
Abstract
Before the introduction of routine measurements of serum calcium in ambulatory services, PHTP (primary hyperparathyroidism) was symptomatic with classic bone disease (known as osteitis fibrosa cystica) nephrolithiasis, and acute neuropsychiatric syndrome with severe hypercalcemia. Currently, PHPT presents few unspecific symptoms. This cross-sectional study was conducted from December 1, 2007, through August 31, 2008 to estimate the prevalence of primary hyperparathyroidism and to describe the clinical and laboratory characteristics of patients receiving ambulatory care. From 4207 patients, we found a prevalence of PHTP of 0.78 (95% confidence interval [CI], 0.52–1.04) of which 81.8% were asymptomatic and 18.2% symptomatic. The female:male ratio was 7.2:1, and 89.7% of the women were postmenopausal. Mean age was 61.12 ± 15.73 years, mean serum calcium was 10.63 ± 1.33 mg/dL, and mean serum parathyroid hormone (PTH) was 182.48 ± 326.51 pg/mL. We found a high prevalence of PHTP at reference centers and a high prevalence of hypertension and type 2 diabetes.
Introduction
Primary hyperparathyroidism (PHPT) is characterized by high levels of serum calcium associated with high or inappropriately normal levels of parathyroid hormone (PTH). 1 PHPT continues to be the main cause of hypercalcemia encountered during ambulatory care, as previously indicated by a number of population-based studies.2,3 Diagnosis is generally simple, although there are many causes of hypercalcemia such cancer, vitamin D intoxication, and use of lithium and thiazide diuretic. 1
PHPT used to be clinically defined as a symptomatic disease, which presented clinical signs of severe bone disease (osteitis fibrosa cystica), renal lithiasis, and acute neuropsychiatric syndrome, which is associated with severe hypercalcemia. 4
After the introduction of routine serum calcium measurement in ambulatory care in the 1970s, the clinical presentation of PHPT changed, and a period of asymptomatic PHPT began with a 4- to 5-fold increase in incidence. 4 Due to a greater understanding of PHPT and the improved techniques for measuring serum calcium, PHPT became asymptomatic, characterized by mild hypercalcemia.4–6 Throughout Europe and the United States, PHPT is considered the third most common endocrine disease after type 2 diabetes and thyroid diseases.5,6 The incidence of PHPT increases with age and is more prevalent in women, especially postmenopausal women.2,7,8 Muscle weakness and fatigue are among the most common complaints presented by patients with asymptomatic PHPT and are often accompanied by degrees of constitutional, behavioral, and psychiatric symptomatologies.9,10 In asymptomatic PHPT, the demonstration of bone involvement depends on the bone densitometry evaluation, which demonstrates the predominant decrease of mineral bone density in the cortical bones, especially in the distal radius. 10
A new PHPT phenotype has been investigated by researchers in patients with normal serum calcium and high levels of PTH, characterized as normocalcemic hyperparathyroidism, which may be an early form of the disease.8,11
Nonclassical manifestations of PHPT, such as type 2 diabetes mellitus (T2DM), pancreatitis, peptic ulcers, depression, multiple endocrine neoplasia type 1 (MEN-1) and cardiovascular diseases such as hypertension, cardiac arrhythmias, acute myocardial infarction (AMI) and congestive heart failure (CHF) have been associated with these patients, 9 but data are still conflicting.
The prevalence of PHPT is variable worldwide, but it has been well documented in Europe and the United States in population-based studies,5,12 thus rendering it necessary to identify the prevalence in other parts of the world.
The aim of the present study was to evaluate the prevalence of PHPT in patients attending reference centers, as well as to determine the presence of nonclassical manifestations.
Methods
A cross-sectional study was conducted to determine the prevalence of primary hyperparathyroidism during the period from December 2007 to August 2008, in 2 endocrine reference centers in the city of Recife, Brazil: the Agamenon Magalhães Hospital (a university hospital) and the Unit for Endocrinology and Diabetes at a private institution. The study was approved by the Committee of Ethics and Research at the Agamenon Magalhães Hospital.
Study subjects
Patients previously diagnosed with PHPT, who were returning to these clinics for their routine consultations, were referred to the interviewer in order to answer the questionnaire regarding the presence of signs and symptoms, both specific (nephrolithiasis, osteitis fibrosa cystica, neuropsychiatric syndrome) and unspecific (muscle weakness, fatigue) of PHPT. Other diseases associated with PHPT (MEN-1, hypertension, T2DM, pancreatitis, peptic ulcers, angina, AMI, cardiac arrhythmias and depression) were also evaluated through the patients' medical histories.
Patients who were returning for their routine checkup and presented serum calcium levels that were equal to or higher than 10.3 mg/dL were required to carry out a further evaluation of their serum calcium levels. Those with confirmed hypercalcemia but who did not present exclusion criteria such as renal failure, malignant neoplasia, the use of medications (lithium and tiazidic diuretics), and a family history of benign hypercalcemia were invited to participate in the study and referred for evaluation of intact PTH levels.
Patients diagnosed with high or in appropriately normal PTH levels were also evaluated with the same questionnaire as the patients previously diagnosed with PHPT. Patients were classified as symptomatic PHPT if they presented evidence of nephrolithiasis, severe bone disease (osteitis fibrosa cystica), typical neuropsychiatric syndrome reflected by mental confusion, depression, increase in profound responses and reflexes, and as asymptomatic PHPT, when the patient did not present the above mentioned findings. 13
Methods
Serum calcium was measured using an auto-analyzer (Cobas Mira Plus, Hoffmann-La Roche Ltd, Basel, Switzerland) with reference levels of 8.5 to 10.3 mg/dL and was conducted on patients after 12-hour fasting without the use of a tourniquet. In the presence of hipoalbuminemia, serum calcium was corrected with the following formula: total calcium (mg/dL) –0.8 × (albumin (mg/dL) –4). 14
Serum PTH was measured by automated electrochemiluminescence (Elecsys, Roche Diagnostics GmbH, Mannhein, Germany) with reference levels of 15 to 65 pg/mL with a detection limit of 1.2 pg/mL. In appropriately normal levels of PTH were considered as those higher than the 75th percentile of the reference level, PTHi ≥ 52.5 pg/mL, in the presence of hypercalcemia on 2 occasions.
Statistic analysis
Statistical calculations were obtained with the Statistical Package for the Social Sciences (SPSS) software version 13 for Windows (SPSS Inc, Chicago, IL). Descriptive statistics included absolute and percentage distributions and the following statistical measurements: mean, median, standard deviation, minimum value, and maximum value. Statistical inference techniques involved the application of the Pearson chi-square test or the Fisher exact test when conditions for using the chi-square test were not verified and the Student t test with equal variances. The margin of error used for statistical test decisions was 5.0%. The period prevalence was calculated as the number of existing cases for 9 months divided by the population and expressed as a percentage of every 1000 population; 95% confidence intervals (CIs) were estimated assuming a binomial distribution.
Results
Of the 4207 patients evaluated, PHPT was found in 33 patients. The age of the patients ranged from 25 to 88 years, with a mean age of 61.12 ± 15.73 years. The period prevalence of diagnosed PHPT was 7.8 per 1000 patients (95% CI, 5.2–10.4).
In the university hospital, 3479 patients were evaluated, of which 8 had previously been diagnosed with PHPT, and 50 presented hypercalcemia (1.44%) and were therefore submitted for a further measurement of serum calcium. Of these 50 patients, 21 (42%) presented with persistent hypercalcemia and were submitted for measurement of serum PTH with an additional 13 new cases, which corresponds to a prevalence of 0.60%. Of these 21, 19 (90.5%) were female, and 2 (9.5%) were male (Table 1).
General characteristics of patients with PHPT.
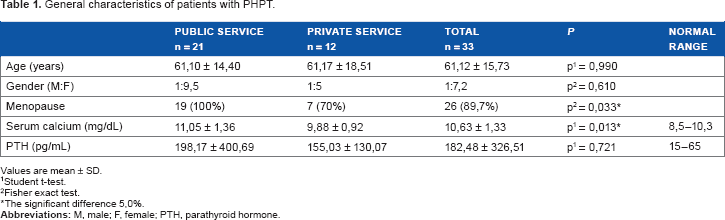
Values are mean ± SD.
Student t-test.
Fisher exact test.
The significant difference 5,0%.
In the private service, 728 patients were evaluated of which 6 had previously been diagnosed with PHPT; with the addition of 6 new cases, this corresponds to a prevalence of 1.64%. Of these 12 patients, 2 (16.7%) were male, and 10 (83.3%) were female (Table 1). In the total group, (4/33) 12.1% of the patients were male, and (29/33) 87.9% were female. All women who attended the public service were post menopausal, as were (7/10) 70% (P = 0.03) those who attended the private service (Table 1). From the total of 33 PHPT cases, 27 (81.8%) were asymptomatic (Fig. 1).

Percentage of patients with primary hyperparathyroidism according to the clinical presentation.
Among the 33 patients, the mean serum calcium was 10.63 ± 1.33 mg/dL. In the public service, mean serum calcium was 11.05 ± 1.36 mg/dL, and it was 9.88 ± 0.92 mg/dL in the private center (P = 0.01). Mean serum PTH was 198.17 ± 400.69 pg/ml in the public service and 155.03 ± 130.07 pg/mL in the private (Table 1).
With regard to the specific symptoms, 6.1% (2/33) of patients had osteitis fibrosa cystica, 18.2% (6/33) had nephrolithiasis, and 3% (1/33) had acute neuropsychiatric syndrome. In the state-run service (2/21) 9.5% presented osteitis fibrosa cystica. Nephrolithiasis was found in (5/21) 23.8% of patients in the public service and in (1/12) 8.3% of patients in the private service. With regard to neuropsychiatric syndrome, (1/21) 4.8% was recorded in the public service, and none in the private service (Table 2).
Classical and non-classical manifestations of PHPT.
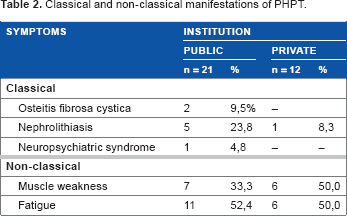
With regard to nonclassical manifestations, muscle weakness was present in (7/21) 33.3% of patients in the public service and in (6/12) 50% in the private. Fatigue was recorded in (11/21) 52.4% of patients in the public service and in (6/12) 50% in the private (Table 2).
MEN-1 was presented in 2 patients in the private clinic. Hypertension and T2DM were present in 71.4% and 33.3%, respectively, in the public service and 50% and 33.3%, respectively, in the private service. Cardiac arrhythmia, CHF, and AMI were not encountered. Total results showed 6.1% of patients with MEN-1, 63.6% with hypertension, 33% with T2DM, 6.1% with peptic ulcer, and 18.2% with depression.
The clinical and laboratory differences between asymptomatic and symptomatic patients are shown in Table 3.
Clinical and laboratory differences between asymptomatic and symptomatic PHPT.

The significant difference 5,0%.
Fisher exact test.
Student t-test.
Discussion
In the present study, we found a high prevalence of primary hyperparathyroidism and its nonclassical manifestations in patients attending reference endocrine centers.
There was a predominance of women at both centers. All women at the public center were post menopausal, and this may be due to the fact that in the private service, PHPT was diagnosed at an earlier age through the presentation of normocalcemia.
The mean serum calcium and PTH levels at the public center were significantly higher than those at the private center. When including patients from both centers, a total of 81% were classified with asymptomatic PHPT and 18.2% with symptomatic PHPT. These findings are in agreement with most of the studies reported.15,16 Asymptomatic patients presented lower serum calcium and PTH measurements than symptomatic patients, but this was not statistically significant.
In Europe, population-based epidemiological studies have indicated a prevalence of PHPT of 21/1000 in women between 55 and 75 years of age, which is an estimated equivalent of 3/1000 of the general population. 5 In the city of Tayside, Scotland, a population-based study showed a prevalence of PHPT of 6.72 per 1000 population in 2006 that was greater in females than males and increased with age. 17 These authors used less rigid criteria than ours, that is, high serum calcium on 2 occasions in the presence of serum PTH above 20 pg/mL. This study found 7.8 cases per 1000 patients, although this was not a population-based study.
In the US city of Rochester, New York, a population study concerning the incidence of PHPT at the beginning of the 1970s, indicated an increased incidence of PHPT between 1974 and 1982, followed by a decline during the subsequent years. It is believed that the introduction of the routine measurement of serum calcium was responsible for the incidence peak during the 1970s. 6
In a case series that evaluated the clinical and laboratory changes over a period of 17 years, a female predominance was found with a mean age of 54.4 years. 18 The study showed an increase in the number of diagnosed cases over the last few years with a predominance of symptomatic patients, with 88.8% in the first 4 years and 52.3% in the later years, thus indicating an increase in asymptomatic diagnoses. 18
Another presentation of PHPT has emerged, known as normocalcemic PHPT. Patients with this condition have no symptoms and demonstrate high levels of PTH with normal serum calcium, which are considered early signs of the disease. 11 This would explain our findings of a higher prevalence of PHPT in the private center, since these patients undergo routine checks for PTH levels for osteoporosis workup.
In a longitudinal cohort from New York, patients with normocalcemic PHPT referred from a bone disease service were monitored for a period of 8 years. It was observed that these patients had a greater skeletal involvement, and complications had developed in 50% of them. It is believed that this form of PHPT may represent an early stage of the symptomatic disease. 19
In another Swedish study, conducted with premenopausal women of between 40 and 50 years of age, the prevalence of PHPT varied from 0.7% to 9.3%, depending on the biochemical criteria used to identify the balance between calcium and PTH. Where hypercalcemia was considered to be from 10 mg/dL and in appropriately normal PTH considered to be above 49 pg/mL, the total prevalence or PHPT was 2.7%. 20 These data may lead to the conclusion that the lowest cutoff point of serum calcium and PTH may be necessary in order to make an early diagnosis of PHPT, as reinforced by previous studies.
In the present study, only 18.2% of patients were classified as symptomatic, and these had higher serum calcium and PTH levels together with the characteristic clinical presentation.
Patients with PHPT may have nonspecific symptoms, such as weakness, easy fatigue, and depression, among others. According to the Third International Workshop in Asymptomatic Primary Hyperparathyroidism, 21 these symptoms do not constitute criteria for surgical treatment, since most of the data are from observational studies22–27 and have divergent conclusions. In the present study, 39% of patients had muscle weakness, more than half complained of fatigue, and 18% had been previously diagnosed with depression. Muscle weakness was significantly present in the vast majority of symptomatic patients. This finding may be due to the high levels of serum calcium and the long exposure to persistently high levels of PTH.
During recent years, many authors have questioned the association of nonclassical organ involvement with PHPT. PHPT may be related to hypertension, disturbances in the rennin-angiotensin system, cardiac arrhythmia, and functional and structural alterations on the vascular wall. 28 The pathogenesis of hypertension remains controversial because in some studies, after surgical cure, there was no improvement in blood pressure.29,30 A mathematical model demonstrated that PHPT was the strongest predictor of arterial stiffness, apart from age, sex, smoking, hypertension, or T2DM. 30 Hypertension was observed in more than 50% of our patients, but none of them had a history of any other cardiovascular diseases.
It is believed that an increase in PTH is associated with a reduction in insulin sensitivity. Thus, a high frequency of glucose intolerance and T2DM may be expected.31–33 In a cohort of 105 patients with PHPT, the prevalence of glucose intolerance and undiagnosed T2DM was greater than in the control group. 34 These data were not confirmed in a study with 61 patients with asymptomatic PHPT in which the prevalence of preexistent T2DM, glucose intolerance, and undiagnosed T2DM was greater in the control group. 35 In the present study, we found a higher prevalence of T2DM in PHPT patients than would be expected for the general population at the same age.
Conclusion
It was observed in the present study that patients from the public service presented higher serum calcium and PTH levels than in the private service, which would suggest a late medical assessment, thus delaying the diagnosis. The results of this study showed a high prevalence of primary hyperparathyroidism, reinforcing the importance of measuring serum calcium in patients undergoing ambulatory care. A high prevalence of hypertension and T2DM was found, which is known to be responsible for an increase in mortality in the general population.
Author Contributions
Conceived and designed the experiments: CE, FB. Analysed the data: CE, FB. Wrote the first draft of the manuscript: CE. Contributed to the writing of the manuscript: CE, AV, FB. Agree with manuscript results and conclusions: CE, AV, FB. Jointly developed the structure and arguments for the paper: CE, AV, FB. Made critical revisions and approved final version: CE, AV, FB. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.
Footnotes
Acknowledgements
The authors wish to acknowledge the patients and employees of the surveyed institutions that contributed to the research.