
Abstract
We report two female patients with Takayasu's aortoarteritis, who presented with symptoms of cerebral ischemia due to critical stenosis of the sole patent cerebral artery. Both had occlusion of both vertebral arteries and one carotid artery with critical stenosis of the other carotid artery and presented with hemiparesis contralateral to the patent but stenosed cerebral artery. They also had transient ischemic attacks attributable to the culprit vessel. In the first patient, balloon angioplasty alone was not successful, and hence, a self-expanding stent was deployed in the right common carotid artery. In the second patient, successful balloon angioplasty was performed for the left common carotid artery. Distal protection devices were not used, and neither patient experienced any periprocedural neurological event. Clinical follow-up at six months revealed no significant cerebral events.
Introduction
Takayasu's aortoarteritis (TA) is a chronic inflammatory disease involving the aorta, arteries arising from the aorta, and frequently, the pulmonary arteries. The inflammation leads to stenosis/occlusion of the involved artery or aneurysm formation or both. The lesions of TA may demonstrate mural thickening and calcification, better seen on cross-sectional imaging such as computerized tomography (CT).1–5
The arterial lesions can lead to secondary hypertension, retinopathy, cardiac involvement, cerebrovascular events, and even premature death. The most catastrophic sequel is a cerebrovascular event. The sites of vascular involvement include the aortic arch and its branches, renal arteries, abdominal aorta, pulmonary arteries, and coronary arteries. 6 The most common site of involvement is the aortic arch and its branches. Involvement of all the branches of the aortic arch is uncommon and is associated with symptoms of severe cerebral ischemia. 7 The reporting of this procedure was approved by the institutional ethics committee.
Case Report
Case 1
A right handed female in her early 40s presented with right sided hemiparesis and motor aphasia. She continued to have repeated transient ischemic attacks (TIAs) in the same vascular territory. On examination, bilateral upper limb pulses were absent, with palpable lower limb pulses. There was a bruit on the right carotid artery, while there were no pulsations in the left carotid artery. She was normotensive and euglycemic with no atherosclerotic risk factors. The erythrocyte sedimentation rate (ESR) was 15 mm/hour. Magnetic resonance imaging (MRI) scan of the brain revealed a left middle cerebral artery infarct. Coronary angiography revealed 40%-50% ostial stenosis of the left main coronary artery, while the aortography revealed total occlusion of both subclavian arteries and the left common carotid artery. The right common carotid artery was patent but showed 80% long-segment stenosis in its proximal segment (Figs. 1 and 2). The abdominal aorta and renal arteries were angiographically normal.

Cannulation of the single patent aortic arch artery, namely the severely stenosed right carotid artery.

Aortic arch angiogram demonstrating the single patent severely stenosed carotid artery. The arrows point to the stenosed right brachiocephalic artery (White arrow), occluded left carotid (Black arrow) and occluded left subclavian arteries (interrupted arrow).
Intra-arterial heparin of 5000 U was administered to maintain an activated clotting time of >250 seconds. The stenosis in the right common carotid artery was crossed with a 0.014-inch 300-cm guide wire using a 6F JR 4 guide catheter and was predilated with 2.5 × 20 mm and 3.5 × 20 mm balloon catheters at 16 atm. The balloon inflations were brief (about 10 seconds) since this was the sole patent cerebral vessel. As there was no significant change in luminal diameter after balloon dilatation, a Precise® Pro RX® 8 × 40 mm nitinol self-expanding stent (Cordis, Johnson & Johnson) was deployed across the stenosis and postdilated with 6 × 20 mm balloon catheter. As the luminal diameter after stenting was suboptimal, it was postdilated at 16 atm using a 6 × 40 mm noncompliant balloon catheter (Fig. 3). The luminal diameter stenosis decreased from 80% to 40%. Since the patient complained of severe pain during balloon dilatation, further dilatation with larger diameter balloons was not performed, and it was decided to accept the residual stenosis of 40%. Since she had no symptoms suggestive of coronary ischemia, the coronary stenosis was not addressed.

Angiogram following stenting of the stenosed carotid artery segment using a self-expanding Precise 8 × 40 mm Nitinol stent (J&J) which was post-dilated using a 6 mm balloon. The arrows point to the proximal and distal ends of the stent in the carotid artery.
There were no procedure-related vascular or neurological complications. She improved clinically with cessation of the TIAs, and hospital stay was uneventful.
Case 2
A right handed female in her 20s presented with left-sided hemiparesis with repeated TIAs in the same vascular territory. She was normotensive and euglycemic with no atherosclerotic risk factors. On examination, bilateral upper limb pulses were absent. There were no bruits. Her ESR was 10 mm/hour. An MRI of the brain revealed a right middle cerebral artery infarct. She was subjected to an aortography, which revealed an occluded brachiocephalic artery with very faint filling of the right vertebral artery and right common carotid artery through small collaterals. The left subclavian artery was occluded at its ostium, and the sole patent branch of the aortic arch was the left common carotid artery, which showed a proximal 90% stenosis <10 mm in length (Fig. 4). Her abdominal aorta and renal arteries were angiographically normal.
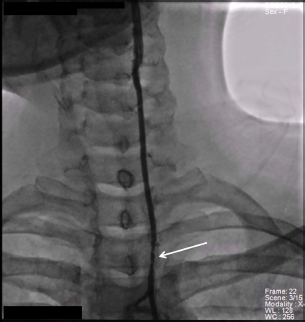
Cannulation of the severely stenosed carotid artery in Case 2.
A 7F Multipurpose Guide catheter was used to selectively cannulate the ostium of the left common carotid artery. Intra-arterial heparin 5000 U was administered to maintain an activated clotting time of >250 seconds. A coronary floppy-tipped 0.014-inch wire was used to cross the stenosis. The lesion was then serially dilated using 2.5 × 15 mm and 3.5 × 15 mm balloon catheters at 12 atm. The balloons were inflated for about 10 seconds. The luminal stenosis diameter decreased from 90% to less than 50%, with establishment of brisk distal flow (Fig. 5). Therefore, stenting was deferred, and a restudy was planned after three to six months. There were no procedure-related neurological or vascular complications. Neither patient had procedural or postprocedural hypotension or bradycardia as the lesions did not involve the carotid bulb. There was significant clinical improvement symptomatically, with cessation of the transient neurological deficits.

Angiogram following balloon angioplasty of the severely stenosed carotid artery using 2.5 × 15 mm and 3.5 × 15 mm balloon catheters.
In both patients, proximal or distal protection devices were not used, primarily due to financial considerations and also because the lesions in TA are usually fibrotic, firm, and nonulcerated. 8
Both patients were given aspirin 150 mg and clopidogrel 75 mg daily before the intervention, and this combination of antiplatelet regimen was recommended for six months followed by aspirin 150 mg/day daily.
As neither patient had signs of disease activity as evidenced by elevated ESR and C-reactive protein, they did not receive systemic corticosteroids or immunosuppressive therapies.
Follow-up
At 14-month follow-up, both patients were symptomatically better with cessation of TIAs and improvement in motor power in the upper and lower limbs with intensive physiotherapy. Repeat angiographic study was not performed in either patient. We also do not have any imaging follow-up studies (CT/MRI) due to logistic constraints.
Discussion
TA is a systemic disease of unknown origin, involving the aorta and its branches. The lesions are characterized by diffuse involvement requiring higher balloon pressures to dilate, with greater incidence of residual stenosis and a higher restenosis rate. 9
Angioplasty is the standard initial mode of treatment for aorta, renal, and subclavian artery stenosis caused by aortoarteritis.10–12 Its role in patients with a single patent arch artery presenting with severe cerebral ischemia is anecdotal. 7
The lesions in chronic TA, without disease activity are often multifocal, long segment, usually involving the ostium and producing irregularity, stenosis, or even total occlusion.1,2
Carotid artery involvement in TA is common (6%-69%), with the left side more commonly involved than the right. 3 Lupi-Herrera et al. 1 showed that 6.8% of these patients developed hemiplegia and 4.5% had loss of vision at a mean follow-up of 33.2 ± 37 months. Cerebrovascular events contribute to 20% of the of mortality in these patients.
Both our patients had advanced stages of TA, presenting to us with its major sequelae. Ours is a private teaching hospital and a tertiary referral center for patients in advanced stages of disease. Many of our patients present to our center only with late manifestations of the disease. Furthermore, both patients were from a lower socioeconomic background which may explain why they did not seek medical help during the early stages of the disease.
The therapeutic options for these patients include surgical carotid endarterectomy or percutaneous carotid angioplasty.7,9,10 Endarterectomy of a sole patent but stenosed carotid artery is associated with high rates of mortality and morbidity. 13 The one-year combined end point of all-cause mortality and major adverse events was 12.2% in the carotid stent group compared with 20.1% in the endarterectomy group. 13 Endarterectomy for TA is associated with high rates of morbidity, mortality, cranial nerve injury, anastomotic narrowing, graft occlusion, and aneurysm formation.1–3 Both our patients had stenosis of the arch vessels, close to their origins from the aorta. Surgical repair of such lesions often necessitates an intrathoracic approach, which would be more complex than a simple endarterectomy. In our clinical scenario of intervention for a single patent aortic arch artery with a severe stenosis, surgical repair was considered to have unacceptably high mortality and morbidity. 14 Hence, our first choice was angioplasty of the single patent but stenosed arch artery.
We did not attempt angioplasty of the occluded vessels since angioplasty of chronically occluded carotid arteries is associated with poorer outcomes due to lower initial success and higher restenosis rates. 8 In TA, higher balloon inflation pressures are often required for dilation as a result of transmural fibrosis. Shorter lesions are associated with good results, whereas the longer segment stenoses tend to have incomplete dilatation and higher rates of restenosis. A self-expandable nitinol stent was used in the first patient as the result of balloon angioplasty was suboptimal. Predilation of the lesion was done in a graded fashion, and following stenting, the stent was postdilated using a noncompliant balloon to reduce restenosis.
Cerebral protection devices may not be required in non-atherosclerotic fibrotic lesions such as fibromuscular dysplasia and TA because atheroembolization is unlikely. 9 Cutting balloon angioplasty may be beneficial in these fibrotic lesions, but financial constraints precluded the use of these devices. We reused angioplasty balloons and catheters (cleaned and resterilized) to keep the costs low. The safety and efficacy of reusing catheters has been documented earlier,15–17 and this is a common practice in many centers. The self-expanding stent was a free donated stent. In order to maintain adequate cerebral protection and prevent convulsions due to cerebral ischemia as other arch vessels were occluded, balloon inflation durations were maintained under 10 seconds.
In stenotic lesions of TA associated with neurological sequelae, angioplasty is a safer and more effective therapeutic option than medical therapy alone.7,9,10,18 This is especially so when disease activity is absent and in the presence of severe symptoms arising from its chronic vascular complications as seen in our patients.
Although the technique of carotid angioplasty presented here is not novel, our case series highlights the clinical fact that for patients with TA presenting with severe cerebral ischemia, and angiographic evidence of a single patent arch artery, revascularization of the single arch artery by angioplasty with or without stent placement is safe, effective, and a reasonable alternative to surgical therapy.
Author Contributions
Conceived and designed the experiments: KV. Analyzed the data: KV. Wrote the first draft of the manuscript: SMA. Contributed to the writing of the manuscript: KV. Agree with manuscript results and conclusions: KV, SMA. Jointly developed the structure and arguments for the paper: SMA. Made critical revisions and approved final version: KV. Both authors reviewed and approved of the final manuscript.