
Abstract
Epidemiological studies have reported associations between periodontitis and vascular disease in Europe. The aim of this multi-centric study was to evaluate the relationship between periodontitis and the calculated risk of cardiovascular death in the French adult population. The survey employed 2144 dentate adult subjects of the First National Periodontal and Systemic Examination Survey (NPASES I). This nationally representative sample was obtained by a quota method. The subjects had a complete full-mouth periodontal examination together with an evaluation of cardiovascular risk factors from laboratory tests, standard workup and questionnaires. Cardiovascular risk was calculated with the European SCORE scale calibrated for low risk populations. We found that age-independent cardiovascular risk increased with categories of periodontal disease (from 0.52 (health), 1.26 (slight), 1.69 (moderate) and 2.83 (severe). Cardiovascular mortality risk at 10 years (%), rose from 0.87 (health) to 1.83 (slight), 2.46 (moderate) and 3.94 (severe), p < 0.001. Our data show an association between periodontitis severity and the risk of cardiovascular death.
Introduction
Periodontitis are a group of infectious oral diseases resulting in inflammation within the supporting tissues of the teeth, which may lead to tooth exfoliation. Periodontitis affects a relatively high percentage of the adult population (Albandar et al. 2000; Albandar, Brunelle, and Kingman, 1999; Baelum et al. 2003; Baelum, Fejerskov, and Manji, 1988; Corbet, Wong, and Lin, 2001; Morris, Steele, and White, 2001; Papapanou, 1999). It is the most frequent cause of tooth extraction for people over 40 years of age (Reich and Hiller, 1993). Cardiovascular diseases remain the major cause of death and disability in developed countries, and become the major cause in emerging countries (Yusuf et al. 2001). Periodontal diseases have been associated with diabetes, adverse pregnancy outcomes, pulmonary disease, stroke and cardiovascular disease, but the causal relations have not been established (Pihlstrom, Michalowicz, and Johnson, 2005).
There is a large body of evidence that in addition to major cardiovascular risk factors, periodontitis is a risk marker for stroke (Dorfer et al. 2004; Scannapieco, Bush, and Paju, 2003) and ischemic heart disease (Howell et al. 2001b). Previous reports of the relationship between periodontal diseases and vascular disease have relied on cardiovascular events, and infrequently on the risk of death.
The National Periodontal and Systemic Examination Survey (NPASES I) was designed to estimate the prevalence, of periodontal diseases in the dentate adult French population, and to describe the associations between periodontal health status and various systemic conditions (Bourgeois, Bouchard, and Mattout, 2007). The NPASES I consisted of a full-mouth clinical periodontal examination, medical examination, laboratory tests, and interviews. In this report, we investigate the relationship between the calculated risk of cardiovascular mortality from integrated risk equations and the severity of periodontal disease, in a large middle age population.
Materials and Methods
The NPASES I is a cross-sectional survey representing the total civilian, non-institutionalized population, ranging from 35 to 65 years of age in France (Bourgeois, Doury, and Hescot, 1999). Details of this study have been published previously (Bouchard et al. 2006) and can be consulted on a website (http://lass.univ-lyon1.fr/pub/NPASES.pdf, 2005). Briefly, the NPASES I employed a multistage, stratified random sampling, stratified on age, gender, socioeconomic status, and geographic areas according the method of quota. Twenty-nine Health Centers were involved in this study. The total study sample included 2144 individuals available for the present analysis. Consenting subjects had 6 or more teeth. They were excluded from the study if they were diagnosed with patent cardiovascular disease, or having systemic anticoagulation or antiplatelet agents.
Cardiovascular Risk Assessment
The subjects underwent a systematic workup in which major risk factors were collected. Trained interviewers recorded medical status, life style and dental behavior data using standardized and validated questionnaires. Presence of Type 2 diabetes, history of hypertension, and presence of overt cardiovascular diseases (ischemic heart disease, lower limb ischemia, stroke) were recorded according to the WHO-ICD 10 codifications. Smoking status (current, former and never) was evaluated quantitatively as the number of cigarettes or equivalent per day. Alcohol consumption was evaluated qualitatively (every day, some days, rarely, former and never) and quantitatively in grams per day. Blood samples were drawn for usual biology, including dosage of fasting blood glucose, total and HDL cholesterol and liver markers. Height, weight were measured. Blood pressure was measured by a trained nurse, in triplicate, sitting position, using a random-zero sphygmomanometer. Hypertension was defined as systolic and diastolic blood pressure >140 or 90 mmHg, respectively, or current use of antihypertensive drugs. Diabetes was defined as the current use of antidiabetic drugs, fasting glycemia > 7.0 mmol/l, hypercholesterolemia was defined as current used of lipid lowering drugs or total CT >240 mg/dl.
Cardiovascular risk was integrated using the SCORE risk calculation, with parameters corresponding to low risk southern Europe population (Conroy et al. 2003). In order to better take into account the confounding effect of age, we further calculated a theoretical risk by using only age in the calculation of risk for each individual (i.e. the risk that the subject would have if he had the same age, but no additional cardiovascular risk factor). We then subtracted age-associated risk from the actual CV risk (taking age + other cardiovascular risk). This age-independent risk represents the aggregate risk attributable to CV risk factors.
Periodontal Examination
In each center, trained dental practitioners recorded the data on prepared record sheets. The intra and inter rater reliability between the examiners was evaluated according to the recommendation of the « Calibration of examiners for the international collaborative study of oral health outcomes » (WHO, 1994). The examiner consistency and reliability was previously published (Bouchard, Boutouyrie, Mattout, and Bourgeois, 2006). Briefly, intra- and inter-examiner variability for investigators by repeated measurements on individual sites in ten patients on CAL. The agreement at the end of the training phase calculated on the average of all pairwise comparisons between examiners for six-grade ordinal categories (2.3.4.5.7.9) was 0.75. Relative distances between successive ordinal categories were 1.
In the four quadrants, all fully erupted teeth were assessed, excluding third molars. The periodontal examination was carried out at four sites per tooth. The mesio-buccal, the mid-buccal, the disto-buccal and the palatal/lingual surfaces were assessed in millimeters for probing attachment level (PAL) and probing depth (PD) measurements. The assessments were made with a 0.20 N probing force by using a disposable PDT Sensor Probe type U.S. (Williams Chicago Illinois).
PAL was defined as the distance from the cemento-enamel junction to the tip of the probe. PD was defined as the distance from the soft tissues margin to the tip of the probe. The Plaque Index (Loe and SILNESS 1963) and Gingival Bleeding Index (Ainamo and Bay, 1975) were recorded at the same sites.
Each subject was assigned a diagnosis. The severity was characterized on the basis of clinical attachment loss (CAL) as follows: Slight = 1 or 2 mm CAL, Moderate = 3 or 5 mm CAL, and Severe = >5 mm CAL. CAL was defined as the apical migration of the periodontal attachment from a reference point, which was supposed to be the normality. We assume that, in an adult population the normality corresponds to CAL = 0.
Data Analysis
Statistical analyses and data management were performed using a statistical software program (NCSS 2004, Jerry Hintze, Kaysville Utah). Data were expressed as, proportions, means and standard deviations. Chi2 test was used to compare categorical variables. Analysis of variance was made for inter-group comparison, completed by Bonferroni all-pair comparison for post-hoc analysis. Logistic regression was used to characterize the relation between cardiovascular risk and peri-odontal disease as categorical parameters.
Results
Characteristics of the study population according to categories of periodontal disease are described in Table 1. Most components of cardiovascular risk increased with categories of periodontal disease (Table 2). Age increased with increased levels of periodontitis. Men were overrepresented in advanced periodontal states. Smoking, obesity, diabetes, hypertension were more frequent in patients with advanced periodontal disease severity. No difference was observed for dyslipidemia. Alcohol exhibited a U-shape relationship with periodontitis which is minimal in moderate drinkers and increased in abstinent and heavy drinkers.
Demographic parameters and cardiovascular risk factors, mean ± standard deviation, number (percentage).

Cardiovascular risk factors according to categories of periodontal disease.

NS means non statistically significant.
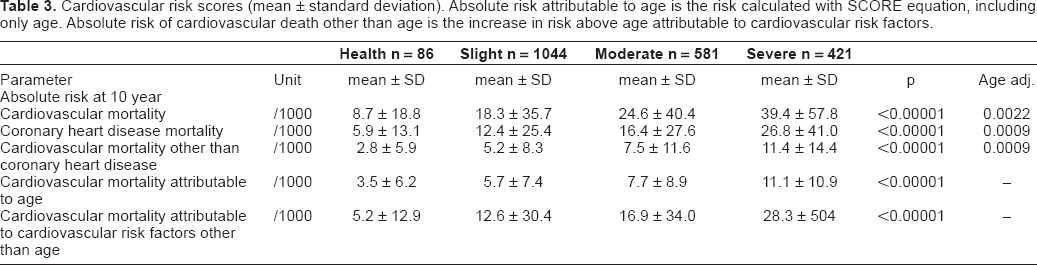
Cardiovascular risk of death, calculated with the SCORE risk scale, increased steeply among categories of periodontitis (Table 3). By comparison with the health category of periodontal disease, slight periodontitis was associated with a 2.1-fold increase in risk, moderate periodontitis with a 2.8-fold increase and severe periodontitis with more that 4-fold increase in risk of cardiovascular death. Periodontal disease was also closely associated with age-independent increase in risk (Table 3). Absolute age-independent CV risk rose with each category of periodontitis (2.4-fold for mild, 3.2-fold for moderate and 5.4-fold for severe periodontitis).
Cardiovascular risk scores (mean ± standard deviation). Absolute risk attributable to age is the risk calculated with SCORE equation, including only age. Absolute risk of cardiovascular death other than age is the increase in risk above age attributable to cardiovascular risk factors.
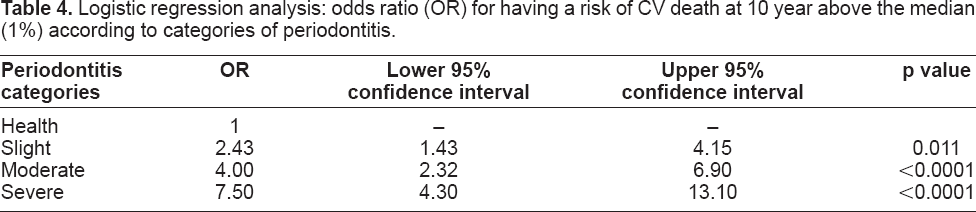
We further assessed the odd ratios for being above the median of risk for CV death at 10 year (median risk = 1%) in a logistic regression model (Table 4). We found OR of 2.4 [1.4 to 4.1] when periodontitis was slight, 4.0 [2.3 to 6.9] when periodontitis was moderate, and 7.5 [4.3 to 13.1], p < 0.0001 when periodontitis was severe. Results were nearly identical when age-independent absolute risk was taken instead of absolute risk of CV death.
Logistic regression analysis: odds ratio (OR) for having a risk of CV death at 10 year above the median (1%) according to categories of periodontitis.
Finally, we tested whether other components of periodontal disease, such as plaque index and gingival index contributed to the prediction of CV risk by constructing a multivariate, robust regression model relating the risk of CV death (Log transform), and periodontal disease parameters (attachment loss, plaque index, and gingival index). We found that all three components of periodontitis were significantly associated with the risk of CV death, explaining more than 8% of variance. This association was also highly significant when age-independent risk of CV death was used (data not shown).
Discussion
The main result of the present study is the presence of a close, age independent association between the severity of periodontitis and the CV risk factors, in a large sample of subjects that give us a representative picture of the periodontal status of a European country. These findings strengthen the hypothesis that periodontitis association with cardiovascular disease mortality is largely mediated through its relation with CV risk factors.
As expected, we found that CV risk was low, with a median value close to 1% for 10 year risk of CV death. We showed in this population that CV risk factors clustered with categories of periodontitis, with a significant association with each CV risk factors, (among them increasing age). When CV risks were combined in the SCORE equation, the relationship between periodontitis and risk of CV death at 10 year was reinforced, since it is well known that CV risk factors cluster together.
It has been suggested that the association between periodontitis and CV disease was age-dependent (Mattila, 2003). We eliminated the confounding influence of age on the relationship between periodontitis and risk of CV death by calculating an age-independent risk from the SCORE equation. We showed that after removing age-related CV risk, periodontal disease parameters were still significantly associated with CV risk, and contributed to explain about 8% of the variance of CV risk.
Periodontitis has been associated with certain systemic diseases including cardiovascular diseases (Slade et al. 2003). These diseases appear to share common risk factors such as increasing age, smoking, body fat content, socioeconomic status, stress, and health awareness. It remains discussed whether the statistical link between the two pathologies is only explained by common risk factors such as tobacco use, diabetes or male sex, or if there is a common pathway to both diseases (Hujoel, 2002; Katz et al. 2001; Larkin, 2001). Recent data suggest that periodontal diseases are also associated with elevated plasma levels of atherogenic lipoprotein (Rufail et al. 2007). In addition, an intervention study showed that peri-odontal treatment is associated with a lowering of the plasma cholesterol levels (Oz et al. 2007). Taken together, these arguments strengthen the association between periodontal diseases and atherosclerosis.
Inflammation is recognized as an early and strong component of atherosclerosis and markers of inflammation are predictive of cardiovascular events (Howell et al. 2001a). The pathogenic link between cardiovascular risk score and periodontitis may involve the deleterious role of cardiovascular risk factors on the periodontal disease progression, whereas the relation between cardiovascular events and periodontal disease involves chronic inflammation caused by periodontal infection, and perhaps extracellular matrix abnormalities explaining both dental and vascular changes. In our study, we found that white blood cell count was positively associated with periodontitis, which could represent a marker of the host reaction to chronic periodontal inflammation, which could be more important for cardiovascular risk than the presence of periodontitis per se (Beck et al. 2005). It has been shown that physical care and antibiotic treatments of severe periodontitis may also have positive effects on CV outcome (Seinost et al. 2005). Nevertheless, antibiotics alone (aimed at Chlamydia pneumoniae or Helicobacter pylori, germs uncommon in periodontitis) failed to favorably alter the course of ischemic heart disease (Andraws, Berger, and Brown, 2005). Several inflammatory diseases have been reported to be associated with severe periodontal disease such as Behcet disease (Akman et al. 2007; Celenligil-Nazliel, Kansu, and Ebersole, 1999). None of our subjects had identified active inflammatory disease at inclusion. Other factors such as gene polymorphisms and uncontrolled inflammatory responses to various stimuli by the overreacting genes might play a role in severe periodontitis together with cardiovascular disease (Hoge and Amar, 2006).
How do our results compare with clinical outcome data? A recent systematic review of the literature (Bahekar et al. 2007) in 5 prospective cohort studies indicated that persons with PD had a 1.14 times higher risk CHD events than controls (relative risk 1.14, 95% CI 1.07-1.21, p < 0.001), whereas the prevalence of CHD in the cross-sectional studies was significantly greater among individuals with PD than in those without PD (OR 1.59, 95% CI 1.33-1.91, p < 0.001). In the present study, we used calculated risk, integrating all identified cardiovascular risk factors as endpoint For comparing with the data of Bahekar, we ranked periodontal disease as present (moderate to severe PD), or absent (health or slight PD). This provided odd-ratios for being at high cardiovascular risk of 2.25 (95% CI 1.89-2.68), which is close to the odd ratios observed in cross-sectional studies. Although our study has not the same design, this suggests that most of the association between CHD and periodontitis may be related to its association with cardiovascular risk factors.
Identification of persons at high cardiovascular risk is difficult and often done too late for efficient primary prevention. Since the reasons to consult the dental surgeon are independent of any cardiovascular consideration, dental surgeons may help in this screening task. Therefore, showing a strong association between periodontitis and cardiovascular risk factors, before overt cardiovascular disease occurs, claims for its significant public health importance since it may help to propose changes in life style in patients with severe periodontitis.
Our study has several strengths: first it is based on a transversal cohort designed to be representative of the nationwide middle age unbiased European population. The method used for building this cohort is the in-situ quotas method, based upon a Baysian model, where each geographical and socio-professional category is represented in the same proportion as in the whole population. Therefore, no systematic bias has occurred in the selection of patients. Second, all patients followed the same workup assessing the severity and extent of periodontal disease by trained practitioners, and CV risk factors were collected using standardized questionnaires and standard method. Third, intra-oral measurements were based on a full-mouth examination, which may give the best epidemiological snapshot of the periodontal conditions.
However, the present study shares with others the limitations of its cross-sectional design. Thus, associations are suggested, and causation cannot be inferred from the outcomes. It does not inform on the relationship between periodontal disease and occurrence of clinical cardiovascular events.
The close association between periodontitis and CV risk score could be of public health importance, and the present survey supports the screening of subjects for primary prevention, involving the odontologists in prevention strategies. Taken together, our results encourage both, cardiologists to send their high risk patients to odontologists for controlling of periodontal conditions, and odontologists to give specific advices for life style changes and referral for cardiologic evaluation to their patients consulting for severe periodontitis. Further longitudinal studies are needed to evaluate the interest to screen for cardiovascular risk factors by dental surgeons.
Footnotes
Acknowledgments
This work is part of the NPASES I, which is funded by the French Union for Bucco-Dental Health (UFSBD), Paris, France, and the WHO Collaborating Center. The UFSBD supports several research projects, which shared data from the population-based NPASES I. This work was also partially supported by grants from Pierre Fabre, Castres, France. The authors wish to thank P. Hescot, president of UFSBD, J. Desfontaine and A.M. Farozzi, epidemiology coordinators of UFSBD, and N. Deville, general director of National Health Insurance Welfare, Saint Etienne, France.