
Abstract
Severe retrograde dissection extending into the sinus of Valsalva is a rare complication during percutaneous coronary intervention (PCI), but life threatening. There is some literature about this complication, but this particular complication has not been previously reported in China. We present a case of coronary artery dissection during a PCI in which progressively extended retrogradely into the sinus of valsalva, and was successfully treated with stenting without an operation.
Introduction
Severe retrograde dissection extending into the sinus of Valsalva is a rare complication during percutaneous coronary intervention (PCI), but life threatening. 1 The danger of this event depends on two aspects: first, the potential occlusion of the related coronary artery and second, the possibility of the dissection extending to the ascending aorta and further. There is some literature about this complication, but this particular complication has not been previously reported in China. We think that the rarity and unknown significance of this complication have probably led to a general underreporting in our country. We present a case of coronary artery dissection during a PCI in which progressively extended retrogradely into the sinus of valsalva, and was successfully treated with stenting without an operation. To the best of our knowledge, this is the first case reported in China.
Case Report
A 63-year-old man with severe unstable angina and aorta sclerosis, who had no primary hypertension and diabetes malleus, was admitted to our hospital to undergo a diagnostic coronary angiography. The procedure was performed from the radial approach and showed presence of three vessels with coronary artery disease (CAD) with severe stenosis of the proximal-mid left anterior descends (LAD) and of the proximal circumflex (CX) coronary arteries and with a chronic total occlusion of the proximal right coronary artery (RCA) (Fig. 1). He was already on treatment with aspirin, clopidogrel and anti-ischemia medicines. Immediately after the angiogram a percutaneous coronary intervention (PCI) of the RCA was planned. The RCA was easily cannulated with a soft tipped 6-French JR4 guiding catheter (USA) having a 0.064 inch inner diameter. After the selection of the guiding catheter in the RCA, an 0.014 inch Pilot 150 guidewire (USA) was advanced to cross the occlusion. After low pressure preinflation in mid segment, we found that a coronary artery dissection had developed at the distal stenotic lesion (Fig. 2) and the patient had stable conditions. The lesion and dissection in the distal RCA was successfully treated with a 3.0 × 24 mm EXCEL eleuting stent. After EXCEL eluting stenting (3.5 × 24 mm) of the lesion in the mid RCA, a contrast injection revealed spiral dissection of proximal RCA which retrogradely extended into the right sinus of Valsalva (Fig. 3). The Electrocardiogram did not show any sign of ischemia, and the patient had no discomfort. He was hemodynamically stable. A 4.0 × 24 mm EXCEL eluiting stent was then immediately placed in proximal overlap with the previous stent, and a second 4.0 × 12 mm EXCEL eluiting stent was deployed in proximal overlap in the RCA to obtain complete coverage of the ostium of RCA resulting in restoration of TIMI 3 flow. To optimize the result, a final post-dilatation was performed in RCA with a 4.0 × 12 mm stent balloon at 16 ATM. A control angiogram showed complete sealing of the coronary dissection and minimal contrast staining limited to the right sinus of Valsalva. Following successful PCI of the RCA, coronary angiography revealed TIMI III coronary blood flow and no dye retention in the right sinus of Valsalva in 30 minutes. Because of lack of chest pain and of signs of ischemia on the electrocardiogram and absence of further aortic involvement, the procedure was concluded and the patient was sent to the coronary care unit for further monitoring. With routine treatment including beta-blockade and low molecule weight heparin etc, the patient remained in the hospital for seven additional days and he was then discharged without any further event. A coronary artery angiography, performed three months later, showed complete resolve of right sinus of Valsalva dissection and no rest-enosis in RCA (Fig. 4). Meanwhile, we successfully performed PCI in another two vessels.
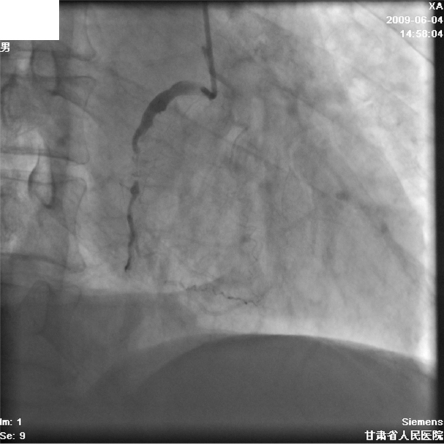
Coronary angiography of RCA. A chronic total occlusion of the proximal RCA.

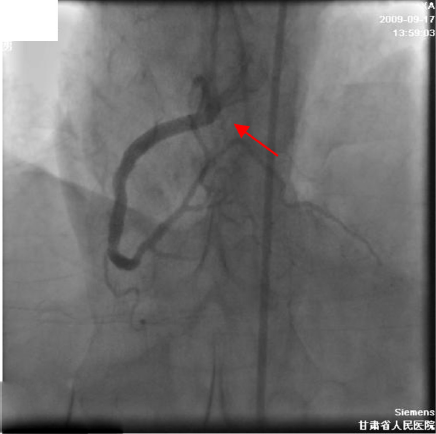
Dissection in mid-distal RCA (Red arrow). After preinflation in mid segment, a coronary artery dissection had developed at the distal stenotic lesion.

Dissection of the right sinus of Valsalva (Red arrow). Contrast staining limited to the right sinus of Valsalva.
Complete sealing of the sinus dissection (red arrow). Following successful PCI of the RCA, coronary angiography revealed TIMI III coronary blood flow and no dye retension in the right sinus of valsalva in 30 minutes.
Discussion
Retrograde dissection of the aorta is a rare but potentially life threatening complication of percutaneous coronary intervention. The incidence rate of this complication was 0%-0.008% for diagnostic catheterization and 0.15%-0.06% for angioplasty procedures from Yip HK et al and Perez-Castellano et al, respectively.1,2 Coronary artery dissection usually involves the RCA and the right sinus of Valsalva aneurysms is most common (75%-90%). 3 It is similarly found in iatrogenic aortic dissection during a coronary angiography or PCI. Most cases (63.4%) of reported iatrogenic aortic dissection to date have been related to the procedure in the RCA.1,2,4–11 But the exact mechanism of it is not clearly understood. A racial predominance is suggested by the finding that the incidence of sinus of Valsalva aneurysms is higher in far eastern countries than in western countries. 3
Iatrogenic aortic dissection may begin in the aortic root or coronary ostium. The causes of it may be direct damage from the catheter or guidewire, forceful dye injection or underlying medial degeneration. 1 The dissection of distal RCA arose after preinflation and this case had aorta sclerosis. Therefore, we think that the coronary artery dissection of the proximal-distal RCA lesion was caused by direct intimal injury from the guidewire and preinflation, and retrograde extensions of the dissection resulted from over-forceful dye injection and medial degeneration possibly. The etiology is most probably guide induced, rather than retrograde extension of dissection from the lesion against coronary flow. A Judkins right guide catheter from a right radial approach does not provide adequate support to tackle a CTO and as a result requires repeated manipulation/reintubation, likely causing an ostial RCA dissection that extends into the sinus, which is a major reason. Accordingly, these kinds of complications involve in many factors above.
Dissection of the RCA involving the right sinus of Valsalva is potentially a life-threatening condition; its management depends on patients’ condition, 5 progression of aortic dissection, and underlying coronary anatomy. While some authors maintain that the best option is outright surgical repair, some report a conservative strategy, with medical management only, while others think stenting of the entry port with bare or covered stents is suitable, if the patient is stable and the dissection is limited to the sinus of Valsalva. However, even when the initial clinical presentation is apparently benign, progression of the dissection into the ascending aorta can suddenly develop; not surprisingly, cases managed conservatively had a fatal outcome. In the case reported here, dissection of the RCA involving the sinus of Valsalva was succesfully treated by delivering a drug-eleuting stent up to the ostium of coronary vessel. Because of stability of the dissection, the absence of myocardial ischemia, and of disease which may predispose to dissection of the aortic arch (Marfan's syndrome, dilatation of the ascending aorta) we opted for percutaneous intervention and then medical management of the lesion. Of course, it is important to use adequate beta-blockade.
Aortic dissection limited to one sinus of Valsalva is a rare complication exclusively reported during catheterization interventions. However, we have not found any similar case with this singular and limited localization, and resolved by stenting in China.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material. Written consent was obtained from the patient or relative for publication of this study.