they were provided a copy of their most recent test results and information on American Diabetes Association recommendations for A1C, lipid, and blood pressure control. Afterwards, they met with their physician for a 15-minute focused appointment. Finally, they met with a diabetic nurse educator. There was no subsequent contact with the nurse educator after the planned visit. We compared the baseline measurements to those from a follow-up visit with the primary care provider at a follow-up over a 6 month period. The comparison group in this study were those who did not accept the invitation for a planned visit. Their outcomes were monitored over the same time horizon.
Results
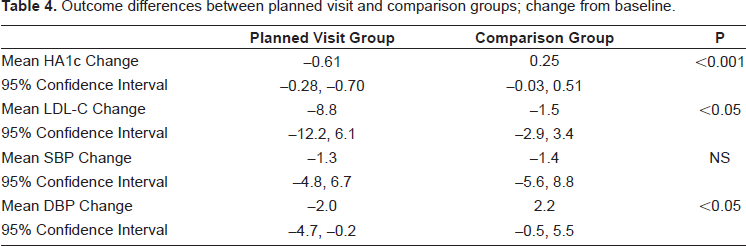
One hundred eighty-three patients attended one of a total of five planned visit sessions. There were 212 patients in the comparison group. There were no significant differences for the measured baseline characteristics. There were significant improvements in A1C, LDL-C, and diastolic blood pressure control in the planned visit group. The mean A1C change was –0.61% (95% confidence interval, –0.28, –0.70); P < 0.001). The mean LDL-C change was -8.8 mg/dL (95% confidence interval, –12.2, 6.1); P < 0.05. The mean diastolic blood pressure change was -2.0 mmHg (95% confidence interval, –4.7, 6.7); P < 0.05. Patients who participated in a planned visit also reported a significantly higher frequency of self-care behaviors and greater understanding about diabetes care.
Discussion
Planned visits led to improvements in glycemic, lipid and blood pressure control over a 6 month observation period. Patients attending planned visits also reported improvements in self-care behaviors and a greater understanding about diabetes care.
Introduction
Many patients with type 2 diabetes mellitus (DM) fail to receive care consistent with published guidelines. 1 Many of these patients have poor glycemic control and poor control of comorbid hypertension and hyperlipidemia. Primary care providers face many challenges in finding ways to deliver more effective care to these patients. What often gets in the way of focusing on optimal diabetes care has been called the “tyranny of the urgent.” 2 Specifically, multiple competing agendas of the patient and provider impair chronic care efforts. As stated by Bodenheimer, “given the demands of acute, chronic, and preventive services, the provision of consistent, high-quality, guideline-compliant care in a 15-minute visit is beyond the reach of most primary care physicians, however, well trained and well intentioned they may be.” 3 One method to deal with these competing agendas is the planned visit. 4 The planned visit is an appointment with one agenda; the management of the patient's chronic condition. This study investigated the impact of planned visits in a primary care practice.
Patients and Methods
Subjects
The study was conducted from July 2007 to February 2008 at the UC Davis Health System Primary Care Clinic in Rancho Cordova, California. The Rancho Cordova Clinic is one of eleven primary care practice sites within the UC Davis Health System. There are six primary care physicians at this facility who provide approximately 15,000 office visits each year. One hundred eighty-three patients with DM were identified from an electronic registry. Eligible participants were 35 to 77 years old, had type 2 DM, were designated as receiving their primary care at this facility, and had not had a specific appointment for their DM in the previous year. Patients who had transferred their care to a primary care provider at another facility were excluded.
Study design
The patients were invited by a letter from their primary care provider to come to a planned visit to discuss their DM care. The clinic staff instructed the patients who called for an appointment to obtain a baseline glycosylated hemoglobin (A1C) and lipid profile prior to the planned visit. On the day of the planned visit, the staff provided the physician with a copy of these test results which were to be handed to each patient. The results included information on the American Diabetes Association (ADA) recommendations for A1C, blood pressure, and lipid control. Patients then met with their physician for a 15-minute focused appointment for diabetes. The physicians were not prompted to follow any specific guideline for medication therapy or asked to consider a more intensive regimen. After the encounter was concluded, the patients met with a diabetic nurse educator. This encounter lasted approximately 45 minutes. The nurse educator reinforced the ADA recommendations, discussed healthy eating, stress reduction, and led a discussion on how to develop an action plan for a health behavior change. There was no subsequent contact with the diabetic nurse educator after the planned visit. Physicians followed-up with their patients in their usual course of practice. The practice standard was to recommend a follow-up appointment in 3 to 6 months. We collected baseline data on A1C, blood pressure, and lipid profile, at the time of the planned visit. We extracted this information from follow-up visits with the primary care provider from the electronic medical record over a 6 month time span.
Comparison group
The comparison group in this study were those who did not accept the invitation for the planned visit. Members of this group met the same eligibility criteria as those who attended a planned visit and had outcomes available over the study's longitudinal horizon.
Outcomes
The primary outcomes were glycemic control, blood pressure, and LDL-cholesterol (LDL-C) measured during the 6 month period after the planned visit. Patient's DM medication regimens were catalogued during the study period. We also assessed patient's reporting of self-care activities and knowledge of DM through the use of a survey (Appendix A).
Survey overview
A Diabetes Care Survey (Appendix A) was mailed to all patients with a diagnosis of diabetes who were being seen by a primary care physician in the Rancho Cordova Clinic in the planned visit or within the previous calendar year. This survey was based on the Patient Assessment of Chronic Illness Care (PACIC), developed and validated by the MacColl Institute for Healthcare Innovation. 5 There were three primary sections to the survey. In Section 1 there were six questions related to the frequency of self-care behaviors. Each question was prefaced by the phrase “How many of the last 7 days did you.” Numeric responses ranged from 0–7. In Section 2 there were eight questions related to patient's understanding of self-care activities. Each question was prefaced by the phrase “How well do you understand each of the following?” Responses ranged from 1 = “I don't understand at all” to 4 = “I understand completely.” In Section 3 there were six questions related to patient's perception of care coordination and teamwork. Each question was prefaced by the phrase “In the last six months when you received care for your diabetes, were you?” Responses ranged from 1 = “Never” to 5 = “Always.” We compared the survey responses of patients who had attended a planned visit compared to those patients who had not.
Statistical analysis
Statistical analysis was performed using the STATA software, version 8.2 (StataCorp, College Station, Texas). Pre and post planned visit means of A1C, LDL-C, blood pressure, the change from baseline for these measures, the differences between the treatment and comparison groups, and survey results were assessed using t-tests, with significance set at 0.05.
Results
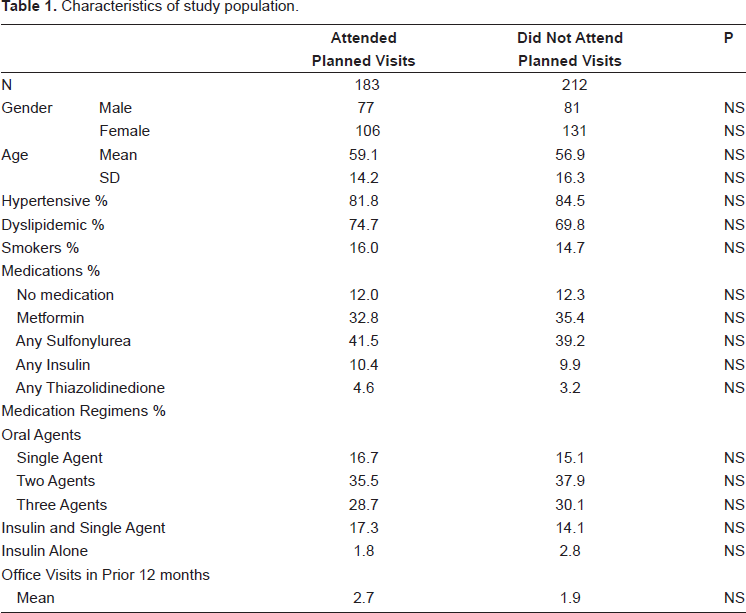
Baseline demographics of the 183 patients with DM who attended one planned visits are presented in Table 1. The mean age was 59 years. Nearly 58% were women. More than two-thirds of the group had hypertension and hyperlipidemia in addition to their DM. There were 212 patients in the comparision group; those who did not accept the invitation for a planned visit. There were no significant differences between these two groups for age or gender or other characteristics such as percentage with hypertension, dyslipidemia, or smoking. There were also no significant differences between these two groups for medication regimens or number of office visits in the prior 12 month period.
Characteristics of study population.
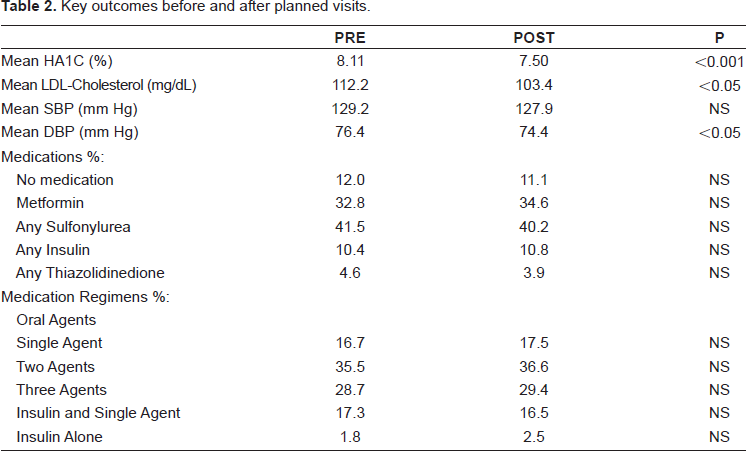
Changes in key outcomes before and after the planned visits are presented in Table 2. There were significant improvements in A1C, diastolic blood pressure, and lipid control. There was no significant change in systolic blood pressure. There was no significant change in medication regimen after the planned visit. The results for the comparison group are presented in Table 3. There were no significant changes in A1C, blood pressure, lipid control, or medication regimen during the observation period. The changes from baseline in these outcome measures between the planned visit and comparision groups are presented in Table 4. There were significant improvements in A1C, lipid control, and diastolic blood pressure. There was no significant change in systolic blood pressure. The results from the Diabetes Self-Care Survey are presented in Table 5. Of the approximately 850 surveys mailed out, 206 completed surveys were returned. There were 85 respondents who had been to a planned visit and 121 respondents who had not been to a planned visit. Patients who attended planned visits self-reported an increased frequency of self-care behaviors, an increased understanding of self-care activities, and an increased acknowledgment of care coordination and teamwork.
Key outcomes before and after planned visits.
Key outcomes for comparison group.

Outcome differences between planned visit and comparison groups; change from baseline.
Diabetes survey results.

Discussion
The main finding of our study is that patients with type 2 DM who received care at a planned visit experienced improved outcomes in measures of glycemic, blood pressure, and lipid control. Patients also reported more efforts toward self-care behaviors, understanding of self-care, and acknowledgement of care coordination and teamwork in the practice. The methodology of this student as a before and after assessment does not carry the strength of a randomized trial; therefore, biases among the patient population may have influenced outcomes. For example, there may have been a selection bias in that those who participated in planned visits were more activated towards changes that influenced their glycemic, lipid or blood pressure control. Also, those who completed the survey's may reflect the same selection bias.
There are other plausible explanations for this study's findings. It is possible that planned visits served to re-engaged patients in the care of their diabetes. This is a reasonable conclusion if there was little evidence for any care in the previous year. However, both the study and comparison groups had a similar number of documented encounters for primary care in the previous year. It is also possible that planned visits led to medication intensification thereby improving these outcome measures. There was no detectable increase in the number of oral agents or in the use of insulin during this study period.
The findings of this study are similar to others involving the use of planned visits. Sadur and associates performed a randomized controlled trial of 97 patients with poor glycemic control; A1C > 8.5%. 6 Their intervention included a large, multidisciplinary team (dietitian, psychologist, pharmacist, and nurse educator in a 2-hour cluster visit. Between monthly meetings a diabetes educator reviewed diabetes management with each patient by telephone twice monthly. The pharmacist reviewed computer-based medication profiles, contacted patients to verify the medications and alerted patients to any potential drug interactions. A1C levels declined by 1.3% from baseline at 6 months and self-reported changes in self-care practices improved from baseline.
In a study involving the Harvard Vanguard Medical Associates Kimura and associates described a delivery system redesign of their primary care practice including: population management, systems-based practice, and planned chronic illness care. 7 Over a 2-year period in a multispecialty ambulatory physician group practice they found improvement in overall DM composite quality measures for screening and improvement in intermediate outcomes A1C < 7, LDL-C < 100, and systolic blood pressure < 130.
Finally, Kirsh and associates did a quasiexperimental trial involving a shared medical visit within a primary care practice. 8 They found that A1C, LDL-C, and SBP all decreased; A1C decreased 1.4% (95% CI 0.8, 2.1), LDL-C decreased 14.8 (95% CI 2.3, 27.4), and SBP decreased 16.0 (95% CI 9.7, 22.3).
While the interventions in these three studies were somewhat different, they were all more effort intensive than our program. Further, the outcomes of these studies compared to ours are similar. The implication from our study is that the level of effort to achieve improved outcomes in patients with DM may not require the use of a large multidisciplinary team. Focused planned visits using the addition of a diabetic educator may achieve similar outcomes. A randomized trial comparing elements of these programs will be important to perform to better understand the level of intervention needed to obtain maximum benefit, balancing costs, and staffing requirements.
Disclosure
The author reports no conflicts of interest.
Footnotes
Acknowledgments
I wish to acknowledge the assistance of the UC Davis Health System Chronic Disease Management Program and the Rancho Cordova Practice Group for their efforts to establish a planned visit program. I would like to thank Larry Taylor for his help in obtaining the registry and outcome data for this study and to Ronald Fong, MD, MPH for his assistance with the statistical analysis.