
Abstract
Osteoporosis and atherosclerosis share common risk factors and the association of low bone mass with increased cardiovascular morbidity and mortality has been demonstrated in some studies. Nevertheless, most studies have been focused on women and only a few on individuals with type 2 diabetes mellitus (T2DM). The measurement of carotid intimal-medial thickness (CIMT) is able to detect early atherosclerotic changes and is a predictive marker of cardiovascular events. The aim of this study was to assess the CIMT and its relationship with bone mineral density (BMD) (in the femoral neck (FN) and lumbar spine (LS)) in men with T2DM. We conducted a cross-sectional study with 24 men with T2DM (aged 61
Introduction
The ageing population has a higher prevalence of diabetes mellitus, osteoporosis, and atherosclerosis, three of the major public health problems worldwide. The association between low bone mineral density (BMD) and increased cardiovascular morbidity and mortality has been suggested in some studies,1–6 conducted mainly in postmenopausal women.7–10 Few of them included men as well as patients who have type 2 diabetes mellitus (T2DM). 11
The association between cardiovascular disease and calcium deposition was first described in the nineteenth century, 12 but only in the late twentieth century were some elements linking atherosclerosis and low BMD discussed. 13 These diseases share some common risk factors such as advanced age, estrogen deficiency, inflammation, and hyperhomocysteinemia.3–5 Additionally, some studies have suggested a close association between them.2,7,9
Measurement of the intimal-medial thickness in the carotid arteries with B-mode ultrasound is a non-invasive, sensitive, and reproducible technique for identifying and quantifying subclinical vascular disease and the risk of a wide range of cardiovascular diseases.14–20 It is, therefore, important to determine whether this occurs in the context of low BMD in men with longstanding T2DM, a population known to have a high risk of atherosclerotic vascular disease and a possible decrease in bone strength. 21
The analysis of the association between low bone mass and atherosclerosis in male diabetic population is important because of the lack of studies on this subject. The study of this relationship helps to establish the need for further investigation on the presence of atherosclerotic involvement in elderly diabetic men with low bone mass and vice versa.
The aim of this study was to assess the carotid intimal-medial thickness (CIMT) and its relationship with BMD in men with T2DM.
Subjects and Methods
Study Population
The patients were 24 men, aged from 60 to 80 years, with the diagnosis of T2DM according to the American Diabetes Association criteria. 22 The study was approved by the Ethics in Research Committee of Agamenon Magalhães Hospital. The exclusion criteria were as follows: patients with type 1 diabetes, defined as patients diagnosed before the age of 20 or who have been hospitalized for diabetic ketoacidosis; and/or chronic use (past or present) of glucocorticoids. Laboratory or radiological evidence of one of the following: hyperthyroidism and hypothyroidism (patients with normal TSH levels were stabilized and included), hypoparathyroidism or hyperparathyroidism, rheumatoid arthritis, Paget's disease of bone, bone disease such as osteomalacia or osteogenesis imperfecta, advanced scoliosis or extensive lumbar fusion, malabsorption syndrome, and/or malignant neoplasm in the last five years (except basal cell carcinoma).
After informed consent was obtained, the patients answered a specific questionnaire and underwent a complete physical examination. Blood was collected after an overnight fast for biochemical measurements.
The ultrasound study of carotid arteries was performed with subjects in the supine position using the B-mode Logic-E ultrasound machine (GE Medical Systems). The CIMT was measured at three different sites on the left and right sides. We calculated the average of both sides and then the bilateral mean, using a total of six measurements per patient which were performed by a single radiologist (EG).
Serum chemistries were processed in a dry chemistry auto-analyzer (Vitros system, Johnson & Johnson), and hemoglobin A1c concentrations were determined by immunoturbidimetric assay (Cobas 501, Roche Diagnostic).
The bone densitometry was performed by dual X-ray absorptiometry of the lumbar spine (LS) at L1 to L4 and femoral neck (FN) (GE Healthcare Lunar Prodigy Advance–-Lunar Corporation, Madison, Wisconsin) and was used to measure the t-score to stratify patients according to the presence of osteoporosis (defined as a t-score less than –2.5) and osteopenia (defined as a t-score between –1 and –2.5), according to the World Health Organization criteria. 23
Statistical Analysis
Analyses were performed separately by taking into account the extent of BMD of FN or LS compared to CIMT. At each site, patients were divided into two groups, the first comprising patients who had normal BMD (t-score > –1), the second group comprising those with osteopenia or osteoporosis. Correlations were also performed between BMD sites in normal and osteopenia or osteoporosis patients. The differences between all the risk factors studied was obtained using the Student t test for quantitative variables and the chi square test in the case of qualitative variables. The correlation measurements were made using the Pearson correlation test. A confidence interval of 95% was used. The statistical analyses were performed using the SPSS Statistics (Version 17.0). The significance was considered for a P value less than 0.05.
Results
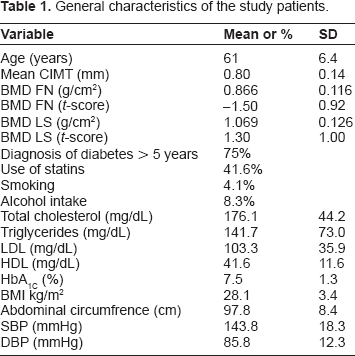
The baseline characteristics of the studied patients are presented in Table 1. No significant differences were found in age, time since the diagnosis of diabetes, smoking habits, alcohol intake, blood pressure, BMI, AC, HbA1c, and serum lipids between the groups with normal and abnormal BMD results both at LS and FN (Tables 2 and 3). The prevalence of osteopenia and osteoporosis at the FN was 45.8% and 16.6%, respectively, while the corresponding figures for the LS were 62.5% and 8.3%, respectively.
General characteristics of the study patients.
Characteristics of patients according to femoral neck BMD.

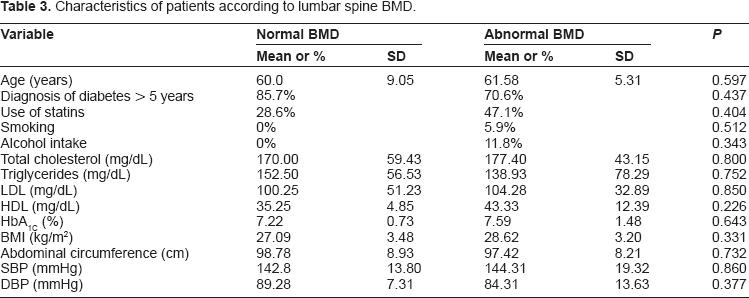
Characteristics of patients according to lumbar spine BMD.
When stratified according to the FN BMD, nine patients had BMD within the normal range with mean CIMT of 0.7 mm (SD

Carotid intimal-medial thickness according to the mean BMD of the femoral neck.
Regarding LSBMD, 7 (29%) patients had a normal result, while 17 patients (71%) were found to have osteopenia or osteoporosis. The mean CIMT was 0.81 mm (SD
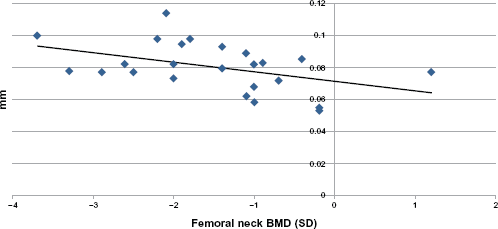
Correlation between bone mineral density in the femoral neck and carotid intimal-medial thickness.
Discussion
Our data showed a significant correlation between decreases in BMD and CIMT in men with T2DM, which was unrelated to traditional risk factors such as blood glucose control, blood pressure, or serum lipids concentrations. Atherosclerosis and osteoporosis may share common risk factors such as advanced age, estrogen deficiency, inflammation, hyperhomocysteinemia and activation of RANKL/OPG system. One study 24 suggested that some polymorphisms in vitamin D receptor gene could be a common point between the BMD variation and CIMT. Another study has found an association with the RANK (receptor activator of nuclear factor kappa B)/RANK-Ligand/OPG (Osteoprotegerin) and vascular pathology due its activation in the case of high bone remodeling states.25,26
One study suggested a unified theory involving the cholesterol metabolites (isoprenoids) as the cause of atherosclerosis, peripheral vascular disease, coronary disease, and age-related diseases such as osteoporosis and T2DM. 27
The measurement of BMD at the FN may be more accurate in old people when compared to that of the spine, because of a lack of accuracy in systematic measurements, due to spine elements irregularities, which may lead to false-positive findings. Because of this, the World Health Organization, when developing the absolute risk score for osteoporotic fractures, did not recommended the LS measurement. 28 In the diabetic population, especially those with longstanding disease, it is expected to find a higher frequency of arterial calcification which, occurring in the aorta, could directly interfere with bone density acquisition at LS, also causing false-positive results. Likewise, we found considerable less bone loss at LS in comparison with FN in our diabetic male patients.
One of the proposed mechanisms to explain the increased risk of osteoporotic fracture in the diabetic population is the accumulation of advanced glycation end-products which is thought to influence collagen synthesis and structure.21,29 In fact, although with a relative higher BMD, type 2 diabetic patients tend to have an increased risk of fracture, which may be related to pentosidine levels.21,30 Advanced glycation end-products are also considered, particularly in the diabetic population, a known step for modifications of LDL particle and in a more direct way for changes in the arterial wall, thus contributing to the atherosclerosis process. 31
Finally, we have recently demonstrated that men with longstanding T2DM also have significant iliac artery calcification as FN BMD decreases, which is not related to traditional risk factors for cardiovascular disease nor the presence of advanced renal insufficiency. 32
The findings of this study are consistent with those of other studies previously conducted in postmenopausal women and suggest that both diseases are clearly present in the elderly diabetic population.
In conclusion, we found a significant association between an increased thickness of carotid intimal-medial complex and low bone density in patients with T2DM, irrespective of other cardiovascular risk factors. This indicates that these individuals, in addition to their risk of cardiovascular disease, have a concomitant increased risk of developing osteoporosis.
Author Contributions
Conceived and designed the experiments: MAPC, FB. Analyzed the data: MAPC, EB. Wrote the first draft of the manuscript: MAPC, JMCMA, ETAMG, GV. Contributed to the writing of the manuscript: MAPC, EB, JMCMA, ETAMG, GV, FB. Agree with manuscript results and conclusions: MAPC, EB, JMCMA, ETAMG, GV, FB. Jointly developed the structure and arguments for the paper: MAPC, EB, JMCMA, ETAMG, GV, FB. Made critical revisions and approved final version: MAPC, EB, JMCMA, ETAMG, GV, FB. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.