
Abstract
The U wave is still an electrocardiographic deflection of enigmatic origin. Numerous hypotheses on its origin have been formulated, but to date none has been conclusively proven. Recently, a report described the first case of bifid (or notched) U waves. Until then this phenomenon has only been described in the T wave. This is the first report of double U waves—two separate deflections, ascribed to an accessory papillary muscle.
Hypothesis
The presence of a double U wave will be associated with an accessory papillary muscle (s).
Materials and Methods
This is a retrospective analysis of 4729 patient files of patients who were evaluated at a cardiology practice. The 12-lead surface electrocardiogram was evaluated for the possible presence of a double U wave. In cases where a double U wave was found, the transthoracic echocardiogram was then scrutinized for the presence of an accessory papillary muscle.
Results
A total of 3 cases of a double U wave were found. In every case an accessory papillary muscle was clearly seen on the transthoracic echocardiogram.
Conclusion
A double U wave is a new variant of an old electrocardiographic deflection of enigmatic origin. This variant may be associated with an accessory papillary muscle.
Keywords
Introduction
The electrocardiographic deflection, which is sometimes seen at the end of ventricular repolarisation and which was named the U wave by Einthoven, is often seen in normal subjects, but is still of enigmatic origin.1,2 The electrophysiological basis of U wave generation is still elusive with numerous cited hypotheses,3,4 such as: repolarisation of the papillary muscles, 5 repolarisation of the Purkinje fibers outlasting that of the contracting myocardium, 6 prolonged repolarisation in cells of the mid-myocardium—the “M cells” 7 or it may be due to after-potentials, caused by mechanical forces in the ventricular wall with termination of mechanical systole—the “mechano-electrical feedback hypothesis”. 8
Equally interesting is the new focus on variation in morphology of the U wave: “Normal” U waves are usually upright, < 1 mm and of similar polarity of the preceding T wave. 4 Recently, Ariyarajah et al 4 described the first report of “notched” or “bifid” U waves—until this report only T wave bifidity have been described. But is it possible to observe two separate U waves—a true “double U wave”?
This study describes the first observation of double U waves—a new variant of a known electrocardiographic deflection of enigmatic origin, possibly associated with an accessory papillary muscle.
Materials and Methods
This is a retrospective analysis. A total of 4729 files of patients evaluated at a cardiology practice were evaluated for the presence of a double U wave, seen on a 12-lead surface electrocardiogram.
Case 1
A 46-year-old Caucasian male with no previous medical or surgical history presented for a routine medical evaluation to exclude any possible underlying disease.
He was completely asymptomatic and was not using any medical treatment.
The clinical examination did not reveal any abnormalities. The electrocardiogram (Fig. 1) demonstrated striking double U waves in leads II, III, aVF and V3–V6. An effort electrocardiogram (Bruce protocol via treadmill exercise) was within normal limits.

Electrocardiogram of case 1. Note the striking double U waves in leads II, III, aVF and V3–V6.
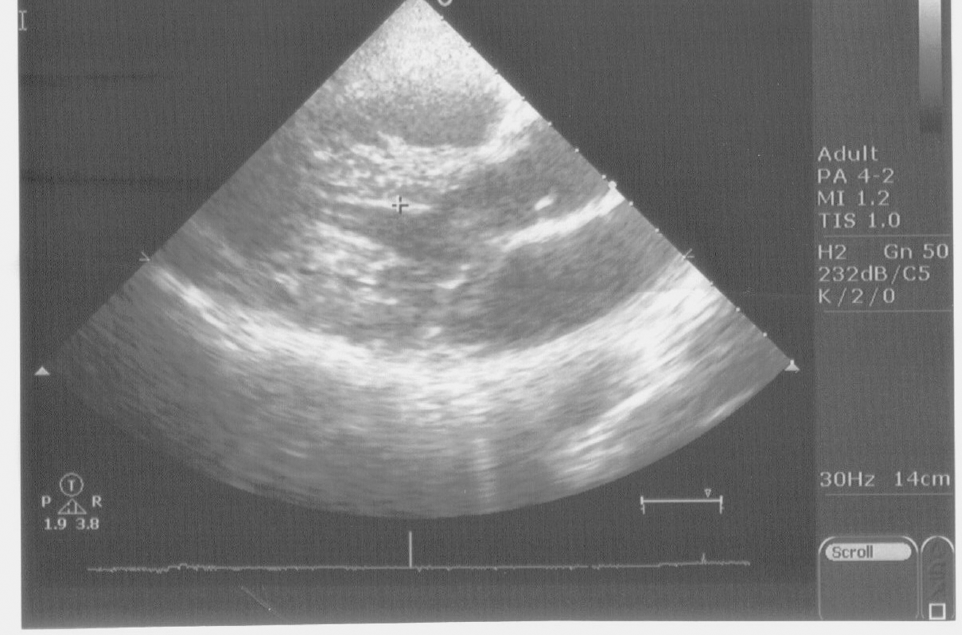
The echocardiogram demonstrated a structurally normal heart, but with a prominent accessory papillary muscle, situated between the left ventricular apex and interventricular septum (Figs. 2 and 3). No intra-ventricular pressure gradient or mitral valve dysfunction were present. Figure 2 is an echocardiographic image from the parasternal, long axis view, demonstrating the accessory papillary muscle (marked with +). Figure 3 is an echocardiographic image, taken from the apical, four-chamber view, also demonstrating the accessory papillary muscle, also marked with +. A comprehensive biochemical evaluation, which included thyroid function, serum glucose level, serum electrolytes, iron and ferritin levels and a full blood count did not reveal any abnormalities which could explain the double U wave.

Echocardiogram. Echocardiographic image demonstrating the accessory papillary muscle of case 1.

Echocardiogram. Additional echocardiographic image demonstrating the accessory papillary muscle of case 1.
Case 2
A 33-year-old Caucasian woman with no previous medical or surgical history also presented for a cardiovascular examination to exclude any possible underlying cardiovascular disease due to the presence of a family history of ischaemic heart disease. She was not taking any medicine and was completely asymptomatic. The clinical examination was completely normal and a biochemical screen did not reveal any abnormalities. The electrocardiogram (Fig. 4) revealed a double U wave in leads II, III, aVF and V3–V6. An effort electrocardiogram (Bruce protocol via treadmill exercise) was within normal limits. The transthoracic echocardiogram also revealed an accessory papillary muscle. No intra-ventricular pressure gradient or mitral valve dysfunction were present. Figure 5 is the parasternal, short-axis view—note the accessory papillary muscle marked with +. The accessory papillary muscle can be clearly seen, situated between the anterolateral and posteromedial papillary muscles. All serum electrolytes were within normal limits.

Electrocardiogram of case 2. Electrocardiogram demonstrating double U waves in leads II, III, aVF and V3–V6.

Echocardiogram. Parasternal, short-axis view of case 2. Note the accessory papillary muscle, marked with +.
Case 3
A 67-year-old Caucasian male with hyperlipidaemia presented for a cardiovascular examination. He was asymptomatic and was taking 10 mg of atorvastatin daily. His surgical history included a prostatectomy for benign prostatic hyperplasia.
The clinical examination was completely normal and a biochemical screen did not reveal any abnormalities. The electrocardiogram revealed a double U wave in leads II, III, aVF and V3–V6 (Fig. 6). An effort electrocardiogram (Bruce protocol via treadmill exercise) was within normal limits.

Electrocardiogram of case 3. Electrocardiogram demonstrating double U waves in leads II, III, aVF and V3–V6.
The echocardiogram demonstrated an accessory papillary muscle—Figure 7 is a parasternal, long-axis view, demonstrating the accessory papillary muscle just below the interventricular septum, marked with +. No intra-ventricular pressure gradient or mitral valve dysfunction were present. All serum electrolytes were within normal limits.
Echocardiogram. Parasternal, long-axis view of case 3, demonstrating the accessory papillary muscle just below the interventricular septum.
Discussion
This study clearly demonstrates the presence of double U waves. As these are visible on separate ECG leads (II, III, aVF and V3–V6) they are unlikely artefactual. Furthermore, as there is a clear return to baseline between these U waves, they cannot be considered bifid (or notched).
In all of these leads with a double U wave, a following P wave is clearly seen, thus the second U wave is also not a mistaken P wave. It is proposed that the second U wave is caused by the accessory papillary muscle.
Interestingly, this is not the first report linking U waves to papillary muscle anomalies. A case of ST segment elevation with QRS notching and a prominent U wave in lead V4 have been described in a patient with solitary papillary muscle hypertrophy 9 and another case linked an accessory papillary muscle to prominent U waves in the inferior leads. 3
In the era of readily available echocardiographic examinations, numerous other electrocardiographic phenomena have been explained by underlying endoventricular structural anomalies. These include: premature ventricular complexes with bigeminy due to a bifid papillary muscle, 10 inferior J-waves due to an accessory papillary muscle, 11 ST segment elevation due to a sub aortic tendon 12 and a new variant of right bundle branch block due to the presence of a sub aortic tendon, leading to an increased velocity of conduction in the left ventricle. 13 However, not all observed papillary muscle anomalies are associated with electrocardiographic changes—a case of a “mirror” papillary muscle had no electrocardiographic abnormalities. 14
It is proposed that the double U wave is a newly observed electrocardiographic entity, possibly and most probably caused by an accessory papillary muscle. Peculiarly, this is observed in leads II, III, aVF and V3–V6 in all of the observed cases. Whether or not there may be any associated arrhythmia risk is not known.
Disclosure
This manuscript has been read and approved by the author. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The author and peer reviewers of this paper report no conflicts of interest. The author confirms that they have permission to reproduce any copyrighted material. Written consent was obtained from the patients for publication of this study.