
Abstract
The progression of atherosclerosis remains a major cause of morbidity and mortality. Plaque formation is an immunological response driven by a number of risk factors, and reduction of risk is the primary goal of treatment. The role of LDL-C is well established and statins have proved effective drugs, although the relative risk reduction is only around 30%. The importance of other factors—notably low HDL-C and high TGs—has become increasingly clear and the search for alternative strategies continues. Niacin is particularly effective in achieving normalization of HDL-C but is clinically underutilized due to the side effect of cutaneous flushing. The discovery that flushing is mediated by mechanisms distinct from the lipid-lowering effects has led to the development of combination drugs with reduced side effects. This review considers the evidence regarding the clinical efficacy of extended-release niacin and the DP1 antagonist laropiprant in the treatment of hypercholesterolemia and mixed dyslipidemias.
Background
Despite recent advances in our understanding of cardiovascular disease, atherosclerosis with its associated adverse clinical outcomes remains a major cause of morbidity and mortality throughout the world. Consequently, new strategies for treatment remain a major goal of health sciences research. Much of this research over the last few decades has centred on the identification of risk factors and the development of strategies that facilitate the management of that risk. The identification of the particular risk posed by elevated levels of LDL-cholesterol (LDL-C) has been the cornerstone of most recent clinical guidelines and statins have proved very effective drugs in this regard.1–4
Although the critical importance of addressing LDL-C targets is well accepted, and statins are widely recognized as the drug of choice, it is equally clear that this approach is not sufficient to prevent the majority of adverse events. Even aggressive lowering of LDL-C to below guideline targets only results in a relative risk reduction of around 25%-35%. Of equal importance is addressing other lipid abnormalities, most notably low HDL-cholesterol (HDL-C) and high triglycerides (TGs), as well as dyslipidemias associated with increased levels of small dense lipoproteins.1,4,5 These combinations are frequently found in conditions such as Type 2 diabetes, which has a strong association with all cardiovascular mortalities. 2 Strikingly, low serum HDL-C demonstrates an inverse relationship with cardiovascular risk, even in patients whose LDL-C levels are well below treatment targets. In addition, lipoprotein (a) (lp(a)) levels have also been identified as an independent risk factor and statins are ineffective in this regard,6,7 although the clinical relevance of this is not entirely clear. The risk posed by elevated lp(a) can be understood in terms of its ability to act as a vehicle for deposition of cholesterol in the intimal wall, and its structural homology with plasmin and plasminogen (combined with a notable lack of fibrinolytic activity) provides a prothrombotic environment which would support the development of vascular events. However, updated analyses suggest that the risk is modest, and the link between lp(a) and cardiovascular risk is certainly not as clear as that for LDL-C: Early data from studies with niacin suggest that lp(a) lowering may be favorable, but as yet there are no randomized clinical trials that demonstrate that selective lp(a) lowering translates into a clinical benefit. It is also true that the modest increased risk associated with lp(a) may be abrogated by aggressive LDL-lowering. 8 This notwithstanding, niacin is the single most effective clinical agent available for addressing both HDL and lp(a) levels. Treatment with niacin also significantly increases levels of ApoAl, 9 enhancing reverse cholesterol transport, thus further reducing blood lipid levels. Furthermore, niacin has additional benefits, not all of which are related to its effects on plasma lipids.10,11 Early studies indicated that these effects translate into a significant risk reduction, although more recent studies suggest a more complicated picture. It is also true that patient compliance is severely reduced due to the frequency and severity of side effects, most notably cutaneous flushing.12–15
The Effects of Niacin on Blood Lipid Levels
The effects of niacin on blood lipids are described in detail elsewhere but, briefly, they are thought to result from signalling through the adipocyte niacin receptor HM74A (GPR109A), which is a G-protein-coupled receptor linked to a Gi/Go pathway.16–19 Inhibition of cAMP (and therefore PKA) reduces activity of the enzyme hormone sensitive lipase, resulting in a decreased release of free fatty acids (FFAs) from adipocytes. The resulting reduction in plasma FFAs means a reduced substrate for hepatic TG synthesis and therefore a reduction in VLDL synthesis. Since LDL-C is generated by the action of lipoprotein lipase on VLDL, there is ultimately a reduction in plasma LDL-C. Furthermore, the reduction in VLDL also reduces cholesteryl ester transfer protein (CETP)-mediated transfer of cholesterol from HDL to VLDL and transfer of TGs from VLDL to HDL. The net result of this is a reduced catabolism of HDL. The exact contribution of these pathways to the lipid benefits is unclear because the effects on FFAs are rather short-lived—immediate release niacin preparations see a rebound to above baseline some 2-3 hours after administration.
The major benefits may stem from other actions of niacin—it is known to inhibit diacyl glyceryl acyl transferase-2 (DGAT2), one of the key enzymes involved in TG synthesis, and this inhibition leads to increased intracellular breakdown of ApoB. 20 Niacin also downregulates expression of hepatocyte ATP synthase β-chain, an HDL/ApoA1 receptor facilitating endocytosis of HDL. Reduced expression therefore leads to reduced hepatic uptake and catabolism, increasing the plasma half-life of HDL-C. 4 The mechanism of action of niacin on lp(a) is not clear, but it is known that levels can only be affected by drugs—such as niacin—that affect lipoprotein production. 7 Drugs that work by altering lipoprotein catabolism (as the statins do) are ineffective. Typically, treatment with niacin results in 30% reduction in plasma lp(a) concentrations.
Clinical Benefits of Niacin Therapy
A number of studies have demonstrated the benefits of niacin therapy with regard to favorable modulation of lipid levels and the clinical benefits associated with this. These are reviewed in detail elsewhere, but the following is a brief summary:
The Coronary Drug Project21–24 is one of the earliest trials suggesting a role for niacin in the prevention of cardiovascular disease. Data showed that niacin was effective in favorably modifying blood lipid levels, and that this translated into a significant reduction of adverse cardiovascular outcomes persisting long beyond the discontinuation of treatment. Both the Familial Atherosclerosis Trial and the HDL Atherosclerosis Studies (FATS and HATS, respectively),25–27 demonstrated that combining niacin with a statin led to a 75% reduction in adverse cardiovascular outcomes, compared with a reduction of approximately one-third with statins alone. Furthermore, a sub-analysis of the HATS trial indicated that the HDL effects included a change in the subclass distribution, with niacin treatment eliciting an increase in the number of the large, buoyant cardioprotective particles. The ARBITER (Arterial Biology for the Investigation of Treatment Effects of Reducing Cholesterol)-228–30 and −331–33 trials arose from the original ARBITER study comparing the efficacy of high-dose atorvastatin (80 mg/day) with 40 mg/day pravastatin in 161 patients being treated for primary or secondary prevention of CV disease. The primary outcome measure was carotid intima media thickness, (CIMT) thought to be indicative of atherosclerotic burden, and this was significantly reduced in the atorvastatin group. This benefit was thought to be due to the reduction in LDL. ARBITER-2 therefore sought to investigate whether any additional benefit could be achieved with HDL modulation. 167 patients, established on statin therapy and receiving treatment for secondary prevention, were randomly assigned to receive either extended release niacin or placebo. The placebo group saw a significant increase in CIMT, an effect not observed for those receiving niacin. There was also a trend that suggested that this benefit was reflected in a reduced clinical event rate, although the study was insufficiently powered to prove this. The SEACOAST (Safety and Efficacy of a Combination of Extended Release Niacin and Simvastatin in Patients with Dyslipidemia) studies34,35 provided evidence that niacin and statin combinations were also particularly beneficial with regard to lipid modulation. Such combinations were at least as effective as a statin alone for reducing LDL-C, while they were significantly more effective in increasing HDL and reducing triglycerides. The Open-Label Evaluation of the Safety and Efficacy of a Combination of Niacin-ER and Simvastatin in Patients with Dyslipidemia (OCEANS) 36 demonstrated that the lipid benefits of once daily treatment with extended-release niacin and simvastatin were maintained during long-term treatment. These latter trials are concerned with the value of combining niacin with simvastatin, but trials such as ADVOCATE (The Advicor Versus Other Cholesterol-modulating Agents Trial Evaluation) revealed that other statins may be even more beneficial when used in combination with niacin and that such combinations also elicited favorable shifts in the density profiles of plasma lipoprotein particles.37,38
Although all of these studies seem to support the value of niacin as a valuable tool in the treatment of dyslipidemia, we are still lacking large outcome studies of niacin/statin combinations that will allow the therapeutic role of niacin to be fully determined. It is hoped that these question may be answered by the AIM-HIGH trial, which is discussed later in this review.
Benefits of Niacin Extend beyond the Effects on plasma Lipids
Modulation of plasma lipids has been shown to reduce atherosclerotic plaque formation and indeed induce regression of existing lesions.39,40 However, this is only part of the story. The development of atherosclerosis is primarily an immune response, thought to be triggered by endothelial injury and exacerbated by a host of risk factors. 41 Niacin favorably influences a number of facets of this process, thus conferring benefits outwith its lipid effects. 11 Fig. 1 describes the processes involved in plaque formation and indicates the role of niacin in each of these aspects. Plaque formation is an inflammatory response: circulating monocytes target the site of endothelial damage, where they leave the circulation and enter the intimal layer of the vessel wall. These cells differentiate into macrophages, which engulf oxidized (Ox)-LDL-C via the scavenger receptors SRA and CD36. 42 The accumulation of lipid within the cytoplasm (stored in specialized, adipophilin-coated vesicles) gives rise to the ‘foam cell’ appearance. Cytokine signals released by foam cells include monocyte chemoattractant protein-1 (MCP-1), which induces further monocyte migration to the site of the plaque.43,44 Other cytokines, such as IFN-γ, promote migration of smooth muscle cells from the underlying media. 45 Under the influence of these signals, these cells also undergo a change in gene expression, accumulating lipid and becoming smooth muscle cell-derived foam cells. They also secrete connective tissue, particularly collagen, forming a cap that stabilizes the whole structure. 46 Critical adverse outcomes are usually the result of breakdown of this connective tissue structure—rupture of the cap and exposure of the collagen acts as a site for thrombus formation, potentially completely occluding blood flow. 47 These events are dynamic in nature and progression in a given individual will depend on the interaction of these immunological processes and the risk factors present at that time. The lipid-lowering actions of niacin will lower the amount of LDL-C (and therefore Ox-LDL-C) reducing lipid accumulation within plaques. It is also worthy of note that unlike the LDL-receptor, expression of which is downregulated in response to high LDL-C-levels, scavenger receptor expression is increased when Ox-LDL-C levels are high. 48 LDL-C reduction therefore has the additional benefit of inhibiting the drive for lipid uptake into the plaque. The niacin-driven increase in HDL-C and ApoA1 also facilitates reverse cholesterol transport,49,50 meaning that the lipid effects of niacin profoundly effect plaque formation. However, in addition to this, signalling through HM74A provides ligands for the peroxisome proliferator-activated receptor-γ, activation of which will have a number of effects on the processes involved in plaque formation.10,11 Activation of PPARγ upregulates expression of CD36 (which may be considered to be a pro-atherosclerotic effect) but also enhances expression of ABCA1, another component of the ApoA1 mediated reverse-cholesterol transport pathway. 51 Activation of PPARγ also directly enhances expression of IKB, and thus inhibits NF-κB signalling, reducing expression of a number of pro-inflammatory cytokines that drive and maintain plaque formation.

Niacin favorably alters a number of aspects of intimal plaque formation. Some of these effects are indirect as a result of PPARγ-mediated inhibition of NF-κB.
Plaque stability depends on a number of factors, but it is known that destabilization is promoted by an increase in expression and activity of the matrix metalloproteinase MMP-9.46,47 Critically, MMP-9 activity appears to be lower in plaques that contain high levels of PGD2. Niacin's ability to elicit PGD 2 production may therefore enhance plaque stability.10,52,53
The use of niacin has also been associated with a number of other cardiovascular benefits, including a reduction in artery intima-media thickness as well as a reduction in the occurrence of stenosis, all of which are likely to improve vascular compliance.11,28,29,33 Niacin can also reduce both systolic and diastolic blood pressure. It is clear from the side effect profile that niacin is vasoactive: in addition to the cutaneous flushing discussed later in this review, there are other (rare) side effects including acute syncope and hypotension (including postural hypotension), especially when niacin is administered alongside other vasoactive medications. 54 However, there is little quantitative information available, although there are some clinical trials that included baseline and endpoint measurements of blood pressure as part of a range of clinical outcomes. One such study 55 demonstrated that acute administration of niacin had no effect on blood pressure in normotensive subjects. However, these results mask profound changes in hemodynamic parameters: there was a significant reduction in both stroke volume and systemic vascular resistance, but both systolic and diastolic blood pressures were maintained by a reflexive increase in heart rate. The response for hypertensive patients was somewhat different—infusion was associated with a small but significant decrease in diastolic pressure, as well as a drop in pulse pressure. As for the normotensive subjects, stroke volume and systemic vascular resistance were shown to be lower as a result of the niacin treatment, and an increase in heart rate was also observed. However, in the hypertensive subjects, this did not appear to compensate for the other hemodynamic changes. In normotensive patients, the blood pressure is likely to remain stable, because any significant peripheral vasodilation is likely to trigger vasoconstriction in other vascular beds as part of the autonomic homeostatic response. Such counter-regulatory responses may not be possible in patients with reduced vascular compliance, such as those with hypertension. This effect may be further exacerbated in hypertensives with abnormal baroreceptor responses, a condition not uncommon in diabetic patients who may have significant autonomic neuropathy.
The molecular explanation for the effects on blood pressure is unclear—and from a metabolic perspective it may seem anomalous. Treatment with niacin leads to a sustained rebound increase in FFAs which tends to provoke insulin resistance in skeletal muscle. One of the effects of normal insulin signalling is to maintain normal blood pressure by enhancing expression of endothelial nitric oxide synthase (eNOS). Thus it may be surmised that a state of niacin-induced insulin resistance may be accompanied by an increase in both systolic and diastolic pressures. In this particular study, the reduced blood pressure may simply reflect the short-term nature of the treatment.
This issue was considered in another study, which investigated the relationship between the effects of niacin on FFAs, insulin sensitivity and blood pressure. 56 This involved only seven patients, enrolled on a randomized, double-blind, placebo-controlled crossover study. During the first week, the treatment regime comprised a twice-daily dose of 250 mg immediate-release niacin, escalated to 500 mg twice daily for the second week. Interestingly, patients receiving niacin displayed a reduced sensitivity to insulin, although fasting glucose, insulin and FFA concentrations remained unchanged compared to placebo. Over the duration of the two-week study, there was no significant effect on either systolic or diastolic blood pressure.
However, these limited studies are not the only source of information with regard to the effects of niacin on blood pressure. Post-hoc analysis of data from the Coronary Drug Project reveals that long-term treatment results in a small but significant decrease in both systolic and diastolic pressures compared to placebo. 54
Overall, the evidence suggests that niacin is capable of eliciting a significant reduction in blood pressure, which would be yet another ‘plus point’ for overall cardiovascular risk reduction. Bays et al 54 suggest that this effect is related to the beneficial effects of niacin on plasma lipids. There is evidence to suggest that the ApoB:ApoA1 ratio inversely correlates with the extent of endothelium-dependent vascular smooth muscle relaxation, and that HDL-C may also increase expression and activity of eNOS. As niacin increases HDL-C and ApoA1 levels (whilst reducing ApoB) it may be expected that it would increase eNOS activity and thus reduce blood pressure. Consistent with this notion is the fact that the blood pressure response is slow and progressive and mirrors the timeframe of the change in HDL-C levels. One thing is clear: the effects of niacin on blood pressure need to be more extensively evaluated. Interestingly, the AIM-HIGH trial includes hemodynamic measurements, although this information is likely to be affected by the early cessation of the trial due, in part, to a slightly elevated risk of ischemic stroke. 57 Blood pressure is one of the outcomes being measured in the Heart Protection Study-2 Treatment of HDL to Reduce the Incidence of Vascular Events (HPS2-THRIVE) study, although this is assessing the efficacy of niacin combined with laropiprant. 58
Side Effects of Niacin Treatment
Niacin use is associated with hyperglycemia, partly resulting from an increase in glucose production in response to lower circulating FFAs, but also because the increased FFA levels associated with the niacin ‘rebound’ promote insulin resistance in skeletal muscle.59,60 The Assessment of Diabetes Control and Evaluation of the Efficacy of Niaspan Trial (ADVENT) 61 investigated the effect of extended release niacin on blood glucose and found that all doses were associated with an increase in fasting blood levels. However, most of the patients were on some kind of anti-diabetic medication (usually either metformin or a sulfonlyurea, but occasionally insulin) and it appeared that the hyperglycemic effects could be prevented by concomitant adjustment of anti-diabetic medication. Although higher doses of niacin were associated with a slight increase in HbA1c, levels, this only just reached significance and it is recommended that concerns regarding diabetic control should not put healthcare professionals off using niacin in the treatment of diabetic patients: the lipid-lowering benefits (and the associated clinical effect of reducing macrovascular complications) is likely to outweigh the slight reduction in glycemic control. 62 These results are backed up by the ARBITER studies28–33 which indicate that patients with diabetes see benefits of a similar magnitude to non-diabetics. Once again, AIM-HIGH is likely to provide further insight, as approximately one-third of the patients enrolled in this study are diabetics.
Other commonly cited side effects are those associated with hepatoxicity, 63 theoretically a greater risk with extended-release formulations because of the increased metabolism through the hepatic pathway.64,65 Hepatotoxicity can be recognized by an elevation in liver transaminases, with a sustained elevation of greater than 3 times the upper limit of the normal level being taken as a cause for concern. In practice, this is rarely seen and only accounts for a very small percentage of the drop out observed in clinical trials. Also of clinical relevance is the observation that none of the side effects discussed here are exacerbated by co-administration with statins. 11
Perhaps the most serious side-effect of niacin treatment is skin flushing.12,13,66,67 Although this is generally considered benign, it is distressing and not only affects initial compliance, but prevents the dose escalation required to reach the gram quantities necessary to achieve full clinical benefit. The recognition that the increase in the blood flow to the skin is caused by PGD2 acting on the DP1 receptor, and therefore independent of the HM74A-mediated effects on lipids, theoretically allows the flushing response to be targeted.
Extended release formulations (such as Niaspan-R™) have been a big step forward in improving tolerability, but skin flushing still remains the major reason for discontinuation. 11 Even with extended release formulations, some 90% of patients on 2 mg daily doses of niacin experience flushing, and studies have shown that by 3 months dropout rates can be as high as 92%. 68 Furthermore, the titration necessary to reach the therapeutic dose is still complicated, 68 requiring dose increments over a period of 4-5 weeks. Existing measures to combat flushing include treatment with aspirin, although this has limited efficacy. Patient education has also been shown to have an important role in improving compliance. 68
A Closer Look at the Flushing Response
As described above, many of the effects of niacin are mediated by its interaction with a G-protein coupled receptor. Signalling through Gi/Go pathways does not usually yield significant amounts of arachidonic acid (AA), although this is very much cell- and receptor-type specific: in immune cells particularly, HM74A has appears to synergize with Gq-coupled receptors, leading to an increase in intracellular Ca2+ concentration which mediates the translocation of activated phos-pholipase A2 to the cell membrane, where it catalyzes the release of AA. AA acts as the substrate for the enzyme commonly known as cyclo-oxygenase, which catalyzes the initial steps in the generation of eico-sanoids, including prostaglandins, prostacyclin and thromboxanes.69–71 More accurately, cyclo-oxygenase is an enzyme complex (PGH2 synthase) which has both peroxidase and cyclo-oxygenase activity. Aspirin and NSAIDs block this cyclo-oxygenase activity.
The overall effect of PGH2 synthase on AA is to produce the unstable endoperoxide intermediate PGH2. The fate of PGH2 will be determined by the cell-specific distribution of the prostaglandin and thromboxane synthase enzymes. 72 Many cell types possess either hematopoietic or lipocalin-type PGD2 synthase and thus are capable of producing large amounts of the acidic lipid mediator PGD2. PGD2 binds to and activates two distinct receptor types: DP1 and DP2 (also known as CRTH2), but it is also metabolized fairly rapidly: initially to PGJ2, and then to 15-deoxy-PGD2. This step is followed by further reactions which yield the cyclopentone prostaglandins, which include 15-deoxy Δ12,14 PGJ2, the endogenous ligand for the peroxisome proliferator-activated receptor PPARγ. 73 This prostaglandin is produced in sufficient quantities to activate PPARγ, 72 and many of the anti-inflammatory effects of niacin may well be mediated by this receptor, as discussed above.
Cell types that express PGD2 synthase—and thus produce PGD2 in significant quantities—include mast cells, which when activated by IgE, can produce up to 50 ng PGD2 per million cells. 74 Peripherally, other immune cells are known to be effective in producing PGD2, and one cell type relevant to the niacin story is the epidermal Langerhans cell.14,75 Stimulation of these cells with niacin has been shown to result in significant PGD2 release and it is generally considered that Langerhans cell-derived PGD2, acting on DP1 receptors in the vascular smooth muscle of dermal blood vessels, is responsible for the hyperemia associated with niacin treatment.
DP-1 Receptor
The DP-1 receptor is a Gs-coupled GPCR. Activation leads to an increase in cAMP, and therefore in PKA activity and the net effect in vascular smooth muscle leads to a profound vasodilation in dermal blood vessels.76,77 Since this effect is thought to be independent of the lipid-lowering benefits of niacin, the co-administration of niacin and DP1 antagonists has been suggested as an appropriate step forward in enhancing tolerability. However, there is some evidence to suggest that the currently held view with regard to the dermal effects of niacin may be somewhat simplistic.
Dunbar and Gelfand 75 suggest that the term ‘flushing’ is inaccurate in describing the effects of niacin on the skin, and significantly understates the nature of the problem. Rather than a simple hyperemia, they suggest that HM74A activation results in ‘an aggressive irritant effect on the skin.’ This is manifested as a response that bears a great deal of similarity to an acute hypersensitivity reaction. They argue that niacin administration elicits dermal infiltration with polymorph neutrophils within a matter of minutes, and the flushing is usually accompanied by significant swelling, paresthesia and pruritis, and suggest a better term for this collection of effects would be ‘niacin-associated skin toxicity.’ Indeed, most clinical studies focus on the measurement and assessment of the redness of the skin (rubor) and there is the concern that a reduction in rubor may not necessarily translate into an improved tolerability. 75 It seems likely that a number of cell types are involved in the adverse effects of niacin on the skin: there is certainly evidence for a role for macrophages and platelets. 7 Furthermore, even the issue of rubor is likely to be more complex—DP1 receptor knockout mice do not show a complete lack of a flushing response to challenge with niacin, 13 and it seems that the vasodilatory response is mediated at least in part by the release of PGE2, which acts on PGE2/E4 receptors. Similarly, clinical trials of the DP1 receptor antagonist laropiprant (discussed later) failed to demonstrate a complete abrogation of both objective and subject-reported measures.
Our understanding of the complex nature of the skin response to niacin has taken a step forward as a result of a series of experiments that have indicated that the Langerhans cell may be something of a minor player, and that the true mediator of the rubifacient properties of niacin may in fact be the keratinocyte. 76 Firstly, the authors demonstrated that HM74A is expressed by both murine and human keratinocytes, and that for both species, the receptor is indeed functional. Using Doppler flowmetry to measure dermal blood flow, they showed that in wild-type mice this flow could be seen to have a characteristic biphasic response: an initial transient rise followed by a slower onset, but sustained, major peak. HM74A knockouts show neither of these peaks, while replacement of the wild-type Langerhans cells with HM74A-null cells results in loss of the transient peak. Interestingly, it appears that the transient peak is mediated by the action of PGD2 produced by Langerhans cells in response to actions of COX-1. This is followed by the more sustained response of the epidermal keratinocytes, which release PGE2 as a result of COX-2 activity. PGE2 mediates its vasodilatory effects through the E2 and E4 receptors. 77 Each peak could be inhibited by pre-treatment with an appropriate COX inhibitor. 76
Lai and colleagues suggest that the hyperemia is one of the most persistent dermal effects of niacin, and continues well into treatment, even as patients are reporting that the symptoms of irritation are reducing. 78 This adds further support to the notion that the pruritis and other problems are not simply a result of increased blood flow to the skin, suggesting that DPI antagonism may not be completely effective in blocking the side effects of niacin treatment.
Role of PGD2
One of the arguments supporting the use of DP1 antagonists is the notion that PGD2 is a pro-inflammatory eicosanoid and therefore blockade is likely to confer additional benefit. Conventionally, the so-called ‘2-series’ eicosanoids, production of which is catalysed by the inducible COX-2 isoform, are considered pro-inflammatory.74,79,80 In addition, PGD2 has been shown to provoke vasodilation and bronchoconstriction, as well as mediating chemoattraction of eosinophils and TH2 lymphocytes. 78 Mice overexpressing the lipocalin-type PGD synthase in the lungs demonstrate enhanced features of asthma, 79 suggesting that inhibition of PGD2 production is associated with reduced allergic inflammation. However, there is an increasing body of evidence to suggest that the story is more complicated, one example being the cardiovascular problems associated with the use of selective COX-2 inhibitors.81–83 Of further interest is the observation that COX-2 inhibitors administered during the resolution phase actually prolong the duration of inflammation, suggesting that 2-series eicosanoids can have potent anti-inflammatory properties 84 and that these effects are context dependent.
Some of the anti-inflammatory effects of PGD2 are likely to be mediated by PPARγ as discussed earlier, but results of a number of studies suggest that many of the pro-inflammatory effects are mediated through its activation of the DP2 (CRTH2) receptor74,79 and that DP1 activation may actually mediate some of the anti-inflammatory effects.72,77,79,85 Certainly PGD2 is protective against neuronal damage caused either by glutamate excitotoxicity or by ischemia.77,86 PGD2 is the most abundant prostanoid in the brain, and both its receptors are also expressed by neuronal tissue.77,87 Cerebral ischemia is associated with induction of COX-2, which leads to an upregulation of PGD2 synthesis. DP1 activation in neuronal tissue triggers a PKA-mediated decrease in intracellular calcium which protects neuronal tissue against necrosis and apoptosis in the early phase of cerebral ischemia. Similarly, DP1 activation protects against glutamate-induced damage: the activated glutamate receptor triggers sodium and calcium influxes that increase intracellular osmolarity, leading to water influx and cell swelling. The calcium influx has the further effect of impairing mitochondrial function, resulting in a failure of the pumps responsible for maintaining normal ionic equilibrium and the swelling worsens. DP1 activation prevents the rise in intracellular calcium, largely as a result of PKA-mediated modulation of the activity of the SERCA pump which increases calcium uptake by the endoplasmic reticulum.77,86 The critical role of the DP1 receptor in this process is demonstrated by the fact that DP1 antagonism ablates this protective effect. These results led the authors to draw the conclusion that DP1 agonists are promising therapeutic agents for the treatment of acute cerebral ischemia and CNS problems associated with multi-infarct damage.
Other evidence supporting the notion that DP1 receptor mediated effects of PGD2 are anti-inflammatory is the observation that hematapoeitic PGD2 synthase knockout mice have a hyperinflammatory response, 72 an effect that can be rescued by treating the animals with a DP1 agonist. These knockout mice appear to have a compromised resolution phase which supports the notion that PGD2 is particularly critical in this phase. Treatment with a DP1 agonist stems fresh polymorph neutrophil influx to the site of inflammation and also promotes macrophage clearance.
Even in asthma, signalling through DP1 may be anti-inflammatory. Many studies have indicated a pro-inflammatory role for this receptor: DPI knockout mice have reduced signs of asthma 88 and PGD2 on its own can mimic the key features of allergic disease, including vasodilation, erythema and edema, as well as the recruitment of eosinophils and TH2 lymphocytes. 74 PGD2 activity also appears to modulate TH2 lymphocyte cytokine expression and also triggers bronchoconstriction. However, a study by Hammad et al 79 demonstrated that, in a mouse model, treatment with a DP1 agonist potently inhibits asthma, and that this affect appears to result from altered function of lung dendritic cells in response to DP1 signalling. Dendritic cells play role in mediating the allergic inflammatory responses associated with asthma because they express an number of antigens (such as CD86, CD40 and MHCII) known to be essential for inducing both naïve and memory effector responses in the lung. DPI agonists downregulate expression of these molecules, and have also been shown to reduce expression of cytokines involved in dendritic cell migration and maturation. 79 Some of the apparent problems associated with PGD2 activity in asthma may be independent of either receptor. DP1 signalling in bronchial smooth muscle causes bronchodilation, but in practice this seems to be overcome when concentrations of PGD 2 are particularly high and its ability to activate the TP receptor becomes significant. The TP receptor is Gq coupled and therefore leads to constriction of bronchial smooth muscle. 74
Other Effects Mediated by the DP-1 Receptor
Perfusion of rat brains with PGD2 induces sleep indistinguishable from physiological sleep, and PGD2 is secreted into the cerebrospinal fluid with a circadian rhythm. This suggests that PGD2 has an important role to play in the regulation of sleep and wakefulness, and this appears to be at least partially a DP1 mediated effect. 87 The DP1 receptor has also been shown to mediate the erectile response in a number of species, including humans One possible concern with DP1 anatgonists must therefore be impotence, which may already be of concern in patients with cardiovascular disease. 89 Another issue which may have particular relevance for diabetics is the observation that, in a mouse model, overexpression of PGDS led to an increase in PGD2 production in adipocytes. The effect of this was to stimulate adipogenesis and enhanced insulin sensitivity.90 While this seems likely to result from the generation of PPARγ ligands, a DP1 mediated-effect has not been ruled out.
Laropiprant
Laropiprant (MK-0524) is a potent (Ki 0.57 nM) orally active and highly selective antagonist of the DP1 receptor,91,92 originally developed as an anti-allergy agent. 68 Once-daily dosing is sufficient to achieve DP1 antagonism throughout the 24 period, which means that it is well-suited to combination with extended-release niacin, which is also given as a single daily dose. Concomitant administration of niacin and laropiprant has been shown to attenuate both incidence and intensity of flushing without affecting the lipid-lowering benefits seen with niacin alone.68,80,93 This reduction in flushing is seen both in terms of objective measures such as reduced malar perfusion, as well as subjective measures, such as patient-rated severity of pruritis, warmth and tingling. The improved tolerability associated with the use of laropiprant in combination with extended-release niacin has also removed the need for complicated titration regimes. 80
Following oral administration, laropiprant is rapidly absorbed. In a study by Karanam et al, 94 healthy human subjects were given a 40 mg dose of 14C-labelled drug, and peak plasma concentrations were observed within 1.5 hours, which is supported by the clinical trials described below which indicate that peak plasma concentrations are typically achieved between 0.8-2 hours after administration. 4 Laropiprant was rapidly metabolized in the liver and excreted in the bile, primarily via the acyl glucaronic acid conjugate, a process catalyzed by the enzymes UGT1A1, 1A3, 1A9 and 2B7. Phase I metabolites (hydroxylated and keto-derivatives) were also detected, although these accounted for only a minor part of the metabolism (and probably resulting primarily from CYP3A4 activity). Approximately 68% of the dose was recovered in the feces, with the rest accounted for by urinary excretion. Of the material retrieved in the feces, most of it was in the form of the parent compound and it is thought that this is the result of hydrolysis of the acyl glucaronic acid conjugate. Oral bioavailability was seen to be in the order of 80%. 94
Clinical trials also indicate that laropiprant concentration in the plasma undergoes a biphasic pattern of decline: initially, a rapid decrease is observed between two and four hours, followed by a slower decrease. The half-life appears to range from about twelve to eighteen hours. 4 Kinetic profiling appears to be similar for both single and multiple dosing, hence the development of Tredaptive™—a combination tablet consisting of a bilayer: one layer of controlled-release niacin (Niaspan-R™) and one layer of immediate release laropiprant, 1 g and 20 mg respectively. 20 This drug has received approval for the treatment of dyslipidemia in the European Union and other countries, but notably not in the US, where concerns remain about the use of laropiprant. 95
One potential problem is inhibition of CYP2C8, 92 an enzyme important in the metabolism of a number of drugs, with one of the most significant being the insulin-sensitizing PPARγ agonist rosiglitazone (Avandia™). Rosiglitazone is extensively metabolized—no unchanged drug can be detected in the urine—predominantly via CYP2C8 with a minor contribution from CYP2C9. Side effects include the increased risk of adverse cardiovascular outcomes which has prompted caution in the use of this drug, especially in patients with heart failure.96–98 Inhibition of CYP2C8 activity theoretically may potentiate this effect. A study by Schwartz et al 92 investigated the effects of laropiprant on the pharmacokinetics of rosiglitazone in normal healthy adults. This was an open-label, randomized, 2-period crossover investigation, comprising two treatments: A (1 × 4 mg tablet of Avandia™ on day 1) or B (40 mg, once daily dose of laropiprant for seven days, with a single 4 mg dose of Avandia™ on day 6). Each patient received both treatments, in random order, with a 3-day washout period between the two treatment phases. For patients on the Avandia™-only phase, blood samples were collected throughout the first 24 hours, while during the laropiprant/Avandia™ phase, blood samples were taken throughout. The laropiprant dose selected for this trial was the highest dose tested during Phase III clinical trials, and the results suggest that alone or in combination with rosiglitazone, it was well tolerated. Significantly, at this ‘maximum recommended dose’ laropiprant had no clinically meaningful effects on rosiglitazone concentrations, suggesting that inhibition of CYP2C8 is not relevant in practice. 92
Another concern is the possible effect of laropiprant on platelets. PGD2, acting through the DP1 receptor, is known to inhibit platelet activity. Activated platelets produce PGD2, and it is thought that this acts as negative feedback mechanism, preventing excessive activation. It follows, therefore, that DP1 antagonism may indirectly enhance platelet activity by blocking this negative feedback.20,78 However, this is not the only possible effect on the platelet: laropiprant has also been shown to be an antagonist of the TP receptor, albeit its potency is orders of magnitude lower than at the DP1 receptor. It is the TP receptor that mediates the powerful activation driven by thromboxane A2, and it may be that laropiprant acting in this capacity would inhibit platelet activation. While the role of the TP-mediated pathway in platelet function is well known, the contribution of DP-1 mediated effects is less clear. To explore this further, Lai and colleagues investigated the effect of laropiprant, niacin and combinations on platelet aggregation and bleeding time in normal subjects. This trial involved four treatments: extended-release niacin alone (2 g single daily dose), laropiprant alone (40 mg single daily dose), a combination of both drugs and placebo to all treatments. All patients received all treatments (in random order) and there was a seven-day washout period between each. Platelet aggregation in response to both ADP and collagen was measured, as was bleeding time. The assay used to measure platelet aggregation in this study was considered to be highly sensitive and possibly detected a mild transient inhibitory effect of laropiprant on platelet activation, but this was not sustained, and did not translate into any clinically meaningful effect on bleeding time. This backs up the results of the clinical trials (discussed later in this review) that indicate that there is no increase in bleeding time associated with laropiprant treatment even with doses up to 300 mg daily over a 4-5 week period. 78
Of course, platelet activation and subsequent aggregation involves more than just the platelet itself—endothelial mediators also influence the process. Platelet function in vivo can be assessed by measuring urinary 11-dehydrothromboxane and treatment with laropiprant did not significantly affect levels of this marker. Similarly, there was no change in levels of PGD2 and PGI2 as measured by their urinary metabolites. Overall, these studies appear to indicate that laropiprant has little or no effect on platelet function in vivo. 78
Clinical Trials concerning the Efficacy of Laropiprant with Respect to Lipid Parameters
Phase III trials have investigated the efficacy of extended-release niacin (ERN) and laropiprant with regard to lipid modulation (Table 1). Maccubbin et al 99 describe how an early phase III trial demonstrated a significant improvement in a number of lipid parameters compared to placebo including an 18.4% reduction in LDL-C, combined with a 20% increase in HDL-C. Furthermore, TG levels were reduced by over a quarter, while ApoB levels fell by 18.8% and ApoAl increased by almost 7%. These figures are similar to those observed with niacin alone, indicating that laropiprant does not attenuate the lipid benefits. Paolini and colleagues4,100 also looked at the impact of ERN/laropiprant on lipid levels and blood pressure although this was a short term study more concerned with safety and tolerability. A drop in LDL-C of 15% was observed, as was an increase in HDL-C of 20%. A second phase III trial 101 involved a much larger group of patients and looked at the effects of ERN/laropiprant in combination with a statin. 1398 participants were randomized to receive either 1000 mg ERN/20 mg laropiprant, simvastatin (10, 20 or 40 mg) or both, following a 6-8 week washout and a 4-week placebo/diet run-in period. After 4 weeks, the doses of ERN and laropiprant were escalated to 2000 mg and 40 mg respectively. The combination was shown to be more effective than simvastatin alone, with respect to all lipid parameters and this result was consistent across all patient groups. The increase in HDL-C was particularly impressive: 28% compared with 6% for simvastatin alone.
Summary of the main findings with respect to lipids of trials involving ERN/laropiprant combinations.
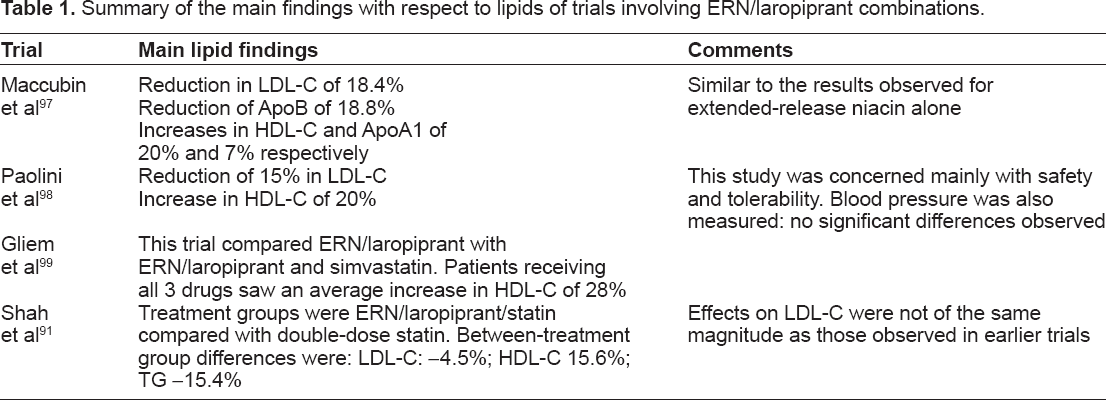
A more recent study by Shah et al 93 looked at combining ERN/laropiprant with either simvastatin or atorvastatin, and comparing the results to those obtained by simply doubling the dose of the statin. Once again, this was a short term study (12 week treatment period) and involved patients with primary hypercholesterolemia or mixed dyslipidemia. In this multi-center, randomized, double-blind, parallel study, one group of patients received either ERN/laropiprant in combination with either simvastatin (10 or 20 mg) or atorvastatin (10 mg). The other group received either simvastatin (20 or 40 mg) or atorvastatin 20 mg. The primary endpoint in this trial was the LDL-C level, but secondary endpoints included a range of lipid measurements (including HDL-C). Doubling the dose of statin proved more effective than the ERN/laropiprant/statin combination with regard to the effects on LDL-C levels, although it was interesting to note that the effects on LDL-C were less dramatic than those observed in other trials involving niacin and laropiprant. The authors suggest that the lack of a placebo comparator arm may have led to an underestimation in the magnitude of the LDL-C response. However, the effects of the combination drugs on all other lipid parameters was superior to those observed for the double-dose statin group, especially with regard to HDL-C.
The results so far with respect to lipid modification are promising. However, all studies so far undertaken are short-term and as yet do not make any assessment of clinical outcome. The HPS2-THRIVE study, 58 due to report in 2013 will go some way towards answering these concerns. Unfortunately, the ACHIEVE (Assessment of Coronary Health using an Intima-media thickness Endpoint for Vascular Effects) trial, which would have offered more insight in this regard has been halted, 102 although this is largely due to concerns that carotid intima-media thickness is not a robust surrogate endpoint.103,104
Effect of ERN/Laropiprant Combinations on Blood Pressure
There have been two trials so far involving ERN/laropiprant that have considered the effect on blood pressure. The first of these was the short term titration study by Paolini and colleagues described above. Involving 412 patients, it showed no significant effect on blood pressure. 100 However, a second larger study involving 1613 patients had different results. This was a worldwide, multicenter double-blind, randomized, placebo-controlled parallel study, beginning with a 4-week placebo run-in followed by a 24-week double-blind treatment period. 105 Participants’ ages ranged from 18-85 years and all had either primary hypercholesterolemia or mixed dyslipidemia. Patients were randomized to receive either ERN + laropiprant, ERN or placebo in a 3:2:1 ratio. Those on active treatment had an initiation period of 1 week on 1000 mg niacin/20 mg laropiprant, which was increased to 2 g/40 mg after this time. Both systolic and diastolic blood pressures were measured at baseline then at 4, 8, 12, 18 and 24 weeks. Treatment with either ERN or ERN/laropiprant was associated with significant sustained reductions in both systolic and diastolic pressures compared to placebo. These figures were similar to the 2-3 mmHg drop observed in the post-hoc analysis of the CDP data described previously.
Efficacy of Laropiprant as an ‘Anti-Flush’ Agent
There have been a number of trials that have specifically investigated the ability of laropiprant to attenuate the niacin flush. Most of the trials described above have assessed this aspect to some degree and there are other trials that have been solely concerned with this aspect.8,106,107 Regardless of the method of assessing the extent of flushing (subjective or objective) it is clear that co-adminstration of laropiprant with ERN significantly increases tolerability and allows optimal therapeutic dosing to be achieved, which is likely to improve the clinical efficacy of niacin. These studies also indicate that 20 mg laropiprant is the optimum dose to prevent the flushing induced by a 1000 mg niacin dose, whereas 40 mg is more effective at attenuating the flush caused by 2000 mg niacin. Currently, for the use of ERN, a 4-step titration regimen is recommended. The use of laropiprant removes some of the need for this process, and the currently recommended strategy is the two-step regimen described by Gliem and colleagues above. 101
It is, however, worth stating again that DP1 antagonism does not completely abrogate the flushing response. Drop-out rates due to flushing are vastly improved, but they are still significant. For example, in the study by Bays et al, describing the effect of ERN/laropiprant combinations on blood pressure, 105 of the 1613 participants, 453 discontinued treatment. 35.7% of the patients receiving ERN alone discontinued: this is not unexpected and is in line with previous studies assessing the tolerability of this agent (this compared with a dropout rate of 11.5% for the placebo group). However, the dropout rate for the group receiving ERN/laropiprant was still 28.5%, which is conistent with other studies that suggest that the dropout rate due to flushing with laropiprant is still around 25%.9,106,107
This is perhaps not unexpected given the considerable body of evidence to suggest that the flushing effect is also PGE2 mediated. Aspirin and NSAIDs have been used in the past to attempt to attenuate the flush but this has not been particularly successful.108–110 A phase I trial, reported by Dishy et al 9 looked at the possibility of further reducing the skin toxicity of niacin by combining ERN/laropiprant with aspirin. Participants were all healthy non-smoking men and non-pregnant women aged between 18-75. This was a double-blind, double-dummy, randomized, placebo-controlled cross-over study with three treatment periods. There were four treatment combinations: each participant received three of these treatments and the sequence of treatments was randomized. Treatment A comprised ERN 2 g/laropiprant 40 mg plus placebo to aspirin 325 mg. Treatment B was ERN 2 g/laropiprant 40 mg plus aspirin 325 mg. Treatment C was placebo to both the ERN/laropiprant and aspirin treatments, while treatment D was ERN 1 g/laropiprant 20 mg plus aspirin 325 mg. All participants received treatments A and B at some point during the study and also received either treatment C or D. Aspirin (or placebo to aspirin) was administered 30 minutes prior to the treatment with niacin/laropiprant or its appropriate placebo. The treatment period was 3 days and flushing was assessed using a flushing symptom questionnaire. Interestingly, the results indicated that there was no significant benefit conferred by pre-treatment with aspirin.
Safety and Tolerability
Generally, laropiprant has been shown to be well-tolerated. Many of the potential concerns have been shown to be of little practical consequence in the short studies so far conducted. Guidance issued by the International Conference on Harmonisation states that early phase clinical testing of novel drugs should involve an assessment of the effect of that drug on the QTc interval. 111 Prolongation of the QTc interval is of particular concern because it may cause potentially fatal ventricular tachycardias such as Torsades de pointes. A study by Luo et al 112 involved a double-blind, randomized, placebo-controlled, double dummy, four-period balanced crossover study, which involved the administration of a single dose of laropiprant (either 50 or 600 mg) and found that even the 600 mg dose, which is far in excess of the maximum clinically used dose, was well-tolerated and did not prolong the QTc interval relative to placebo.
Although the potential effects of laropiprant on platelet activity appear to have no clinical relevance, it is possible that it may be of concern to patients who are receiving anti-coagulation therapy, which is of particular relevance to the patient groups most likely to benefit from lipid-lowering therapy.113,114 A study by Schwartz et al indicates that there are no significant effects of laropiprant on the pharmacokinetics and pharmacodynamics of warfarin. 115 Especially important is the observation that there is no significant change in the INR meaning that it is likely that ERN/laropiprant combinations can safely be used in patients on warfarin.
Both niacin65,116–119 and statin61,120–123 treatment have the potential to elevate liver transaminases. Most of the trials involving laropiprant have indicated that there is an increase in the number of patients experiencing more than one elevation ≥3 times the upper limit of normal ALT or AST levels. These did not appear to be problematic: they were asymptomatic and resolved rapidly following discontinuation of treatment.93,100,107 However, these are all short-term studies, and it may become more of an issue when higher statin doses are used. For this reason, it is currently recommended that patients receiving laropiprant combinations should have liver function tests performed at 3 months and 6 months after the initiation of treatment and every six months thereafter. Similarly, the myopathy associated with statin use124–126 does not appear to be aggravated by laropiprant treatment. 90 The evidence also suggests that adding laropiprant to ERN does not exacerbate the effects of niacin on glycemic control. 93
AIM-HIGH: Challenging the HDL Hypothesis?
The Atherothrombosis Intervention in Metabolic syndrome with low HDL/high triglycerides: Impact on Global Health outcomes (AIM-HIGH) trial was a large-scale multi-center study designed to answer the question as to whether or not extended-release niacin can further reduce cardiovascular risk in patients whose LDL-C levels are already well-controlled. 3414 patients were enrolled, and inclusion criteria included the presence of established CV disease and atherogenic dyslipidemia. Diabetes was not an exclusion criterion. Patients received simvastatin at a dose required to reach a target LDL-C of 40-80 mg/dL, although ezetemibe could also be added to the treatment if the statin alone was insufficient to achieve the target LDL-C. Patients were then randomized to receive either placebo or extended-release niacin (2000 mg/day, or 1500 mg if the higher dose proved difficult to tolerate). The study began in 2005, and was due to finish in September 2012, with the primary outcome measure being a composite endpoint of CHD death, non-fatal MI, ischemic stroke, hospitalization for non-ST segment acute coronary syndrome or a symptom-driven coronary or cerebral revascularization. 127 However, the trial was halted in May 2011, because the study aim of reducing risk by an additional 25% could not be met, 128 although the supposedly beneficial lipid alterations were achieved. This underlines the importance of measuring clinical outcomes rather than relying on surrogate endpoints, 129 but the full impact of the results remains to be seen.
Conclusion: Place in Therapy
Despite the recent controversy generated by the cessation of AIM-HIGH, which has led some to suggest that treatment goals should remain focussed on LDL-C lowering, 130 there is an extensive body of evidence to support a wider approach with regard to lipid modulation and ERN is well-proven in this regard. Combination with laropiprant is effective in reducing the side effects and does not appear to attenuate the clinical benefits. However, the present studies are all short-term, whereas the development of cardiovascular disease is most certainly a chronic condition. Especially in light of the considerations with regard to the potential anti-inflammatory benefits of DPI signalling, it is critical that longer-term studies are undertaken not only to back up the initial findings, but to ensure that the benefits with regard to lipid modulation extend to clinical risk reduction. Health care professionals should be aware of the potential risks and remain vigilant to prevent a repeat of the sort of issues observed with rosiglitazone.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributor-ship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.