
Abstract
Aims
This study investigated the prognostic value of B type natriuretic peptide (BNP) in acute myocardial infarction (AMI) patients and its relation with left ventricular function and post-myocardial infarction complications.
Methods
In this cross-sectional study, plasma BNP level was measured for 42 consecutive patients (mean ± SD: 61.6 ± 10.85 years old) with acute ST elevation myocardial infarction (MI) and 42 healthy, age and gender matched subjects.
Result
BNP level in AMI patients were significantly higher than control group (@P < 0.001). Regarding to infarct location, the highest BNP level measured in inferoposterior MI (BNP = 4436.63 ± 6188.159 pg/ml) and the lowest one indicated in standalone inferior MI (BNP = 598.83 ± 309.867 pg/ml (P = 0.071). There was significant reverse relation between BNP and EF (P = 0.006, OR = −0.47) and a significant relationship between BNP and killip classification (P = 0.036). There was no significant relation between diastolic and right-ventricular function and BNP level (P = 0.61, P = 0.21). The highest BNP level was detected in LV septal rupture and false aneurysm (P = 0.02) and in ventricular tachycardia, but without significant relationship (P = 0.25).
Conclusion
After the onset of AMI, BNP blood level can be used as an important predictor for left ventricular dysfunction, killip classification, early mechanical complications and cardiac death.
Keywords
Introduction
Natriuretic peptides are released from the heart, in situations of pressure and volume overload of the ventricles. During the last decade, B-type natriuretic peptide (BNP) has been proposed as a useful marker for the determination of acute and chronic left ventricular dysfunction and the severity of systolic left ventricular dysfunction.1,2
BNP is a 32-amino acid neurohormone synthesized in the form of pre-proBNP, which is firstly cleaved to pro-BNP, and then to active BNP and inactive fragment NT-proBNP.
In the first hours of acute myocardial infarction, BNP is released as a result of ischemia and necrosis of myocardial cells. Afterwards, BNP rises as a result of systolic and diastolic dysfunction and increased wall stress of the left ventricle.3–5 There have been several evidences, supporting that variation in plasma BNP level during acute phase of AMI, can be used as a prognostic factor. 1 Moreover, new studies has shown that plasma BNP level, measured in acute coronary syndromes, independently might predict mortality rate, heart failure and degree of expansion of myocardial infarction.6,7
Although, BNP plasma level is measured routinely in AMI patients, but it is not fully determined, level of it how is useful in acute phase MI, for estimation of left ventricular ejection fraction (LVEF), diastolic dysfunction and other acute complications. This survey designed for elucidation of these issues. Moreover, we sought to investigate the prognostic value of BNP in different MI locations, as well as its relationship with different EF levels, right ventricular function, killip classification (as delayed mortality rate and early AMI complications indicator), gender, pulmonary artery pressure and major electrical and mechanical complications.
Method and Materials
Study Population
Study population in this cross-sectional and observational survey included forty two consecutive patients with acute ST elevation MI (aged 61.6 ± 10.85, male = 27) who referred to emergency heart department of Ghaem Medical Center (Mashhad, Iran) from January 2007 until January 2008. These patients were in the initial three days of event. Diagnosis of acute myocardial infarction was confirmed via ST segment elevation in initial EKG and cardiac enzymes measurement.
Demographic information and vital signs, major risk factors (like hyperlipidemia, obesity, diabetes and smoking), para-clinical data, infarction location and electrocardiogram results were gathered by questionnaire for each patient on admission.
During hospital stay (after the third day of admission until pre-discharge date) transthoracic echocardiography (TTE) was performed for all the patients by VIVID3 machine (GE-USA) with 2.5-3.5 MHZ probe according to ASE/AHA guidelines. All related information concerning LV size, systolic and diastolic function, valve dysfunction, pulmonary artery pressure level, right ventricular function and mechanical complications of AMI were evaluated and all results were recorded. Afterwards, all the patients were followed up for fourteen days after admission. Forty-two consecutive healthy, age and gender matched, subjects were recruited for control group, as well.
The study protocol was approved by the medical ethics committee of the Mashhad University of Medical Sciences (MUMS).
BNP Analysis
Blood samples were obtained from the patients and controls, using plastic tubes containing ethylendiaminetetraacetic acid (EDTA) and aprotinin (50 ka/ml). Plasma was separated by centrifuge technique at 300 rmp, 4 degree Celsius and stored at minus 80 degree of Celsius until analysis. Plasma BNP level was measured by commercial immunodimetric assay method.
Statistical Analysis
SPSS for Windows, version 11.5 (SPSS Inc., Chicago, IL, USA) was used in all statistical procedures. Data were expressed at mean ± SD. with 95% confidence interval (CI) calculated by maximum likelihood ratio estimation method. Differences in proportions were judged by χ2 test. Comparison of BNP levels between the two independent groups (patients with or without specific cardiac diagnosis) was made using the Mann-Whitney test. A two-tailed P-valve >0.05 was considered statistically significant.
Results
Demographic Data
Demographic data of the current study, such as hypertensive, hyperlipidemic and diabetic subjects, and the other characteristics were comparable (Table 1).
Demographic and base line clinical variables and plasma BNP level for AMI studied patients and control group.

Percentages in the parenthesis reflect the total number of patients for whom data were available
Plasma BNP level
Mean plasma BNP level in the patient group (3784.57 ± 6344.97 pg/ml) was significantly higher than the control group (68.35 ± 69.66 pg/ml) (P < 0.001, Table 1).
BNP and Gender, Age and Pulmonary Artery Pressure
Mean plasma BNP level in male patients was 3008.12 ± 6889.354 pg/ml while its level in male control subjects was 70.75 ± 76.561 pg/ml (P < 0.001). Likewise, female subjects had significantly higher mean plasma BNP level in comparison to female controls (3841.75 ± 5616.783 pg/ml vs. 64.75 ± 60.048 pg/ml) (P < 0.05). In both groups BNP mean rates were not significantly different, according to gender of the participants (P = 0.97). There was slight positive relation between BNP levels of AMI patients and age (P = 0.01, r = 0.39). Mean pulmonary artery pressure in the patient group was 41.88 ± 11.24 mmHg. Considering 35 mmHg as a cut-off point, pulmonary artery pressure was normal in 17 (37.5%) but increased in 25 (62.5%) of the patients. However, there was no significant relationship between BNP level and pulmonary artery pressure (P = 0.36, r = 0.24) (Table 1).
BNP and MI Location
The site of infarction was anterior in 41.9% (mean BNP level = 4208.92 ± 508.067 pg/ml), inferior-posterior in 25.8% (4436.63 ± 688 pg/ml), isolated inferior wall infarction in 19.4% (598.83 ± 309.867 pg/ml), inferior right ventricle in 12.9% (1462 ± 141.297 pg/ml) of the patients. The highest level of BNP was in posterior-inferior MI and the lowest one in isolated inferior wall MI. There was no significant relationship between BNP levels and infarction location (P = 0.13) (Fig. 1).
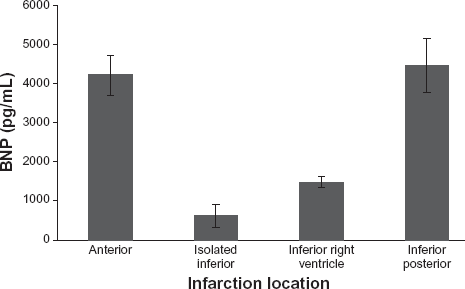
Relationship BNP level (pg/ml) and MI location.
BNP and Mechanical Complications
Between 42 studied patients, 11 individuals (27.5%) had mechanical complications, between this group, two individuals (18%) had free wall rupture (mean BNP level = 7310.50 ± 6760/648 pg/ml) septal rupture in one patient (12091 pg/ml). Left ventricular aneurysm in four patients (34%) (10995.50 ± 14960.840 pg/ml), false aneurysm of left ventricle in one patient (9%) (12091 pg/ml) and left ventricular clot observed in three patients (29%) (3969.26 ± 6486.318 pg/ml). Mean BNP levels was the highest in the patients with septal rupture and false aneurysm complications with significant different (P = 0.02).
Ejection Fraction (EF), Diastolic Function Association with Bnp
The average of left ventricular EF in the patients was 47.55% ± 11.07%, and there was significant reverse association between BNP level and EF (P = 0.006, r = −0.47, (Figure 2). EF was also strongly associated with age and pulmonary artery pressure (PAP) rate (P < 0.05).

BNP level (pg/ml) association with ejection fraction in AMI patients.
It is understood that one of the most important consequences of acute ischemic attack and AMI is diastolic function disorder (DFD). In our study 28 patients had impaired left ventricular relaxation, (Grade one), seven in Grade two and seven others in advanced DDF (Grade three). There was no significant relation between diastolic dysfunction grade and BNP level (P = 0.61).
BNP and Right Ventricular Function
In studied group, 33 patients (82.5%) had normal right ventricular function with mean BNP level 4762.21 ± 7952.59 pg/ml, and nine patients (17.5%) had right ventricular dysfunction with mean BNP level 2315.43 ± 2010.25 pg/ml. There were no significant relationship between BNP mean level and right ventricular function (P = 0.21).
BNP and Major Electrical Complications
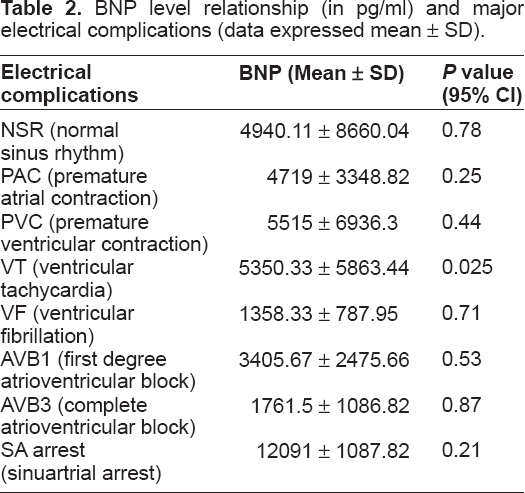
Our findings represent the highest BNP levels belonging to patients with PVC, junctional rhythms (5515 ± 6936.3 pg/ml) (P = 0.44) and VT rhythm (5350.33 ± 5863.44 pg/ml) (P = 0.25). Lowest BNP level was measured in SA-arrest (1209.51 ± 1086.81) (P = 0.21), but no significant difference between BNP levels and other major electrical complications was observed (P < 0.05). (P = 0.21, Table 2).
BNP level relationship (in pg/ml) and major electrical complications (data expressed mean ± SD).
BNP and Killip Classification
According to killip class 1, 2, 3 and 4, from all the patients, 13 (32.5%), 19 (47.5%), 8 (20%) and 2 (12.5%) patients were allocated, respectively. There were significant relations between BNP mean level and different killip classes (P = 0.036).
Discussion
AMI is a major mortality cause and in spite of recent diagnostic and therapeutic improvements; mortality and morbidity rate of this condition is already remained high. Recently, B-type natriuretic peptide (BNP) has been recognized as a useful marker for predicting acute and chronic left ventricular dysfunction. Patients with acute ST elevation myocardial infarction (STEMI) who had higher levels of BNP have been shown to have worse prognosis.8–12
This study aimed to determine BNP level in AMI patients and its comparison to the healthy subjects. Besides, to evaluate the association of BNP level with left ventricular dysfunction and mechanical complications induced by AMI assessed, as well.
Morita et al have indicated that plasma BNP level was increased in 50 AMI patients in comparison to control group. 13 In the mentioned survey, maximum BNP level was reported, to be prone to rise, in the first 16 hours following admission, more than 50% of normal range, as a second peak. 13 Yang et al (2007) studied on 246 AMI patients with 14 months follow-up and investigated several indexes, as like as BNP to determine the most valuable prognostic factors for AMI induced mortality, They found, with multiple regression analysis, that BNP is an independent risk factor and an appropriate prognostic index for mortality rate estimation, in short and long term after AMI. 14
As presented in the current study, Yoshida et al reported that female MI patients had significant higher BNP levels, than male MI patients, independent from their age. 15 However, in our study there was no significant difference between the genders in mean of BNP level, which may be due to the smaller number of patients as a limitation.
It seems BNP basal level would be a prognostic LVEF indicator. 16 Kallistratos et al understood that plasma BNP level is related to LVEF, and aerobic capacity can predict lower cardiopulmonary function and exercise capacity in the patients with impaired LVEF. 17 Likewise, in our study; significant reverse correlation between EF and BNP level confirmed.
In recent studies on AMI patients with ST segment elevation, BNP has been recognized an important prognostic indicator of early and delayed complications of infarction,18–24 as well as Killip class. Grabowski et al in evaluation of 126 AMI patients with ST segment elevation, found that in higher Killip classes, BNP levels is more likely to be increased. They found out, mortality rate in Killip class I and BNP below 321 mg/ml was 1.1% while for Killip more than one and BNP more than 331 mg/ml, this risk increases to 55.6%. 25 As well in our study, according to higher killip class, BNP level increased significantly.
Kaya et al (2008) found that plasma BNP level in posterior AMI with right ventricular involvement is higher than isolated posterior infarction. 26 The current study approved this finding, but BNP level in different infarction locations did not showed significant relationship regarding this measurement.
On the other hand, it is understood, as well as pulmonary artery pressure—an indirect indicator of left ventricular diastolic dysfunction and left ventricular volume overload-, BNP levels were also increased and this relationship confirmed in our study. Besides, present study findings investigations demonstrate positive correlation among BNP increased level and older age of the patients.
It seems, according to left ventricular pressure overload, secondary pulmonary hypertension and right ventricular dysfunction, BNP level is likely to increase. 27 In our study, even though, increased BNP level was associated with right ventricular dysfunction, but it was not strongly confirmable.
Furthermore, Bettencourt et al 27 reported relationship between BNP level and diastolic function, but in the present study, no significant relationship between BNP level and grade of diastolic dysfunction was found.
Satton et al demonstrated BNP level increases in accordance with MR severity, 28 therefore; we investigated this association in our study, and among eleven patients with mechanical complications, maximum BNP level (12091 pg/ml) was belonged to LV septal rupture cases and false aneurysm, and the lowest BNP level measured for LV clot.
Blangy et al reported that together with serving as a marker of left ventricular dysfunction, BNP level is marker of Ventricular Tachycardia (VT) as well, and increased serum BNP was associated with a higher incidence of VT. 29 Although, there are few evidences about BNP levels and major electrical complications.
In our studied group, 26 patients (65%) had major electrical complications (Table 2). Maximum BNP level was observed in the patients with premature ventricular contraction (PVC) and ventricular tachycardia (VT) disorder, while the lowest BNP level was measured in the patients with sinuartrial arrest rhythm disorder. However, generally there was no significant difference between subgroups of the patients with other electrical complications.
Conclusion
The findings of this study confirmed previous hypotheses and brought important information, regarding the BNP prognostic role on acute MI and acute complications happening after 3rd days of admission, meanwhile pre-discharge time.
Accordingly, we assumed, the first, plasma BNP level could be useful as an important and valid predictor of left ventricular systolic dysfunction, as a reverse relation of BNP levels and LVEF is observed in AMI patients. Second, BNP elevations in higher Killip classifications and mechanical complications, strongly confirmed prognostic role of BNP in AMI patients. Therefore, it seems that measurement of plasma BNP level in early phase of myocardial infarction may be useful as a non-invasive method for identification of individuals, at higher risk of complications and post-MI mortality.
Limitations
Effect of type of treatment, on BNP level was not assessed in present study. Besides, we could not recruit more than forty two patients due to the high cost of plasma BNP measurement. Finally, short-term follow up of our patients, confined to 14 days is another limitation.
Conflict of Interest
None of the authors of the manuscript has declared any conflict of interest meanwhile conduction of the current study, for being named as an author on the manuscript.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributor-ship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.
Footnotes
Acknowledgements
The authors greatly acknowledge Research Council of Mashhad University of Medical Sciences (MUMS) for financial support of this study. The authors are also thankful to the personnels of echocardiography lab, CCU ward and Moayeds laboratory staff for their kind cooperation.