
Abstract
Background
Aortic dilatation is associated with the presence of aortic diseases. Current guidelines for assessing the aortic root (AoR) depend on linear measurements acquired by two-dimensional (2D) echocardiography. We considered that real-time three-dimensional echocardiography, which correlates better with AoR volume obtained by computed tomography, is widely unavailable, and therefore, there is a need to determine the AoR volume using 2D echocardiography.
Methods
Fifty-one consecutive apparently healthy volunteers were recruited and subsequently divided into three age groups. Specified planes of acquisition and previously defined landmarks were identified, and phases of the cardiac cycle that allowed for measurement standardization were used. Volume was determined by the modified Simpson's method.
Results
Although the average diastolic and systolic volume measurements of the AoR dimensions were not significantly different across the three age groups in the study population, a highly significant difference was observed in the volume measurements between male and female normotensive persons, P < 0.01 in each case. AoR volume measurements were five times in the diseased compared with the normotensive individuals; however, linear measurements were only 1.5 times in size of the normal individuals. Both point and interval estimates of the volume measurements of AoR in adult normotensives in three age groups were presented as baseline information.
Conclusions
We hereby present a novel way to determine the AoR volume using 2D echocardiography and the normal reference range with respect to age and gender. We also established the relevance of our measurement by comparing the normal population with two isolated diseased aortas.
Background
Prediction of cardiovascular outcomes by noninvasive techniques remains a priority in patients with cardiovascular disease. Accurate and reproducible measurements of aortic root (AoR) dimensions are crucial for informed decision-making on the timing and nature of interventions on the aortic valve (AV) or AoR. Transthoracic echocardiography (TTE) can easily assess the AoR, and repeated measurements are safe and reliable.1,2 Some guidelines have suggested that specified measurement methods could be used to improve the reliability and validity of AoR measurement with TTE.3,4 Aortic dilatation is strongly associated with the presence and progression of aortic regurgitation, 5 and with the occurrence of aortic dissection. 6 Just as the left atrium (LA) volume (which reflects long-standing hemodynamic conditions) has been compared with the glycated hemoglobin of diabetes mellitus, 7 aortic dilatation assessed by volume determination (rather than linear dimensions) may also have similar quantitative strengths and may perhaps better predict outcomes in AoR diseases. When LA size is measured in clinical practice, volume determinations are preferred over linear dimensions because they allow accurate assessment of the asymmetric remodeling of the LA chamber. 8 In addition, the strength of the relationship between cardiovascular diseases is stronger for LA volume than for LA linear dimensions.9,10 Excellent correlation has been demonstrated between AoR volumes measured using real-time three-dimensional echocardiography (RT3DE) and multidetector computed tomography (CT). 11 However, RT3DE analyses are time consuming, and this modality has the tendency of underestimating the AoR volume. Since there is, however, no existing information on the expected normal range for AoR size assessed by volume determination using two-dimensional (2D) echocardiography, there is a need to investigate and create a reference range of values as baseline information among the healthy normotensive population.
Our attempt at quantification of the AoR size using 2D volume determination is therefore a logical consequence of the progress that has been made in the assessment of the dimensions of the LA and left ventricle (LV) using volume rather than linear measurements. We hypothesized that linear measurements may be an inaccurate surrogate for volume because the use is based on the unlikely assumption that asymmetric remodeling does not occur in the AoR, and therefore, there is a constant relation among AoR dimensions.
Objective
The objective of this study is to determine the AoR by volume by 2D echocardiography using specified planes of acquisition and previously defined landmarks for measurement and establish normal ranges and their variations with respect to gender and age. In addition, we further attempted to establish the relevance of the mean AoR volume obtained by comparing our results with that of two deceased patients with the established AoR disease.
Methods
Written informed consent was obtained from the participants. The research procedures were approved by the Osun State Health Research Ethics Committee, and the research was conducted in accordance with the principles of the Declaration of Helsinki.
Fifty-one consecutive adult volunteers underwent 2D echocardiogram in our Cardiology Unit. All studies were performed with a 3.5 MHz transducer and a Toshiba Nemio XG or a Siemens Acuson Cypress. The American Society of Echocardiography (ASE) recommends that in quantification of the AoR, 2D, parasternal long-axis images should be used to visualize the left ventricular outflow tract (LVOT) and the AoR should be recorded in different views in varying intercostal spaces and at different distances from the left sternal border. We propose that the AoR volume may be obtained using the modified Simpson's method by tracing from the hinge point of the right coronary cusp of the AV to the widest point of the corresponding sinus of Valsalva (SOV), and then to the corresponding sinotubular junction (STJ). The tracing should then be continued across the LVOT to the opposite STJ, to the neighboring SOV, and finally back to the hinge point of the noncoronary cusp of the AV. Due to movement of the AoR during the cardiac cycle, we found a midsystolic frame (beginning of the ST segment – Appendices 1-2) and end diastolic frame (peak of R wave – Appendices 3-4) most useful in demonstrating the landmarks for optimal tracing. By freeze-frame analysis, the systolic frame was scrolled to the widest excursion of the aortic leaflets, just before valve closure. The diastolic frame was scrolled to ensure valve closure, just before valve opening. These phases of the cardiac cycle allowed for standardization of measurements. We calculated the AoR volume using the modified Simpson's method (biplane method of disks). The average of each set of three measurements was taken. We thereafter compared the normotensive individuals in our cohort with the two isolated cases of known aortic disease.
Results
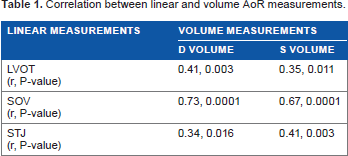
Of the 51 healthy normotensive volunteers, the male:female ratio was 1.4:1. The mean age was 41 ± 14 years. The subjects comprised three age groups, namely, 18-44, 45-64, and 65-79 years. The age range of the study population was 18-76 years. Normal AoR measurement (volume and linear) ranges and their variations with respect to gender and age were observed. The mean AoR volume was 6.84 ± 1.96 mL in diastole and 8.32 ± 2.20 mL in systole. We found that volume measurements significantly correlated with linear measurements (Table 1).
Correlation between linear and volume AoR measurements.
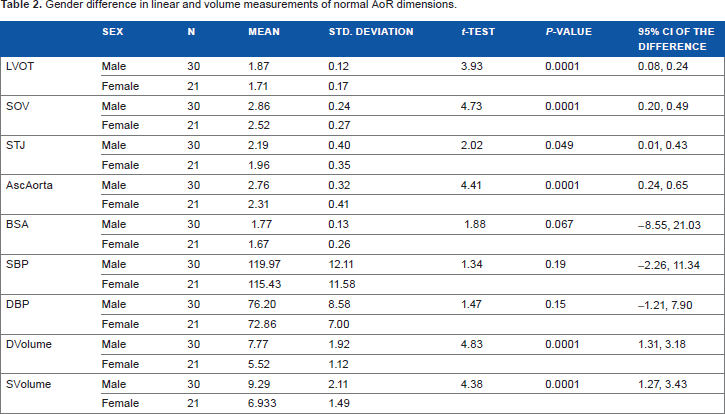
Both 18-44 years and 45-64 years age groups had comparable average diastolic (6.8 ± 2.1 vs 6.8 ± 1.1 and 7.8 ± 1.0; F = 0.343, P = 0.711) and systolic (8.2 ± 2.3 vs 8.3 ± 1.4 and 10.7 ± 0.6; F = 1.866, P = 0.166) volume measurements; however, a sharp increase was observed in the oldest age group, and there was no statistically significant difference in all the measurements though. These results were further presented in Figures 1 and 2. In AoR volumes, in Table 2, diastole and systole were typically found to be significantly larger in males than in females (7.8 ± 1.9 mL) vs (5.5 ± 1.1 mL) and (9.3 ± 2.1 mL) vs (6.9 ± 1.5 mL), respectively, P < 0.0001 in each case.

Diastolic Volume measurement of aortic root dimensions and age groups of normotensive individuals. Error bar showing mean and 95% confidence interval (CI) of AoR volume (Diastolic) by age groups with 43, 5 and 3 respective frequencies. No significant difference as (P > 0.05; F test).

Systolic Volume measurement of AoR dimensions and age groups of normotensive individuals. Error bar showing mean and 95% confidence interval (CI) of AoR volume (systolic) by age groups with 43, 5 and 3 respective frequencies. No significant difference as (P > 0.05; F test).
Gender difference in linear and volume measurements of normal AoR dimensions.
In Table 3, the mean AoR volume in diastole and systole for the normotensive individuals aged 65 years and above is 7.8 ± 1.0 mL and 10.7 ± 0.6 mL, respectively. Conversely, we found that the AoR volume of a 73-year-old hypertensive male who suffered aortic dissection was 38.6 mL, which is about five times larger compared with our mean volume in diastole. The corresponding LVOT and SOV measurements of the patient with the dissection were 3.1 and 4.8 cm, respectively (Appendices 5-6). The mean LVOT, SOV, and STJ measurements in our male sample aged 65 and above were 1.8 ± 0.1 cm, 3.0 ± 0.2 cm, and 2.5 ± 0.2 cm, respectively. We also compared our mean AoR volume with that of a 12-year-old boy diagnosed with Marfan's syndrome. He was found to have an appreciably larger AoR volume of 18.4 mL (Appendix 7). The corresponding LVOT, SOV, and STJ measurements for this boy were 1.9, 3.5, and 2.7 cm, respectively.
Average linear and volume measurements of AoR and age profile of normotensive individuals.

Discussion
RT3DE is a useful imaging modality that can be easily performed in the clinical practice and has been proven to be applicable in measuring the real volumes of cardiac chambers such as the LV,12–14 LA,15,16 and the right ventricle, 17 without geometric assumption. The volumes measured using RT3DE are well correlated with volumes assessed using other imaging tools such as cardiac magnetic resonance imaging (MRI) and multidetector CT. However, analysis of RT3DE is time consuming among other challenges of this modality 18 and may not be easily adaptable for routine clinical use. We found that it took less than three additional minutes to measure the AoR volume by tracing, as described earlier. Though the authors of previous studies did not present the time required for image analysis, 20-30 minutes would be necessary to analyze one image acquired by RT3DE.
We found that the AoR volume was larger in systole compared with diastole by about 2.0 mL. This is likely due to the deformations of the AoR during a cardiac cycle.19–22 These deformations allow for AoR expansion during isovolumic contraction. These deformations in the AoR may also explain our observation that visualization of the STJ was much more challenging at the end systole. Therefore, this emphasizes the need for the location and timing of measurements to be well defined, as outlined earlier for reproducibility of results.
AoR dimensions were typically found to be larger by about 2 mL in males than in females. Comparing those aged 18-44 years with those aged 45-64 years, volumes increased by 0.1 mL, and it increased by about 1-2 mL in 65-year olds or older. Our finding is in keeping with other studies conducted using cardiovascular MRI, which have found that the AoR dimensions are larger in males compared with females and that dimensions increase with age. 22
We made a brief attempt to establish the relevance of volume measurements by comparing this new variable with the established linear dimensions of two clearly diseased aortas. We found that the AoR volume of a 73-year-old male patient who died from aortic dissection is five times the mean of the normotensive male in the same age group. The corresponding linear dimensions were only about 1.5 times larger than the normal size. Furthermore, we found that the volume of the AoR of a 12-year-old boy suffering from Marfan's syndrome had doubled compared with our mean volume. This patient's linear dimension was just slightly above the adult normal reference values. The implication of the results of these comparisons is that volume measurements show remarkable deviations in AoR between the normal and the diseased individuals, whereas a linear measurement does not. This then suggests that a earlier prompt for intervention is more likely if deviations from the normal AoR dimension is based on volume measurements rather than the linear measurements, which could be less sensitive as was observed. Several studies have shown that a substantial number of complications occurred in patients with AoR dimensions less than that for which prophylactic root replacement is routinely performed.23–26 Until a molecular-based approach is widely available that will identify patients at high cardiovascular risk, echocardiographic variables will remain the most important prognostic indicators. 23
Therefore, we propose that assessing the AoR using volume measurements, rather than linear measurements, may better quantify the severity of dilatation, enhance earlier intervention, and possibly reduce morbidity and prevent mortality in patients suffering from AoR disease. This method of assessment, if adequately explored, may also have the potential of guiding therapy in AoR surgery.
Conclusion
To the best of our knowledge, our study is the first to describe AoR volume measurement and present the normal range by 2D echocardiography. Our finding has shown the importance of gender and age differences in AoR volumes.
This novel application can represent a reproducible new way to reliably determine AoR size and perhaps better quantify the degree of dilation in subjects with cardiovascular diseases with a view to predicting outcomes. We have shown an appreciable difference between the mean AoR volume of our subjects and the mean AoR volume of two diseased aortas.
This method of volume acquisition has the potential of removing the need to routinely perform RT3DE, which requires extensive training and acquisition time. We hope that our findings will stimulate further research in this area.
Author Contributions
Conceived the study and participated in its design and coordination and in drafting the initial manuscript: ATO. Participated in structuring the initial manuscript, presentation and critical review of the study, and performed data analysis: BEE. Critically reviewed the figures, tables, and overall data in addition to helping with the draft: AAA. Reviewed the subsequent drafts and made valuable input to the design: OOO. Participated in the manuscript drafting, editing, and review: EAA. Coordinated the overall process: MOB. All the authors read and approved the final manuscript.