
Abstract
Background
High morbidity and mortality characterize patients suffering infective endocarditis (IE). The treatment of IE has undergone significant changes within ten years but it is not known whether mortality has decreased and which factors are determinant of the outcome.
Objectives
Our aim was to evaluate the prognostic significance of clinical characteristics and outcomes of IE.
Methods and Results
312 definite cases of IE diagnosed using the Duke criteria were evaluated. Overall in-hospital mortality was 28%. Independent predictors of death, determined by a Weibull regression model, in medically-treated patients were (1) treatment era 1990-1995 vs. 2005-2007 (hazard ratio 3.14; 95% CI 1.37-7.21); (2) aging for each year (hazard ratio 1.02; 95% CI 1.004-1.03); (3) cardiac complications (hazard ratio 1.91; 95% CI 1.06-3.43); and (4) heart failure (hazard ratio 2.27; 95% CI 1.34-3.85). Independent predictors of the death in surgically-treated patients were (1) treatment era 2001-2004 vs. 2005-2007 (hazard ratio: 0.31; 95% CI 0.10-0.97), (2) aging for each year (hazard ratio: 0.96; 95% CI 0.94-0.99), and (3) cardiac complications (hazard ratio: 1.91; 95% CI 1.01-3.63).
Conclusions
Some of the predictive factors for a poor prognosis were the same as those observed in previous studies. These factors could be used to identify those patients for more aggressive treatment. A new finding was the hazard function for mortality being highest at enrollment and declining rapidly in both medically and surgically treated patients, especially during the first 12 months.
Despite changes and improvements in healthcare delivery and effort, infective endocarditis (IE) remains a severe disease with elevated short- and long-term mortality. The poor prognosis for IE is not only due to the high rate of in-hospital mortality and early complications but also late-emerging sequelae from the infection. The short-term prognosis for IE has improved as a result of recent progress in diagnostic techniques, antibiotic treatment and improved early detection of complications.
Prior studies of IE reported in-hospital and long-term mortalities >20%,(1-7) and evaluated the predictors of death. Cabell et al. 8 found an association between infection with Staphylococcus aureus and death. Recently, Hasbun et al. 9 derived and validated a scoring system for clinical variables used to predict the 6-month survival in complicated IE. These variables included comorbid illness, heart failure, infective organism and surgery.
Previous studies defined the clinical findings which have prognostic significance and mortality; however, some inconsistencies between the results from different hospitals were evident. Our specific aims were to analyze the clinical characteristics of an entire cohort, prognostic factors, short- and long-term mortality. In particular the study focused comparing combined medical and early surgical treatment with medical treatment alone.
Methods
We performed combined retrospective (1990 to 1999) and prospective studies (2000 to 2007, data on all patients admitted at two tertiary referral hospitals (the university hospitals). The Duke criteria 10 were used as the diagnostic standard.
Data Collection
For each patients the following information was recorded.
Gender and age.
History of prior heart disease, prosthetic valve and infective endocarditis.
Echocardiographic findings: vegetations, valve ring abscess, degree of valvular regurgitation and destruction.
Current IE: location, symptoms and physical signs, number of positive blood cultures, causative microorganisms. The date and time of any in-hospital events of surgery and death were available from each patient's case-report form. The need for surgical treatment was recorded for all patients for the period from admission to discharge. In addition to hospital records, where needed, the date of death was obtained from the National Population Registry.
Indications for surgery during the active phase of infective endocarditis.

Persistent fever and/or positive blood cultures for the same pathogen after 1 week of appropriate antibiotics.
Statistical Analysis
To determine predictors of patient survival, a parametric survival analysis, using Weibull regression was conducted separately; one for the patients who underwent medical treatment and the other for those who underwent cardiac surgery. Statistical analysis based on the Weibull regression is able to detect if there was the non-constant risk of dying, the likely finding for IE. The model would reveal a parameter estimate of an underlying hazard function whether the risk of dying would be decreasing or increasing over the specified period. For the medically-treated patients, the primary outcome was months from diagnosis to death or censor and the predictors included: era of treatment (1990-1995, 1996-2000, 2001-2004 vs. 2005-2007), patient's age and sex, presence of cardiac complications, New York Heart Association classification (NYHA) and duration of symptoms. For the cardiac surgery patients, the time to event was counted in months from surgery and the predictors were the same, except the duration of symptoms was replaced by time to surgery.
Results
Among the 312 patients identified in our cohort, both medically and surgically treated, the hazard showed a decreasing trend over time. The underlying hazard was highest at enrollment but it was lower in the surgically-treated patients (Fig. 1), than in the medically-treated patients (Fig. 2). The risk of dying in both groups of patients then declined rapidly, especially during the first 12 months after enrollment.

Hazard-function estimate for overall mortality in patients who underwent surgery.

Hazard-function estimate for overall mortality in medically treated patients.
General Characteristics
During the study period, 312 were treated for IE, of whom 92% and 8% had native and prosthetic valve endocarditis, respectively. The mean age of the cohort was 41 (±15) years, with a range of 15 to 82 years. Two-thirds (205) of the patients were male and 107 (34%) were female (Table 2).
Characteristics in 312 cases of Infective Endocarditis.

NVE indicates native valve endocarditis. PVE indicates prosthetic valve endocarditis.
Chronic Obstructive Pulmonary Disease.
Blood Cultures and Microorganisms
Streptococci were the most frequent microorganisms (41.5%), Staphylococci (both coagulase positive and coagulase negative) were responsible for 14.5 per cent. Negative blood cultures but nevertheless, had clinical, surgical, or pathological findings supporting the diagnosis of IE in 40 per cent. (Table 3).
Causative pathogens of 312 cases of Infective Endocarditis.
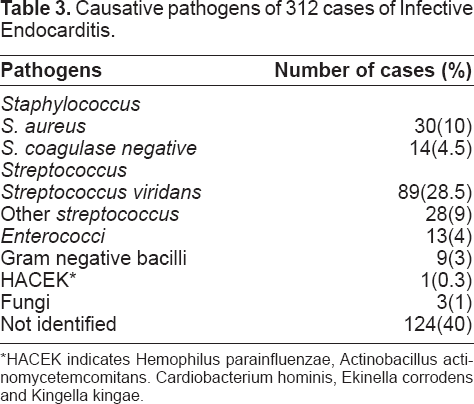
HACEK indicates Hemophilus parainfluenzae, Actinobacillus actinomycetemcomitans. Cardiobacterium hominis, Ekinella corrodens and Kingella kingae.
In-hospital complications
As shown in Table 4, cardiac and extracardiac complications in-hospital were very common, 82% of the cases (n = 256) were associated with at least one severe complication. The most common complications were congestive heart failure due to valve regurgitation or prosthetic valve dysfunction.
Incidence of severe complications in 312 cases of infective endocarditis.

Other cardiac complications indicates valve ring abscess, myocar-dial abscess, conduction abnormality, pericardial effusion.
CNS indicates central nervous system: rupture mycotic aneurysm, cerebral embolism, brain abscess, meningitis.
Serum creatinine >2 mg/dL.
Treatment
All patients received antibiotics treatment. Of the 171 patients (55%) underwent valve surgery. Early surgery was more common than emergency surgery (Table 1). The most common indication for surgery was congestive heart failure (63% of all indications). The proportion of patients who underwent surgery increased significantly by the treatment eras (30% vs 64%, p < 0.001). (Fig. 3).

Comparison between surgical and medical treated patients and mortality during difference periods.
Mortality
Overall in-hospital mortality was 28%. The mortality by year is shown in Figure 4. The most common cause of death was due to cardiac and co-morbidities. In-hospital mortality deceased significantly between 1990 and 2002 in patients who underwent surgery. During follow-up, 42 patients (18% of the survivors of the active phase of IE) died. The causes of late death were congestive heart failure secondary to progression of the underlying cardiac lesion, and unknown etiologies.

Overall mortality and proportion of patients who underwent surgery and medical treatment per year.
Effect of surgical versus medical treatment alone on mortality as shown in Figure 5. Both in- hospital and long-term mortalities were significantly lower in patients treated surgically than in medically treated patients.

Comparison of Kaplan-Meier curves demonstrating improved overall survival with surgical treatment compared to medical treatment alone.
Factors Predicting Mortality
Patient Characteristics
The factors predicting mortality in the medically treated patients are presented in Table 5. Patients having IE between 1990-1995 significantly predicted mortality compared to the other treatment eras (Fig. 6). Other significantly predictive factors of mortality included cardiac complications, congestive heart failure (NYHA class IV) and increasing age.
Factors Predicting Overall Mortality Of Medically Treated Patients.


Kaplan-Meier survival curves. Overall survival in medically treated patients between periods.
The factors predicting mortality in the surgically-treated patients are presented in Table 6. Patients with IE during the treatment era 2001-2004 had significantly less mortality than the other treatment eras (Fig. 7). Age and cardiac complications were similarly significant predictors.
Factors Predicting Overall Mortality Of Surgically Treated Patients.


Kaplan-Meier survival curves. Overall survival in surgically-treated patients between periods.
Discussion
Physicians caring for IE patients need to be able to accurately identify patients at high risk of early death in the course of their illness. One challenging aspect of this disease is the dynamic nature of clinical, microorganism and echocardiographic findings in the active phase. Our study included IE patients over a 18-year period in order to demonstrate the clinical factors apparent in the early course and predict in-hospital mortality. Recognition of these factors may allow for more intensive treatment of these patients and improve outcomes.
Previous studies have defined various clinical findings, which have prognostic significance in patients treated for IE.14–18 This may be due to differences between the institutions or patient populations or even between environmental or genetic factors. We defined the prognostic factors in IE patients in a relatively large cohort at a tertiary care hospital and compared the outcomes and predictive factors between the old and new IE treatment eras. Ours was the first study to determine the hazard-function estimate for mortality in an IE cohort using the Weibull regression model. The analysis result suggested that mortality was highest at enrollment and declined rapidly with a decreasing risk overtime.
Effects on Mortality
Since the time of the first successful implantation of a prosthetic valve during active IE, one of the practice questions in patients with active IE is whether they would benefit from early valve surgery. 19 Potential risks of surgery in the active phase of infection have to be weighed against the potential unfavourable course of medical treatment only.
Operative mortality in IE has been declining steadily from 9%-37% 20 in the past to 2%-12%21–22 in recent years. The need for late valve surgery was more common in patients treated medically during active IE, although this pattern is consistent with most previously published data, 23 the necessity for late valve surgery after medically treated infection was considerably lower in our study (26%)
Tonos et al. 23 , and Castillo et al. 24 did not find a better survival rate following early surgery in their populations with native valve endocarditis. Study by Vlessis et al. 25 showed an association between early surgery and improved survival over five years.
In our study, regarding the assessment of the role of cardiac surgery, performed in 55% of all cases regardless of the type of IE during their hospitalization, was higher than that reported in other studies (15%-34%).26–29 The patients who underwent cardiac surgery were significantly increased by year (Figs. 3,4). Overall mortality rate of 55% with medical treatment was compared to 29% mortality rate for surgical treatment (Fig. 5). However, the patients who received medical treatment were very heterogeneous—the group comprised both those at low risk with good prognosis without any complications and those indicated for surgery that could not be performed because of high surgical risk with a poor prognosis especially in the early period (1990-1995).
Congestive heart failure (CHF) was present in 78% of this cohort and was independently associated with in-hospital death among both medically- and surgically-treated patients. CHF and the need for late surgery were the most frequent causes of morbidity.23–24 The timing of congestive heart failure in the course of IE may influence mortality. Roder et al. 30 found that the presence of heart failure early in the disease process was not associated with higher mortality rates, whereas late heart failure was associated with poorer survival. Heart failure has been shown to be a prognostic factor in other studies10, 31
Effect of the patient age, as predictor of mortality (positively in surgically-treated but negatively in medically-treated patients), our results suggest that a factor that might be related with this better prognosis in surgically-treated is to operate on patients with active IE with an appropriate selection of older patients (≥60 years, 14 patients), recommended indications.
(Table 1): large vegetation, the most common indication (60%), streptococcus viridans IE (50%), less NYHA (classIV) (36%), only two patients (2/14) died from surgery (aortic valve ring abscesses).
Study Limitations
This analysis should be interpreted with regard to its retrospective nature in the early period, especially concerning the comparison between patients with and those without early surgery. However, because of the nature of the disease, controlled studies are not feasible.
Our study population was heterogenous, including in terms of native and prosthetic valve diseases, As it is typical in a tertiary hospital setting.
However, our findings are applicable to different populations only with caution. Firstly, because of the relatively low incidence of IE, patients were included over a relatively long period of time of 18 years, during which medical therapy and surgical methods improved considerably. This problem can not be overcome, since adequate numbers of patients can hardly be collected by one or two centres. Secondly, referral rates and access to surgery may differ between institutions.
Conclusion
The management of patients with IE, however, remains a challenge for physicians. Our findings may help to identify high-risk patients, need more aggressive treatment or interventions. A new finding was the hazard function for mortality being highest at enrollment and declining rapidly in both medically and surgically treated patients especially during the first 12 months after enrollment. Long term prognosis is good for survivors with active IE.
Footnotes
Acknowledgments
The authors thank the Department of Medicine and the Faculty for its support, the patients for their participation and Mr. Bryan Roderick Hamman for assistance with the English-language presentation.