
Abstract
Background
Coronary sinus rupture (CSR) is a rare preventable complication of cannula insertion for retrograde cardioplegia. In the hands of an inexperienced surgeon, this complication has the risk of potential mortality and morbidity, and its repair is technically challenging. Techniques for repairing CSR have been reported previously. In this study, we determined predictors of CSR following coronary artery bypass graft (CABG) surgery.
Methods
Over a four-year period, we retrospectively analyzed 1500 patients in whom a retrograde coronary sinus catheter was used to administer cardioplegic solution. CSR occurred in 15 patients. (12 women and 3 men). Variables such as age, weight, body mass index, gender, aortic clamp time, pump time, cardiomegaly, ejection fraction, and number of grafts were determined for each patient. Factors correlated with CSR were analyzed using multiple regression analysis, and odd ratios of significant variables were determined.
Results
In multiple regression analysis, factors such as female gender, age, weight, and body mass index showed a significant correlation with CSR, and their odd ratios were 4.2, 1.0, 0.96, and 2.2, respectively.
Conclusion
In all 15 cases, a retrograde cannula with a self-inflatable balloon was used and 12 patients were woman with low body mass index. Forceful insertion due to coronary sinus web, fragility of arteries in thin patients, or a small coronary sinus caused CSR in the hands of an inexperienced surgeon.
Introduction
Delivery of cardioplegia via the coronary sinus was first described by Melrose in 1955. 1 Lillihei et al 2 subsequently used the same method routinely for heart protection. The advantage of this method is steady homogenous delivery and distribution of cardioplegia in the presence of proximal coronary artery stenosis or occlusion. This route of delivery also avoids the problem of stunning or an island of poorly protected myocardium, which can occur with antegrade delivery. The mechanism of myocardial protection due to retrograde cardioplegia is similar to that for the antegrade method, in that both techniques can provide nutritive flow and myocardial cooling. However, the two routes differ in their distribution. Retrograde flow via the coronary sinus distributes to subendocardial muscle tissue whether coronary artery stenosis is present or not, and distributes preferentially in the left ventricle, with decreased flow to the septum and right ventricle. Despite this decreased flow to the right side of the heart, retrograde delivery of cardioplegia provides effective cooling of the right ventricle and septum. 3
In redo CABG surgery, injection of antegrade cardioplegia causes atherosclerotic plaque emboli of grafts while the injection of retrograde cardioplegia causes washing of small atherosclerotic plaque out of the arterial system and allows the arterial graft to be deaired in a retrograde fashion. 4
In patients with aorta regurgitation, injection of cardioplegia into the aorta root does not provide adequate aortic root pressure but does not cause diastolic arrest, so retrograde injection can be used to protect the heart. An additional advantage of retrograde cardioplegia is the ability to deliver it while performing key technical components of an operation. For example, during mitral valve surgery, retrograde cardioplegia may be given without the need to reposition the retractor because myocardial protection is no longer dependent on a component aortic valve, as it would be in the case of antegrade delivery, thus allowing uninterrupted progression of surgery. 5
The disadvantage of retrograde cardioplegia includes possible injury to the coronary sinus by the catheter, stylet or balloon, myocardial injury with edema and hemorrhage if cardioplegia is delivered at a pressure higher than 50 mmHg, and the possibility of inadequate protection of the right ventricle. 5 In fact, some anterior parts of the right ventricle and parts of both atria would not drain from the coronary sinus, and the small cardiac vein would drain most of the blood from the anterior part along the marginal artery (in the atrioventricular groove) into the right atrium.
The the besius vein enters into the right atrium directly and sometimes enters into the right ventricle. In the absence of an anomalous venous system, retrograde injection of cardioplegia will not protect the right ventricle. In the case of anomalous systemic veins, distribution of cardioplegia via the retrograde route will not be uniform, so it cannot protect the heart so well. 6
Considering the above advantages and disadvantages, there is no uniform agreement about routine use of retrograde cardioplegia in patients undergoing coronary artery bypass grafting (CABG) due to the potentially lethal complication of coronary sinus rupture (CSR) and poor protection of the right ventricle. A considerable number of studies have been reported in the literature, but most are case reports about techniques for CSR repair. In this retrospective clinical study, we attempted to identify predictors of CSR following CABG. Ethical approval for this research was received from the Imamali Heart Center and Imamali Hospital.
Materials and Methods
A total of 1500 patients who underwent CABG with retrograde cardioplegia at our center over a four-year period from April 1, 2003 to April 1, 2007 were studied retrospectively. Patients who underwent CABG without cardiopulmonary bypass or had combined surgery were excluded. Patients with CSR (Group A) were compared with a control group of 1465 patients who did not have CSR (Group B). Twenty patients were excluded because of reported difficulty in retrograde cannula insertion. We designed a retrospective study to identify predictors of CSR after open heart surgery. Variables such as age, gender, body mass index, body weight, number of grafts, ejection fraction, hypertension, aortic cross clamp time, pump time, left main coronary artery disease, and location of rupture were determined.
A standardized cardiopulmonary bypass protocol was used. Cardiopulmonary bypass was established by cannulation of the right atrium and an arterial cannula was placed in the ascending aorta. Medtronic DLP pulsating cardiopulmonary bypass was performed with mild core hypothermia (35 °C) using a hollow fiber membrane oxygenator (Sorine, Italy). Intermittent antegrade cold blood cardioplegia was delivered through a 10 gauge aortic root cannula, and a Medtronic retrograde cannula was placed for myocardial protection. A coronary sinus cannula with a passively inflated (Auto inflated Edward life sciences), or manual inflated balloon (Medtronic, DLP 13-15)was placed via a mattress suture in the lateral wall of the right atrium. The cardioplegic mixture consisted of 50% St. Thomas' cardioplegic solution and 50% autologous blood. A dose of 15 mL/kg was delivered antegradely to induce diastolic arrest and 3 mL/kg was administered from a retrograde cannula.
Statistical Analysis
Statistical analyses were carried out using the SPSS statistical software package 10 (SPSS Inc., Chicago, IL). All data were expressed as means ± standard deviation. Categorical and continuous variables were compared using the χ2 test and t-test, respectively. Variables with a P value <0.05 were entered in multivariate regression analysis and odds ratios of significant variables were determined. Differences were considered significant at P < 0.05.
Results
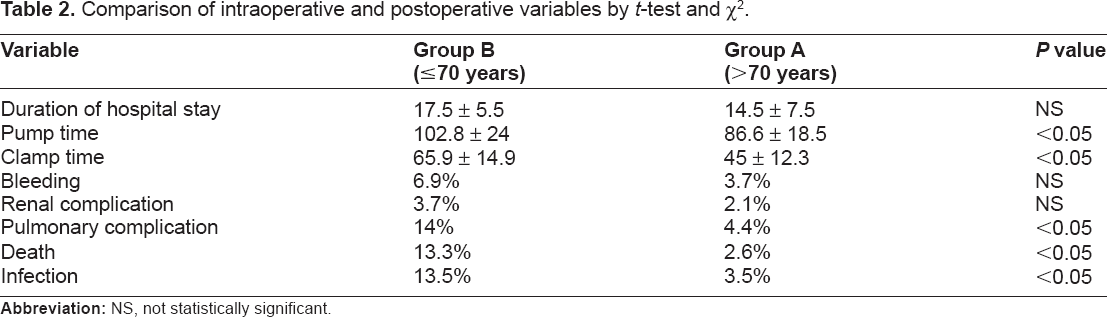
Patient characteristics are shown in Tables 1 and 2. There were significant differences between group A and Group B with respect to variables such as gender, age, body mass index, ejection fraction, postoperative myocardial infarction, congestive heart failure, preoperative creatinine >1.5, chronic obstructive pulmonary disease, infection, pulmonary complications, and death (P < 0.05). CSR was documented in 15 patients (15 of 1465, 1.02%) who received retrograde cardioplegia for heart protection, two of whom died, and CSR was repaired according to standard surgical methods in the remaining 13 patients. There was a significant difference in the incidence of postoperative complications between the two groups. Postoperative infections occurred in 13.5% of patients in Group A and in 3.5% patients in Group B (P < 0.05). The average length of stay for Group A was 17.5 ± 5.5 days and 14.5 ± 7.5 days for Group B. There were two postoperative deaths in Group A (13.3%) and 38 postoperative deaths (2.6%) in Group B. Postoperative pulmonary complications occurred in two patients (14%) in Group A and in 64 patients (4.4%) in Group B.
Comparison of preoperative variables between Group A and Group B using t-test and χ2.

Comparison of intraoperative and postoperative variables by t-test and χ2.
The mean age of the patients was 73.2 ± 2.87 years in Group A and 54 ± 8.37 years in Group B. In Group A, 12 patients were female and two patients were male. Mean body weight was 72.3 ± 11.5 kg in Group A and 67.5 ± 12.3 kg in Group B. Twenty percent of CSR occurred in the proximal portion (1.5 cm from the entrance to the coronary sinus), 70% were in the middle third, and 10% in the distal third of the coronary sinus. Two patients underwent beating onpump CSR repair. In the remaining patients, cardiopulmonary bypass was instituted immediately with systemic cooling to 30 °C, the aorta cross was clamped, and antegrade cardioplegia was given to arrest the heart. The heart was vented via the aortic root, the heart was gently retracted cephalad, and the coronary sinus area was examined carefully. If there was an intact subepicardial hematoma surrounding the coronary sinus, the decision was made to leave it undisturbed, and if the coronary sinus was torn, the decision was made to deflate the balloon, which was accomplished by leaving the balloon at the rupture site. If the rupture site was of small size, it was repaired edge to edge with 7-0 running Prolene sutures, and if the injury was large, an autologous pericardial patch repair was undertaken, as described by other surgeons. 7
Two of our 15 patients with CSR died. In the first case, we repaired the CSR after performing the distal graft and releasing the aortic cross clamp. As contraction of the heart started and the heart was lifted to the right to expose the coronary sinus, the heart became severely edematous. The long pump time caused further damage to the heart and due to the friable and fragile wall of the coronary sinus and blood in the field, extension of the CSR occurred upon movement of the heart. Because of multiple sutures and use of the pericardial patch, the coronary sinus became thrombosed and the heart was severely edematous. Due to coronary sinus obstruction, venous bleeding started from the suture line and in view of the severely edematous heart, the sternum was not closed until 48 hours later. About 30 units of whole blood, 20 units of fresh frozen plasma, 20 units of platelets, and 20 units of cryoprecipitate were given to control severe bleeding. After closing the sternum, the patient developed acute respiratory distress syndrome and respiratory failure. At last, due to unsuccessful weaning from ventilator, tracheostomy and pneumonia, the patient died.
In the other patient who died, CSR was caused by repeated attempts at cannula insertion, and rupture was secondary to traumatic stylus-guided catheterization. The rupture extended to the atrioventricular groove and, despite pericardial patch repair, the situation was deemed not salvage able and the patient died after a long pump time and in cardiac failure, and was not weaned from cardiopulmonary bypass.
Multivariate regression analysis of CSR as dependent variables.
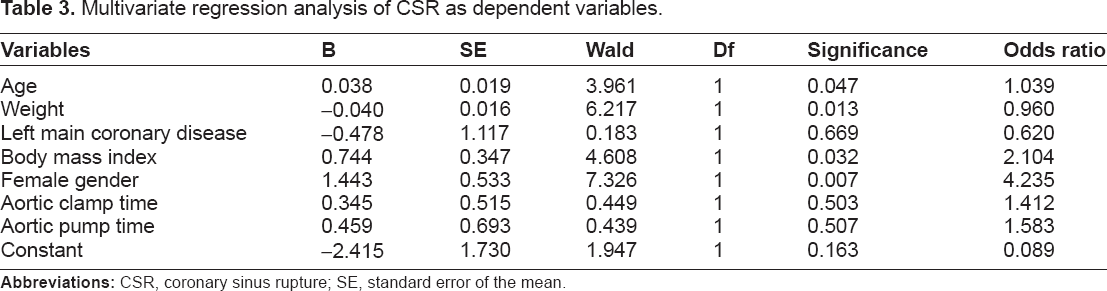
After our initial experiences of CSR repair using the beating onpump method, subsequent cases of CSR were repaired by arresting the heart with cardioplegia, fixing a cannula in the CSR site to prevent the return of venous blood and, because the surgical field was not bloody, we could repair the rupture using 7-0 Prolene with or without a pericardial patch. Fortunately, 13 of our 15 cases were repaired without any damage. In multivariate regression analysis, predictors of CSR include advancing age, female gender, weight, and body mass index, with odds ratios of 1.0, 4.2, 0.96, and 2.2, respectively. Female gender had the strongest effect on risk of CSR in CABG patients (Table 1).
Discussion
In certain situations, it is difficult to cannulate the coronary sinus for injection of cardioplegia, because it causes trauma at the entrance or along the coronary sinus, or because of inappropriate distribution of cardioplegia. Ostial valves at the entrance to the coronary sinus will prevent entry of the cannula at this site. 8 In the event of a persistent left superior vena cava, the coronary sinus will be hypoplastic, preventing entry of the cannula. In this situation, injection of cardioplegia does not protect the heart, because most of the heart veins enter the right atrium directly. 9 In cases of coronary sinus atresia, the veins of the heart drain directly into either the inominate vein, the left superior vena cava, the left atrium, or the the besius veins. 10 If the hepatic veins enter the coronary sinus via the left superior vena cava, injection of cardioplegia via the coronary sinus is not worthwhile, because the cardioplegia enters the pulmonary veins via a low pressure system and will not enter the veins of the heart, thus preventing uniform distribution of cardioplegia in the heart.6,11 If a fistula exists between the coronary sinus and the pulmonary sinus or left atrium, injection of cardioplegia does not have any protective effect, and sometimes the connection between the coronary sinus and left atrium would be in the form of an unroofed coronary sinus. 10 In the case of a left superior vena cava, and correct location of a retrograde cannula, the pressure of injection is low, and the heart would not arrest. In this situation, if the cannula is inserted forcefully, a rupture may occur in the coronary sinus. 12 If the left superior vena cava enters the coronary sinus via the left jugular vein and if there is a connection between the left superior vena cava and the inominate veins, it is possible to protect the heart via cannulation of the coronary sinus after closing the left superior vena cava. 5 If the surgeon is impatient or stressed during insertion of the retrograde cannula, the risk of CSR is increased. The risk also increases with female gender, fragile tissues, low body mass index, insertion of a large retrograde cannula into a small coronary sinus size, placement of the catheter tip in the distal third of the coronary sinus, and a high injection pressure (>50 mmHg).
Conclusion
We conclude that the best strategy to avoid the potentially lethal complication of CSR during CABG is prevention. Careful and cautious retrograde cannula insertion is essential, especially in thin female patients with fragile arteries and low body mass index. In multivariate regression analysis, female gender and low body mass index had a significant correlation with CSR. When difficulty is experienced during inserting of a retrograde cannula and repeated attempts have been made and were unsuccessful, it is best to avoid cannula insertion. If a CSR occurs, the best strategy is to inject antegrade cardioplegia, hold the retrograde cannula in the location of the rupture with an empty balloon cuff, and then sew the edges of the coronary sinus with 6-0 or 7-0 Prolene, or undertake a pericardial patch repair. However, it should be remembered that sewing of the CSR with an open aortic cross clamp when the surgical field is bloody and the heart is beating is likely to causes further damage to the coronary sinus and left circumflex coronary artery, as well as coronary sinus stenosis and thrombosis.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.
Footnotes
Acknowledgment
Special thanks are due to Dr. Roshan and the Department of Statistics for providing valuable statistical information.