
Abstract
Aims
We evaluated the relationship between distribution of lesions in coronary tree and atherosclerotic renal artery stenosis (RAS).
Methods and Results
Data collected prospectively on 500 consecutive patients who underwent simultaneous renal angiography following coronary angiography. Overall prevalence of RAS was 26.2% (131 patients). Significant (≥ 50% luminal diameter stenosis) RAS was present in 70 patients (14%). In 346 individuals of the study population, significant CAD was present (69.2%). Significant RAS was more common (18.4%) in this group. Older age, higher intra-arterial systolic blood pressure (SBP) and pulse pressure (PP) at the time of catheterization, and 3-vessel coronary artery disease (CAD) were associated with significant RAS in univariate analysis. Relationship between involved locations of coronary arteries [Left anterior descending (LAD), left circumflex (LCX), Right Coronary Artery (RCA), and their ostioproximal portions] and RAS were significant except for left main (LM) disease. In multivariate model, age more than 62 years, SBP greater than 150 mmHg, PP in excess of 60 mmHg and RCA involvement were independent predictors of significant RAS.
Conclusion
Simultaneous renal angiography following coronary angiography might be justified in patients with significant RCA disease who are older with increased levels of intra-arterial SBP and PP.
Introduction
Atherosclerotic renal artery stenosis (RAS) is an important and frequently unrecognized contributor to refractory hypertension (HTN), ischemic nephropathy, and cardiac destabilization syndromes (unstable angina, flash pulmonary edema, and decompensated heart failure).1–5 Atherosclerotic RAS is a progressive disease leading to renal atrophy over time and chronic kidney disease despite control of HTN.6–13
Presence and severity of incidental RAS is an independent predictor of mortality in atherosclerotic patients regardless of the mode of treatment of underlying coronary artery disease.13–15
The prevalence of RAS has been reported to be in the range of 20-30 percent in high risk populations including patients with known atherosclerotic vascular disease elsewhere.16–18 In these patients invasive screening for RAS is highly cost-effective especially when done at the time of another invasive diagnostic procedure like cardiac catheterization, and may affect treatment strategies. 19
Atherosclerosis is a diffuse process but affects certain regions of the vascular bed preferentially. The association between extent and severity of CAD and RAS has been well established in most previous studies,12–14 but a few has been addressed the relationship between the distribution of lesions in coronary tree and RAS.2,8,14
The main purpose of our study was to find out if any association exists. In parallel, we evaluated the relationship between demographic variables, atherosclerotic risk factors, renal function, and levels of intra-arterial pressures during catheterization and RAS. In conclusion, we postulated that these findings might help decide in which group of patients screening renal angiography could be justified following coronary angiography.
Methods
Over a period of 12 months from November 2008, data collected prospectively on 500 consecutive patients who underwent simultaneous renal angiography following coronary angiography in Shaheed Rajaie Cardiovascular Medical, and Research Center.
The indications for coronary and renal angiography were at the discretion of the attending cardiologist. Demographic variables, laboratory data, and history of atherosclerotic risk factors obtained from the patients’ medical record.
Patients considered hypertensive, if they had a positive history of HTN who were under life style modification and/or medical treatment. Patients considered diabetic (DM) as either currently taking anti-diabetic medications or having more than one fasting plasma glucose (FPG) ≥ 126 mg/dl on laboratory record. Dyslipidemia (DLP) defined if the patient was under medical treatment for known dyslipidemia or any of the following laboratory criteria existed: Fasting low-density lipoprotein cholesterol (LDLc) ≥130 mg/dl, high- density lipoprotein cholesterol (HDLc) ≤40 mg/dl in men and ≤50 mg/dl in women or triglycerides ≥150 mg/dl. Patients considered having a history of smoking if they were current or former smokers. A positive family history (FH) established based on a known history of CAD in a first degree relative male or female less than 45 and 55 years respectively. Glomerular filtration rate (GFR) estimated by the four variable modification of diet in renal disease (MDRD) equation using plasma creatinine concentration, age, and gender.
According to the catheterization laboratory routine practice, all of these patients underwent abdominal aortography following coronary angiography using a pigtail catheter and 10-20 degrees straight left anterior oblique (LAO) projection with a pump injector at a rate of 15 ml/sec. In those patients for whom it was difficult to evaluate the degree of stenosis via aortography, selective renal angiography also performed using a right judkins catheter and 0-20 degrees straight LAO projections with hand injection. By average, about 30-40 ml additional contrast media were utilized which was either Ultravist-300 (Shering AG, Germany) or Visipaque-320 (GE Healthcare, Ireland). No procedural related complications with either method reported. Data on contrast-induced nephropathy (CIN) was not available.
Significant RAS defined if luminal-narrowing ≥50 percent was present. Coronary disease considered ostioproximal if it observed before first diagonal or septal branch in LAD artery, before first sizable obtuse marginal (OM) branch in LCX artery and before the first bend of the vessel in RCA. All angiograms digitally recorded at 15 frames/sec speed and interpreted at a consensus of two interventional cardiology fellowships.
Statistical Analysis
All collected data entered into a database and subsequently analyzed using SPSS software version 15.0 for windows (SPSS). The relationship between RAS and other variables was examined using student's T-test for normal continuous variables and Chi-square test for categorical factors. Continuous variables that revealed significant relationship with RAS in univariate analysis categorized according to their distributions and entered into the multivariate model. Numerical variables expressed as mean ± standard deviation (SD) and categorical factors as percentages. Finally, independent predictors of RAS derived by multivariate stepwise logistic regression analysis and expressed as odds ratios (OR) with 95% confidence interval (CI).
P value of 0.05 or less considered statistically significant.
Results
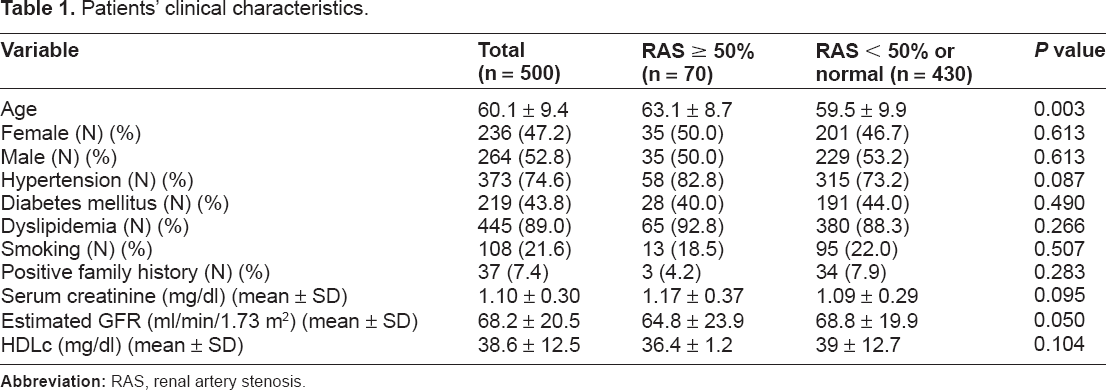
In these cohort of patients, 264 (52.8%) were male with mean age of 59.6 ± 10.1 years and 236 (47.2%) were female with mean age of 60.8 ± 8.7 years. As for major atherosclerotic risk factors, 373 patients (74.6%) had HTN, 219 patients (43.8%) were diabetics, 445 individuals (89%) had DLP, 108 (21.6%) of them were smoker and 37 subjects (7.4%) had a positive FH (Table 1).
Patients’ clinical characteristics.
Prevalence of RAS with any degree of stenosis was 26.2% (131 patients). Significant RAS was present in 70 patients (14%). It was unilateral in 46 patients (9.2%) and bilateral in 24 (4.8%). In 26 (56%) of patients with unilateral disease, RAS was detected on left renal artery and in 20 patients (44%) right renal artery was involved. High-grades stenosis (≥70% luminal narrowing) was present in 45 (9%) of them [37 (7.4%) unilateral, 81 (1.6%) bilateral, 18 (49%) on the left side and 19 (51%) on the right] (Fig. 1).

Severity and sidedness (left, right, and bilateral) of renal artery lesions.
Patients with high-grade stenosis underwent renal artery stenting at the same setting or differed intervention for another session. Patients with moderate (50%-70%) stenosis referred to nephrologists for further assessment about intervention or medical therapy. In 346 individuals, significant CAD was present (69.2%). Significant RAS was more common (18.4%, P < 0.001) in this group. In the remaining 154 patients (30.8%) with either normal coronaries or insignificant CAD, six subjects (1.2%) had significant RAS in which all were high -grade stenosis (bilateral in one). Significant RAS was more common in patients with three vessel CAD compared to those with single or two vessel CAD. Relationships between involved locations of coronary arteries and RAS were significant except for LM disease (See Table 2).
Catheterization characteristics.

Patients with significant RAS were older compared to those without significant disease. Neither sex nor other atherosclerotic risk factors showed any association with significant RAS. Borderline relationships observed between significant RAS, serum creatinine, and eGFR levels (Table 1). Because almost all patients were receiving statins, which has modest effect on HDLc (less than 10% increase in HDLc) compared with other components of lipid profile, 1 only this parameter statistically analyzed.
Mean intra arterial systolic, diastolic and pulse pressures during catheterization were 172.8 ± 30.7 vs. 161.6 ± 29.2 mmHg for systolic BP, 85.1 ± 14 vs. 78.8 ± 21.5 for diastolic BP and 87.7 ± 23.7 vs. 78.8 ± 21.5 for pulse pressure with significant RAS compared to those without demonstrating a good relationship between systolic and pulse pressures but not diastolic BP and RAS.
At the end, by multivariate logistic regression analysis age more than 62 years (OR 2.12; 95% CI 1.16 to 3.48, P = 0.013), SBP greater than 150 mmHg (OR = 3.19; 95% CI 1.57 to 6.46, P = 0.001), PP in excess of 60 (OR = 3.82; 95% CI 1.11 to 13.09, P = 0.033) and RCA involvement (OR = 3.76; 95% CI 1.89 to 7.48, P < 0.001) were independent predictors of significant RAS. LAD artery disease showed borderline significance (OR 2.12; 95% CI 0.94 to 4.79; P = 0.069). Results of the models for RAS ≥ 70% were almost similar to RAS ≥ 50% in both univariate and multivariate analyses.
Discussion
Prevalence of RAS with different severities and of bilateral RAS in this cohort of patients undergoing coronary angiography is within the range of most other studies.
Our study showed no difference in patients with significant RAS compared to those without with respect to major atherosclerotic risk factors except for age. This may reflect that traditional risk factors have a limited potential for predicting RAS. Dzielinska et al 5 and Wang et al 12 were reported similar results, but considerable variability seen in many other studies.
In our study, age more than 62 years was an independent predictor of RAS. In a number of studies, this issue addressed with different thresholds, in which it was more than 60 years at a minimum.6,9 We also found borderline relationships between serum creatinine, eGFR levels, and RAS. In most studies reduced levels of eGFR (specifically less than 60 ml/min/1.73 m2) discovered to be an independent predictor of significant RAS.
Bearing in mind that not all patients with even severe RAS have uncontrolled HTN, renal failure or other clinical clues1,12 and the fact that well proven anti-atherothrombotic medications which block rennin-angiotensin system may act as a two edged sword in the presence of significant but clinically unsuspected bilateral RAS1,3 underscores the need to step beyond traditional screening for RAS. Additionally hemodynamically significant RAS may have several deleterious systemic effects through activating this system, which may accelerate atherogenesis and contribute to cardiovascular events.13,14
There was a good relationship between intra-arterial systolic and pulse pressures and RAS, which is in agreement with study of Weber-Mzell et al 8 and Rihal et al. 18 In our study, systolic BP above 150-mmHg and pulse pressure in excess of 60 mmHg found to be independent predictors of significant RAS. Wide pulse pressure may simply reflect more advanced arteriosclerosis and renal disease and in a recent published study of Dieter et al, 20 pulse pressure > 100 mmHg was shown a powerful predictor of poor outcome following renal angioplasty and stenting. We found highly significant relationships between atherosclerotic involvement of LAD, LCX, and RCA and RAS, which remained significant in their ostioproximal segments; this was not true for significant LM disease. As for number of coronaries involved, patients with three vessels CAD showed strong relationship with RAS and those with normal coronaries or insignificant CAD had a potent negative association with RAS. Interestingly in multivariate model, three vessels CAD no longer seen as an independent predictor of RAS while RCA involvement was a strong independent predictor of RAS and LAD artery disease showed borderline relationship. As far as we know this independent relationship between atherosclerotic disease of RCA and significant RAS not been reported before.
The predilections of certain sites in vascular system to develop atheroma are clear. 1 Atherosclerotic RAS predominantly affects the aorto-ostial segment, 1 but relationship between distribution of coronary artery lesions and segments involved has not been addressed extensively.
In a study by Weber Mzell et al, 8 LAD, LCX, and RCA stenosis were more frequent in patients with significant RAS but in multivariate analysis, having >2 significant coronary lesions recognized as an independent predictor of RAS. In another study by Conlon et al, 14 LAD disease was more frequent in patients with RAS ≥ 75%. There was no relationship between anatomical distribution of coronary artery lesions (proximal, mid or distal portions) and RAS in a study by Danesh et al, 2 but two and 3-vessel coronary disease reported as an independent predictor of significant RAS.
Although the therapeutic implications of incidentally detected RAS has been remained controversial until now 21 it may be valuable to be aware of this condition given the progressive nature of the disease, the precautions in prescribing angiotensin antagonists and possibly the need to revascularization in appropriately selected cases.
Given the considerable drawbacks of noninvasive imaging techniques1,2,13 and safety of renal angiography13,16,17 recognizing potential candidates for screening of RAS based on readily available variables at the time of cardiac catheterization is important from a practical point of view. Patients with incidental RAS may deserve aggressive medical treatment and more close follow-up.
Conclusion
Simultaneous renal angiography at the time of coronary angiography might be justified in patients older than 62 years, with increased intra-arterial systolic pressure (≥150 mmHg) and pulse pressure (≥60) and RCA disease in the absence of traditional clinical clues.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
Acknowledgements
We greatly appreciate all interventional cardiology fellowships and catheterization laboratory staff of the Shaheed Rajaie hospital for their cooperation in data collection.