
Abstract
Restenosis after sirolimus-eluting stents (SES) remains a clinical problem. We report our experience with the use a second SES in the first SES to treat in-SES restenosis. Twenty-seven patients with in-SES restenosis were included in the registry. In-SES restenosis was focal in 34%, diffuse in 59% and proliferative in 7%. The procedure was successful in all patients without any acute in-hospital complications. During a mean follow-up of 14 ± 7 months MACE occurred in 8 patients (30%), (1 death, 1 myocardial infarction, 4 target lesion revascularisation, 1 target vessel revascularisation and 1 patient underwent CABG). Nineteen patients (70%) had an event-free outcome. In conclusion SES placement to treat in-SES is safe and feasible and could be considered as a therapeutic option. However the incidence of MACE remains high on a long-term period.
The use of stents has significantly improved the outcome of percutaneous coronary interventions (PCI) (1,2). However, despite major advances in angioplasty and stenting, in-stent restenosis remains a major limitation. Recently, drug-eluting stents and especially sirolimus-eluting stents (SES) have emerged as a very promising approach in preventing restenosis, and several different compounds have been shown to have a major impact on both the angiographic and the clinical outcome (6-9). However, even after drug eluting stents implantation in-stent restenosis (ISR) remains and represents a clinical challenge. Several approaches have been proposed to deal with ISR like plain old balloon angioplasty (POBA), rotational atherectomy, brachytherapy (1-3). Few reports are actually available about the use of SES in SES for ISR treatment. We report our experience about the use SES for treating an ISR after SES implantation.
Method
Between March 2004 and April 2006 all patients with in-SES restenosis that were not optimally treated by plain old balloon angioplsty received a second SES (Cypher and Cypher select, Cordis, Miami Lakes, Florida) within the first one (re-SES). The procedural data of these consecutive patients were included in a registry. The institutional review board of both participating institutions approved the study. Eligible patients provided written informed consent. The study complied with the Declaration of Helsinki regarding investigations in humans.
Procedures were performed via a femoral artery approach. A 5 or 6 French guiding catheter was used. All patients were pre-treated with aspirin 100 mg/day. Intravenous heparin (70 U/kg) was given at the beginning and a 300 or 600 mg loading dose of clopidogrel was administered at the end of the procedure. Standard interventional techniques were used to treat the patients and performed at the discretion on the in-charge operator. Intravascular ultrasound was not used. Angioplasty with a «power-grip» balloon was performed in all patients before implantation of the second new SES stent. A successful procedure was defined, as a residual stenosis <20 percent and the absence of major adverse cardiac event during the in-hospital stay.
After the procedure, patients were monitored in an intermediate care unit. CK, CK-MB values were measured at least once on the morning of the following day. A 12 lead ECG was recorded at the end of the procedure for all patients, and further tracings were obtained if indicated by the clinical course. Patients were discharged the same day or on the day following the procedure. Aspirin 100 mg/day was given long term and clopidogrel 75 mg/day was prescribed for 12 months.
Quantitative coronary angiography evaluation was obtained in multiple views. Analyses were performed before, during and after the procedure after administration of intracoronary nitrates. For patients with angiographic follow-up, restenosis was defined as a 50 percent or more reduction of the luminal diameter occurring within the 5 proximal and distal segment millimeters of the stented.
Clinical follow-up was obtained by a visit or by telephone contact with the patient or his/her referring physician. The pre-specified primary end point was a composite of major adverse cardiac events (MACE), defined as cardiac death, myocardial infarction, and ischemia-driven revascularization of the target lesion. Secondary end points included ischemia-driven revascularization of the target lesion (TLR), target-vessel revascularization (TVR), and target-vessel failure (TVF). TLR and TVR were considered to be driven by ischemia if the stenosis of the target lesion or vessel was >50% on the basis of quantitative coronary angiography in the presence of ischemic signs or symptoms, or if there was a stenosis of >70% in the absence of ischemic signs or symptoms. TLR was defined as a repeated revascularization based on a stenosis within the stent or within the 5-mm borders proximal or distal to the stent. The diagnosis of myocardial infarction (MI) after the intervention was established whenever new Q-waves of at least 0.4 seconds duration in at least 2 contiguous leads appeared on the electrocardiogram with an elevated creatine kinase MB fraction level, or in the absence of pathologic Q waves, an elevation in creatine kinase levels to more than twice the upper limit of normal with an elevated creatine kinase MB or troponin I level. Stent thrombosis was defined as an acute coronary syndrome with angiographic documentation of either target vessel occlusion or thrombus within or adjacent to the previously successfully stented segment.
Statistical Analysis
Values are expressed as mean ± standard deviation. The Fischer's exact test was used for statistical analysis. A two tail p value <0.05 was considered to be of statistical significance.
Results
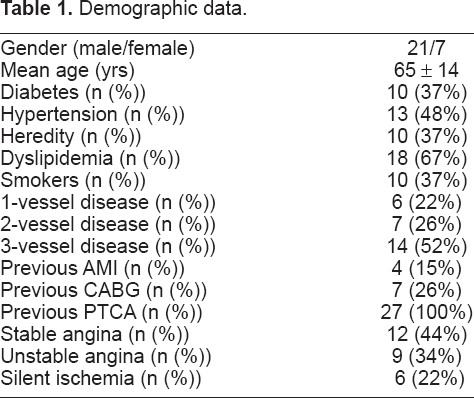
During the study period 3802 percutaneous interventions were performed. Hundred and four patients underwent plained old balloon angioplasty (POBA) because of focal restenosis. Twenty seven patients (0.1%) patients who had in-SES restenosis which could not be treated solely with POBA, were included in the registry. The demographic and clinical data are presented in Table 1. All patients were already treated with dual antiplatelet agents (aspirin and clopidogrel). This combination is routinely administered for 1 year after implantation of SES. A high percentage (37%) of patients were diabetics and more than a half had 3 vessel disease. The angiographic characteristic of the lesion are presented in Table 2. Most of the patients had a pattern of diffuse restenosis (54%), although proliferative restenosis was rare (7%). In 7 patients the stent was located in a saphenous vein graft. The procedure was successful in all patients and a mean number of 1.1 ± 01 stents/patients were implanted. The minimal lumen diameter increased from 0.73 ± 0.44 mm to 3.27 ± 0.5 mm. No patients experienced in-hospital complications.
Demographic data.
Angiographic data.

At the end of a mean follow-up of 14 + 7 months, 19 patients were still free of adverse events (70%). Major cardiac adverse events (MACE) occurred in 8 patients (30%). Two patients died, one from a cardiac cause and one from a non cardiac cause. Six patients required additional revascularisation, 4 (15%) had a target lesion revascularisation (TLR), one (4%) had a target vessel revacularisation (TVR) and one (4%) underwent CABG. Among the patient requitring TLR, 2 (50%) had a focal restenosis.
Even rare, in-stent retenosis following SES implantation remains a clinical relevant problem in 4 to 10% of the treated population. Several approaches exist to overcome this drawback like balloon angioplasty, brachytherapy, stent in stent implantation or rotational atherectomy. As reste-nosis occurred in SES, it seemed logic to implant a second SES in the first one. The concept is that a second implant with an additional dose of sirolimus on the same lesion might be more efficient than the first one, the reason for this inefficiency remaining unclear. In addition very few data are actually available in the literature about the re-SES treatment. It could, thus, be interesting and important to have long-term data on this approach. Our group of patient is a somewhat different from the real world population with more diabetics (almost 40%) and patient with saphenous vein graft disease. However this is not surprising since diabetics and patients with SVG angioplasty are more prone to have restenosis even after SES implantation (5). Our data confirm the feasibility and the safety of this procedure and our results are very similar to the 24% of MACE, at 8 months, recently reported by Torguson et al. in a group of patients with re-SES, and are consistent with data from Lemos PA et al. who reported a MACE rate of 29.2% at 9-month follow-up in DES-patients with in-stent restenosis (9). The long-term clinical outcome after re-SES is not as good as after SES implantation for de-novo stenosis since the incidence of MACE is approximately 30%, mainly due to a second restenosis. This is not surprising since most of our patients had complex (proliferative or diffuse) restenosis. However, even focal restenosis can recurred as we have seen in 2 of our patients. For non-diabetic patients we can hypothesize that the pattern of the lesion (non-focal, focal, proliferative, diffuse) as already documented for any DES (6), or the efficiency of the stents (how and how long the drug is delivered, how the stent is set in etc.) could give an explanation for the recurrence of the stenosis. Paclitaxel stent implantation could be an alternative, as these stents have been shown to be efficient in diabetic patients. However, we decided not to use these stents to avoid interaction due the application of several different drugs on the same site.
Clinical outcome at a mean follow-up of 14 ± 7 months.

Our study confirms that re-SES placement is safe and feasible. The technique allows to treat most of the patients with in-SES restenosis. However, this does not represent a miraculous solution but an alternative to other percutaneous or surgical options. It should be reserve to patients with diffuse or proliferative restenosis. In patients with focal reste-nosis, balloon angioplasty will certainly remain the best option, at least for a first restenosis.