
Abstract
Backgrounds
In recent years, low levels of Insulin-like Growth Factor-1 (IGF-1) have been suggested to be associated with higher risks of developing heart failure and higher long-term mortality rates following Acute Myocardial Infarction (AMI). However, the effect of IGF-1 levels on short-term survival has been rarely studied. In this study we aimed to assess any possible association between serum IGF-1 concentration following AMI and short-term survival rates.
Methods
In this study, serum total IGF-1 levels were measured in 56 patients within 24 hours following AMI and were compared to 56 individuals with no cardiovascular disease. Patients were followed up to death or discharge from hospital (median = 6 days) and survival curves were compared based on median IGF-1 value.
Results
Mean (±SD) of serum IGF-1 levels were 232.73 ng/ml (±81.74) and 211.00 ng/ml (±58.22) in survived and expired patients respectively and the difference was not statistically significant (P value = 0.501). The difference between survival curves was also not statistically significant (P value = 0.246).
Conclusion
According to findings of this study, serum total IGF-1 concentration does not seem to be associated with short-term survival rates.
Introduction
Insulin-like growth factor-1 (IGF-1) is involved in the growth and development of many cells,1–5 including cardiac myocyte. 6 In addition, it has been found to interfere with apoptosis and cellular death in various tissues7–9 including myocardial cells.10,11 IGF-1 is synthesized mainly by the liver and kidneys but also, in a paracrine and autocrine way, by endothelial and vascular smooth muscle cells and by cardiac myocytes.1,2
In recent years, low levels of IGF-1 have been suggested to increase the risk of developing cardiovascular disease particularly myocardial infarction.12,13 Moreover, data analyses based on Framingham and Rotterdam studies have reported low levels of IGF-1 to be associated with the risk of developing heart failure.14,15 Further studies have emphasized the stimulating effect of insulin like growth factors on left ventricular remodeling and long term survival following myocardial infarction.11,13,16,17
However, the effect of IGF-1 on short term survival in the acute phase of Acute Myocardial Infarction (AMI) has rarely been studied. The aim of this study was to evaluate serum IGF-1 levels following AMI and assess its possible association with short-term survival rates.
Methods
In this cross sectional analytic study from March 2008 to July 2009, of 167 patients referred to the Coronary Care Unit of Rasoul Akram Hospital for management of suspected myocardial infarction, 111 patients were excluded (70 patients didn't provide informed consent, 15 had hypertension, 10 had BMI > 30, 5 patients had acromegaly and 11 patients had chronic inflammatory disease). This left a study population with following inclusion criteria: age <80 years, AMI diagnosed by WHO criteria and LVEF on admission >45%.
Subjects who were investigated as the control group had normal EKG without any history of chest pain or diabetes mellitus and were selected from patients admitted to Rasul Akram Hospital for ophthalmic problems. They did not consume any drugs which could interact with IGF-1.
All participants gave written informed consent for inclusion in the study. The study protocol was approved by the Ethics Committee of the Iran University of Medical Sciences (Tehran, Islamic Republic of Iran).
Blood Sampling
A 5-ml blood sample was achieved from all patients within 24 hours of CCU admission, and centrifuged. Then serum was separated and sent for measurement of IGF-I. Concentration of IGF-1 was evaluated using radioimmunoassay. The normal range of this assay is 107 ng/ml to 310 ng/ml. We also measured fasting blood sugar and lipid profile on the day after admission.
Patients were divided into low and high IGF-1 groups, using median concentration of IGF-1 as the cut-point. All patients were followed until they were discharged from hospital or expired.
Statistical Analyses
The Student's T-test was used for comparison of IGF-1 concentration between patients and control groups. Survival curves were constructed by the Kaplan-Meier method and compared by log-rank test. Data are mean ± SD. P < 0.05 was considered significant. All tests were done with SPSS 16.0 (Statistical Package for Social Sciences) for Microsoft Windows.
Results
A total of 56 patients with a mean (±SD) age of 58.53 (±11.68) were enrolled to the study. Table 1 shows baseline characteristics of the MI affected group. Serum IGF-1 levels of 56 healthy controls aged 60.12 (±6.16) was also measured as an estimate of normal IGF-1 values.
Baseline characteristics of MI affected patients.
Comparing AMI affected patients and control group, mean (±SD) levels of serum IGF-1 were 230.02 ± 79 ng/ml and 307.46 ± 64 ng/ml respectively and the difference was statistically significant (P value < 0.001) (Fig. 1).
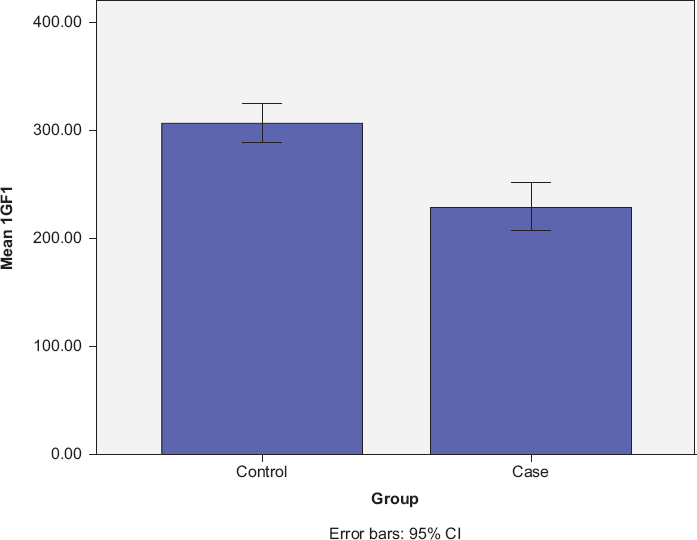
Mean IGF-1 levels (ng/ml) in control and case groups.
Among the patients, seven died of cardiovascular events. Three patients expired on the first day of admission, one on the second day, two on the third day and one on the fourth day. Table 2 compares a number of cardiovascular risk factors between this group and surviving patients, revealing statistical significance for none of the variables.
Comparison of baseline characteristics between survivors and expired patients.

No statistical significance could be found in the correlation between levels of IGF-1 and duration of hospitalization (P = 0.086). Mean IGF-1 levels were 232.73 ng/ml (±81.74) and 211.00 ng/ml (±58.22) in survived and expired patients respectively and the difference was not statistically significant (P value = 0.501).
Survival curves were constructed according to the median value of serum IGF-1 in the first 24 hours following acute myocardial infarction and are shown in Figure 2. The difference between curves was also not statistically significant (P value = 0.246).

Survival: long rank P value = 0.246.
Discussion
In this study, IGF-1 levels in the first 24 hours following acute myocardial infarction were found to be lower in the comparison with the control group. Event analysis was also performed to detect any possible difference of survival curves between higher and lower levels of IGF-1 while the analysis did not demonstrate a statistically significant distinction.
Previous studies have also documented a decrease in IGF-1 levels following MI.12,13,18 These reduced levels have been shown to return to control level within one month and cytokine reactions are assumed to be responsible for this reduction. 18 Besides these findings, previous reports have also documented lower levels of IGF-1 to be associated with higher risks of developing heart failure and higher long term mortality rates following acute myocardial infarction.14–17
Unlike our study, a study published in 2008 18 reported significant difference in 90-day survival rates according to the median value of IGF-1. As the sample size of the mentioned study and our study's are very close to each other (54 and 56), sample size is very unlikely to be the cause of this mismatch. Instead, there is methodological difference between these two studies. The study followed patients for longer and reported 90-day survival while we followed them up to the time of discharge. Thus it might be possible that the other study reports sub-acute survival instead of acute survival rates.
In conclusion, we did not detect any significant role for serum IGF-1 levels in short-term survival of MI affected patients in the acute phase of their disease. As there is disagreement between the results of this study and a previous study, addressing a similar question but with a different methodology and definition of short-time survival, further studies are suggested to assess the compact of IGF-1 on short-term mortality rates in which the definition of “short-term” should be carefully determined.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.