
Abstract
An infant with hypoplastic left heart syndrome showed paroxysmal episodes of bradycardia, hypotension, and hypoxemia upon crying after modified Norwood operation. Echocardiography showed decreased right ventricular ejection with grade III tricuspid regurgitation, a markedly enlarged aortic arch, and accelerated blood flow distal to the enlarged aorta. Aortography demonstrated an aneurysmal neo-aorta with an apple-shaped appearance. The pressure measurements revealed intriguing aortic hemodynamics: the diastolic pressure of the ascending aorta was lower than that of the descending aorta (42 mmHg vs. 52 mmHg) despite no systolic pressure gradient. Markedly reduced compliance in the ascending aorta relative to that in the descending aorta, which was suggested by the difference in time constant of aortic pressure decay, may explain this hemodynamics. Impaired coronary circulation caused by lowered diastolic pressure in ascending aorta was indicated by reduced subendocardial viability ratio, and may account for her symptom and lowered ventricular ejection. The patient's condition was indeed significantly improved by surgical correction of the aortic shape. This case highlights the importance of aortic shape and properties after Norwood operation.
Aortic arch obstruction is a relatively common complication after the Norwood procedure and can be deleterious by causing an increased afterload on the single ventricle, resulting in ventricular dysfunction, 1 tricuspid regurgitation, and an imbalance in the systemic-to-pulmonary blood flow ratio. 2 Although a systolic pressure gradient produced by the stenotic reconstructed aorta best characterizes this complication, our case presented in this report showed that a paradoxical diastolic pressure gradient without an evident systolic pressure gradient was associated with hemodynamic deterioration after Norwood operation, possibly due to impaired coronary perfusion.
Case Report
A full-term newborn girl with a birth weight of 2926 g had hypoplastic left heart syndrome characterized by mitral atresia, aortic atresia, and hypoplasia of the ascending aorta and the aortic arch. A modified Norwood operation 3 was performed on day 22 after birth, following bilateral pulmonary artery banding and continuous infusion of prostaglandin E1 to keep the ductus arteriosus open. The main pulmonary artery was transected and anastomosed to the ascending aorta and the aortic arch, which was enlarged using an autologous pericardial patch. A ringed graft (diameter, 4 mm) was placed from the right ventricle to the pulmonary artery as a source of pulmonary blood flow.
During the postoperative recovery period, the patient showed paroxysmal episodes of bradycardia, hypotension, and hypoxemia upon crying. Echocardiography revealed decreased right ventricular ejection with grade III tricuspid regurgitation, a markedly enlarged aortic arch, and accelerated blood flow distal to the enlarged aorta. The aortic arch enlargement was confirmed using aortography; the aortography showed an aneurysmal neo-aorta with an apple-shaped appearance (Fig. 1). The site of the aortic arch aneurysm corresponded with that of the pericardial patch plasty.

(
The pressure measurements obtained using a high-fidelity micromanometer 4 before performing an angiography showed intriguing aortic hemodynamics (Fig. 2). Although there was no systolic pressure gradient across the aneurysmal neo-aorta, the diastolic pressure of the ascending aorta (proximal end of the aneurysmal neo-aorta) was lower than that of the descending aorta (distal end of the aneurysmal neo-aorta) (42 mmHg vs. 52 mmHg). The time constant of the diastolic pressure decay 5 (0.30 s vs. 0.67 s) was more than 2-fold smaller in the ascending aorta than in the descending aorta, indicating much lower compliance in ascending aorta.
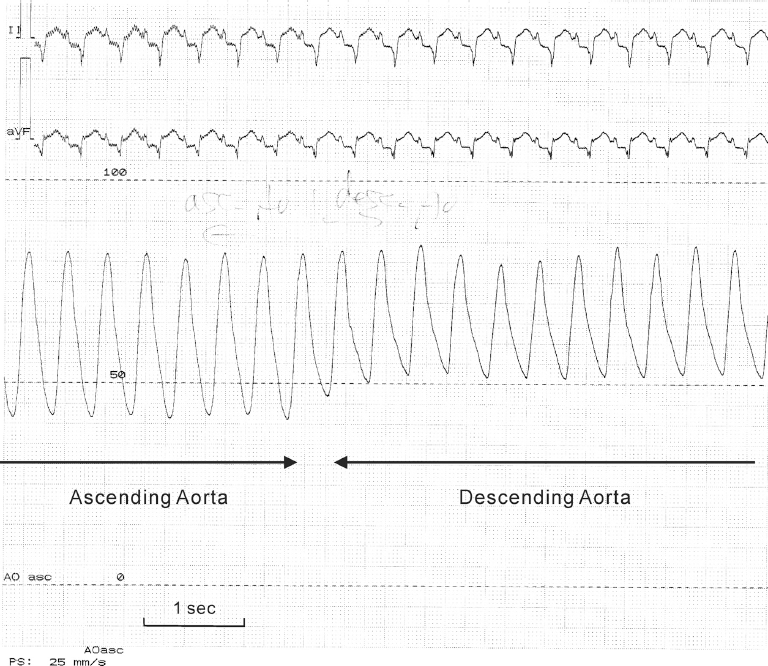
Analog recording of pressure measurement was performed using a high-fidelity micromanometer mounted on a 0.014-inch guidewire; the guidewire was advanced from the ascending aorta to the descending aorta.
Because balloon dilation failed to relieve the discrepancy in the size of the ascending and descending aorta, surgical repair was subsequently performed; the repair dramatically improved her symptoms as well as right ventricular ejection (fractional area change, from 12% to 20%) and reduced tricuspid regurgitation (from Grade III to Grade I–II).
Discussion
In an infant after modified Norwood operation, we observed aneurysmal formation of the reconstructed aorta. The aneurysmal site could presumably have been dilated because of the distending pressure attributed to the resistance to forward flow at the anastomosis site (distal end of the aneurysmal neo-aorta). Previous reports also depicted the occurrence of the enlargement of neo-aorta with homograft 6 as well as autologous patch plasties. 7 Influence of the type of materials used on the occurrence of aortic arch enlargement remains unclear and needs to be clarified in the future study. Interestingly, unlike many other patients who had stenotic neo-aorta, the patient showed a paradoxical diastolic pressure gradient without systolic pressure gradient: the diastolic pressure of the ascending aorta was lower than that of the descending aorta (Fig. 2). The great difference in the time constant values of diastolic pressure decay between ascending and descending aorta implied that the compliance of the ascending aorta was much lower than that of the descending aorta, 5 and the distal end of the aneurysmal neo-aorta served as a valve during diastole. Aortopulmonary collateral shunts in this patient were only minimum on aortography, which was supported by echocardiographic demonstration of no aortic flow reversal during diastole, and thus could not account for the diastolic pressure gradient.
The unique aortic hemodynamics may have resulted in an inadequate coronary blood supply because of the paradoxically lowered diastolic pressure of the ascending aorta and may be responsible for the symptoms of heart failure in our patient. This hypothesis is supported by the fact that the subendocardial viability ratio of 0.7, 8 which is calculated as the time-tension index divided by the diastolic pressure time index (an index of myocardial oxygen supply/demand balance), was less than 70% of the mean value (1.1 ± 0.2) obtained from 31 control subjects with a small ventricular septal defect (unpublished data).
A systolic pressure gradient across the anastomosis site is a hallmark of the existence of a stenosis. However, our case indicated that discrepancy in the size of the ascending and descending aorta and low compliance of the surgically created neo-aorta could cause significant hemodynamic deterioration even without an evident systolic pressure gradient. Further, the present case emphasizes the importance of the surgical design of the neo-aorta in the Norwood operation.
Author Contributions
Analysed the data: SM. Wrote the first draft of the manuscript: SM. Agree with manuscript results and conclusions: SM, HS, HI, HS. Jointly developed the structure and arguments for the paper: HS, HI, HS. Made critical revisions and approved final version: HS. All authors reviewed and approved of the final manuscript.
Funding
Supported by Medical Research Grants from Kawano Memorial Foundation (H.S.), and Saitama Medical University Internal Grant (H.S.).
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.
Footnotes
Acknowledgments
We thank our departmental colleagues who performed the catheterization studies.