
Abstract
Context
Late intervention to open an occluded infarct-related artery (IRA) after initial acute myocardial infarction was postulated to lead to clinical benefit.
Objective
To conduct a meta-analysis of the randomized trials.
Study Selection
Eligibility criteria were: 1) randomized trials comparing percutaneous coronary intervention (PCI) in a totally occluded artery (TIMI flow 0-1) versus medical therapy, 2) in stable post myocardial infarction (MI) patients without spontaneous or low level exercise induced ischemia, 3) trials with a time from the onset of symptoms to randomization >24 hours, but <6 weeks, and 4) trials reporting mortality and recurrent MI as an endpoint. Of 961 citations reviewed, 3 disagreements were easily resolved by discussion and 6 trials were selected for inclusion.
Data Synthesis
The primary endpoint was the composite of recurrent MI or death. The secondary endpoints were the development of heart failure or recurrent myocardial infarction. In a meta-analysis of the 6 trials, which included 2642 patients, late intervention of an IRA had a RR of death or recurrent MI of 1.12 (95% CI 0.91-1.38). Data regarding the development of heart failure was available for 4 trials. In a meta-analysis of these 4 trials, which included 2527 patients, late intervention of an IRA had a RR of 0.79 (95% CI 0.58-1.08). Data regarding the occurrence of recurrent MI was available for 5 trials. In a meta-analysis of these 5 trials, which included 2598 patients, late intervention of an IRA had a RR of 1.28 (95% CI 0.91-1.79).
Conclusions
Our meta-analysis of the currently available randomized data addressing late intervention of an occluded IRA failed to reveal clinical benefit with regard to the clinical endpoints of death, heart failure or reinfarction. The trend towards an increase in reinfarction among the PCI treated patients suggested by the Open Artery Trial (OAT) investigators persisted, but did not achieve statistical significance.
Background
Early reperfusion after an acute myocardial infarction (MI) salvages myocardium, limits infarct size, preserves left ventricular (LV) function, and thus improves clinical outcomes (1). However, there are instances where restoring perfusion is not attempted or is not possible and the infarct related artery (IRA) remains occluded (2). Whether intervention on an occluded IRA days to weeks after initial MI leads to quantifiable clinical benefit has been debated (3).
The “open artery hypothesis” suggests that late reperfusion, beyond the time window for myocardial salvage, may improve prognosis independent of LV function (4,5). Mechanisms proposed to explain this purported benefit include prevention or attenuation of LV remodeling, (5,6) reduction of ischemia in border-zone myocardium, reduction of arrhythmogenic substrate, (7,8) and provision of collateral flow to other vessels (5).
A number of small prospective randomized trials have evaluated whether late opening of an IRA is clinically beneficial. These studies have revealed conflicting results (9-13). The definitive trial testing the open artery hypothesis, OAT (Occluded Artery Trial), was recently published. The OAT data refuted the open artery hypothesis, and in fact, revealed a trend towards harm in the form of an increased rate of reinfarction in the treatment arm (14). Thus, to obtain the most reliable estimates of the effect of late intervention in an IRA after acute MI on cardiac adverse events, we conducted a systematic review of the literature and meta-analysis of the randomized controlled trials addressing this question.
Methods
Literature Search
We searched for relevant trials in the following databases: MEDLINE (1966 to 2006), Cochrane Central Register of Controlled Trials (CENTRAL), and American College of Physicians (ACP) Journal Club. We used and combined the terms percutaneous coronary intervention, late intervention, myocardial infarction, percutaneous transluminal coronary angioplasty, open-artery, and infarct-related artery. We restricted our search to articles indexed as randomized trials (publication type), as well as those that mention the word random, placebo or trial in their text or abstract. We also hand-searched published abstracts presented at the meetings of the American Heart Association, American College of Cardiology, and European Society of Cardiology. We also reviewed the reference lists from recent reviews on the subject, and contacted experts in the field.
Trial Selection
Two authors (AZ, SJH) independently evaluated potential trials for inclusion. Citations considered relevant by one were further assessed in detail by both authors. Disagreements were solved by direct discussion. Eligibility criteria were: 1) randomized trials comparing percutaneous coronary intervention (PCI) in a totally occluded artery (TIMI flow 0-1) versus medical therapy, 2) in stable post CMC.S356myocardial infarction patients without spontaneous or low level exercise induced ischemia, 3) trials with a time from the onset of symptoms to randomization >24 hours, but <6 weeks, and 4) trials reporting mortality and recurrent MI as an endpoint.
Data Abstraction
Three of the authors (AZ, TBH, SJH) extracted data regarding demographic characteristics of the patients, use of medications, length of follow-up, ejection fraction, and the occurrence of recurrent MI, heart failure and death. If any information was missing from the published report, we contacted the primary authors requesting such information.
Statistical Analysis
The primary endpoint was the composite of death or recurrent MI. The secondary endpoints were the development of heart failure or recurrent MI. For all endpoints, the individual trial definition was used.
For each trial we calculated the relative risk and their corresponding 95% confidence interval (CI). In the meta-analysis we performed stratified analyses by trial to avoid direct comparisons between individual patients in the individual trials. We calculated the combined RR, and its 95% CI using the fixed effect model, as described by Mantel-Haezel (15). We attempted, but were unable to obtain all trial individual data.
The presence of heterogeneity was evaluated by means of the Q statistic, with a significance level of 0.05, and by visual analysis of a funnel plot. All analyses were conducted in the statistical software Revman version 4.2.8 (The Cochrane Collaboration).
Results
Literature Search
Of 961 possible relevant titles 921 were easily excluded on basis of the title. 40 abstracts were reviewed and 34 were excluded. The reasons for exclusion are depicted in Figure 1. There were only 3 disagreements which were easily solved by discussion. Using this strategy, 6 trials were finally included in the analyses (9-14).

Search strategy results. PCI: percutaneous coronary intervention; RCT: randomized controlled trials.
Patient Characteristics
The 6 trials randomized 2642 patients (1326 to PCI and 1316 to medical therapy). Table 1 describes the individual trial characteristics. The mean age of the randomized patients ranged from 57 to 62. Most randomized patients were males (70 to 86%). Time from MI to randomization varied from 25 hours to 27 days. The use of beta-blockers, aspirin, ACE-inhibitors and statins differed significantly across trials, a reflection in part of the long timeframe since the publication of the first (12) and the most recent trial (14). The length of follow-up varied from 4 to 34 months.
Characteristics of the trials included in the meta-analysis.

TAMI-6: Thrombolysis and Angioplasty in Myocardial Infarction - 6; TOAT: The Open Artery Trial; TOMIIS: Total Occlusion Post-Myocardial Infarction Intervention Study; DECOPI: Desobstruction Coronaire en Post-Infarctus; OAT: Open Artery Trial; n: sample size; MI: Myocardial Infarction; PCI: Percutaneous Coronary Intervention; ACEI: Angiotensin-Converting Enzyme Inhibitor; ASA: Aspirin; EF: Ejection Fraction; PTCA: Percutaneous Transluminal Coronary Angioplasty; BMS: Bare Metal Stent N/A: Not Available.
Data only available for entire cohort.
=Angiographic data from TOSCA-2, the angiographic substudy of 381 OAT patients (29).
Intervention
In 3 of the trials, balloon angioplasty was the intervention used among patients randomized to PCI (9,10,12) while in the three more recent trials, stents were used in the majority of patients (11,13,14). An angiographically successful PCI was obtained in 72 to 94% of the patients assigned to the intervention group.
An attempt at systematic angiographic follow-up was made in all patients for five studies (9-13), and in a prespecified subset of patients randomized in OAT, and published as the Total Occlusion Study of Canada (TOSCA)-2 Trial (29). The interval between initial and subsequent angiography ranged from 4 to 12 months. The rate of re-occlusion of an intervened artery ranged from 5% to 57%. In contrast, the rate of spontaneous recanalization for patients randomized to medical therapy ranged from 13% to 38%.
Outcome
Of the 6 trials, only 1 (n = 88 patients) found a statistically significant reduction in the primary outcome (10). We found no significant heterogeneity among the trial results (p = 0.15). Among the 2642 randomized patients, 313 had either a recurrent MI or died. Of these, 166 had been randomized to PCI and 147 to medical therapy. The pooled RR for death or recurrent MI was 1.12 for the angioplasty group (95% CI 0.91-1.38) when using the medical therapy group as reference. Figure 2 depicts the RR and corresponding 95% CI for the individual trials, as well as the pooled estimate.

Pooled data from the included trials. Late opening of a totally occluded artery had no effect on the combined outcome of death and recurrent myocardial infarction. TAMI-6: Thrombolysis and Angioplasty in Myocardial Infarction - 6; TOMIIS: Total Occlusion Post-Myocardial Infarction Intervention Study; TOAT: The Open Artery Trial; DECOPI: Desobstruction Coronaire en Post-Infarctus; OAT: Open Artery Trial.
Data regarding the development of heart failure were available for four of the trials (10,11,13,14). There was no heterogeneity among trials (p = 0.13). Of the 2527 patients enrolled in these trials, 147 patients developed heart failure. Of these, 65 patients had been randomized to PCI and 82 to medical therapy. The pooled RR for developing HF was 0.79 (95% CI 0.58-1.08) for the intervention group compared to the medical therapy alone group. Figure 3 depicts the Forest plot for this outcome.
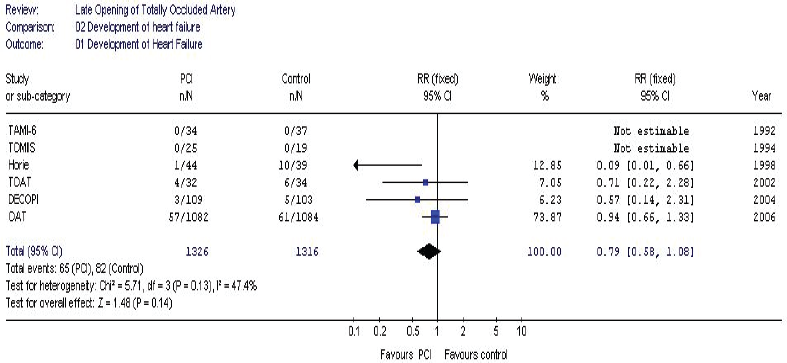
Pooled data from the included trials. Late opening of a totally occluded artery had no effect on the development of heart failure. TAMI-6: Thrombolysis and Angioplasty in Myocardial Infarction-6; TOMIIS: Total Occlusion Post-Myocardial Infarction Intervention Study; TOAT: The Open Artery Trial; DECOPI: Desobstruction Coronaire en Post-Infarctus; OAT: Open Artery Trial.
Data regarding the occurrence of myocardial infarction during follow-up were available for five of the trials (10-14). There was no heterogeneity among trials (p = 0.30). Of the 2598 patients enrolled in these trials, 128 sustained a myocardial infarction during follow-up. Of these, 72 had been randomized to PCI, and 56 to medical therapy. The pooled RR for developing a myocardial infarction was 1.28 (95% CI 0.91-1.79). Figure 4 depicts the Forest plot for this outcome. Table 2 shows endpoints for all included trials, as well as angio-graphic follow-up data.
Results of the trials included in the meta-analysis.

TAMI-6: Thrombolysis and Angioplasty in Myocardial Infarction-6; TOAT: The Open Artery Trial; TOMIIS: Total Occlusion Post-Myocardial Infarction Intervention Study; DECOPI: Desobstruction Coronaire en Post-Infarctus; OAT: Open Artery Trial; n: sample size; MI: Myocardial Infarction; PCI: Percutaneous Coronary Intervention; IRA: Infarct Related Artery; N/A: Not Available.
Among those randomized to PCI and whom had a follow-up angiogram.
Among those randomized to control group and whom had a follow-up angiogram.
=Angiographic data from TOSCA-2, the angiographic substudy of 381 OAT patients (29).
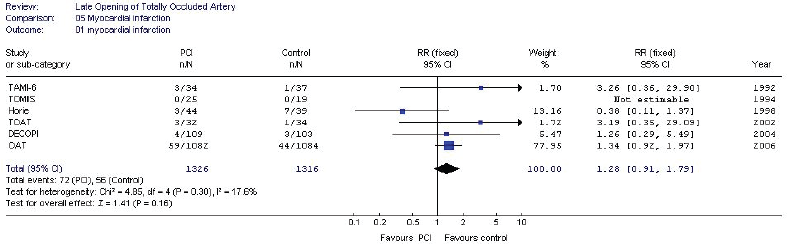
Pooled data from the included trials. Late opening of a totally occluded artery had no effect on recurrent myocardial infarction. TAMI-6: Thrombolysis and Angioplasty in Myocardial Infarction-6; TOMIIS: Total Occlusion Post-Myocardial Infarction Intervention Study; TOAT: The Open Artery Trial; DECOPI: Desobstruction Coronaire en Post-Infarctus; OAT: Open Artery Trial.
The funnel plot was symmetric (Figure 5), suggesting that publication bias should not have affected the observed results in a significant manner.

Funnel plot. Each of the blue circles represents individual studies. No publication bias is appreciated, small negative trials were included as much as positive ones.
Discussion
This meta-analysis of the 6 available randomized trials reveals no benefit or harm of late intervention on an occluded infarct related artery for either the combined endpoint of death and recurrent myocardial infarction, recurrent myocardial infarction alone, nor the development of heart failure.
It is generally agreed that, in patients, myocardial salvage can only be achieved within the first hours of acute myocardial infarction. The exact time window for such myocardial salvage may vary from individual to individual, due to variations in preconditioning and collateral circulation, but certainly does not exceed a few hours. The open artery hypothesis states that mechanisms other than myocardial salvage are responsible for the time-independent benefit of late reperfusion (5,16,17). Postulated mechanisms include prevention of LV remodeling, (5,6) reduction of ischemia in border-zone myocardium, reduction of arrhythmogenic substrate, (7,8) and provision of collateral flow to other vessels (5). Several observational studies have reported that patients with an open IRA had a lower mortality and incidence of congestive heart failure than those with an occluded IRA, independent of LV function (18-24). However, the largest retrospective analysis of 11,228 patients enrolled in the GUSTO I trial refuted these results, revealing that after adjusting for clinical and angiographic variables, a patent IRA was an independent predictor of death at 30 days, but not at 1 year (25).
This meta-analysis reveals no benefit of late intervention on an occluded infarct related artery for hard clinical endpoints. Only 1 trial showed a statistically significant benefit (10). Many of the randomized trials were underpowered to detect any possible benefit on clinical outcomes as they were unable to recruit their target number of patients, mainly because of strong clinical bias in favor of late opening of the IRA, and unwillingness of asymptomatic patients to consent for an intervention (26). The largest trial to date, OAT, failed to demonstrate any clinical benefit, and in fact revealed a trend towards increased myocardial infarction among the treated patients (14).
The benefit of late PCI observed on heart failure and suggestive benefit on recurrent MI or death are limited to the data reported by Horie (10). In this Japanese trial, the PCI used was balloon angioplasty, there was no use of glycoprotein IIb/IIIa inhibitors or thienopyridines, and the use of beta-blockers and ACE-inhibitors was suboptimal (Fig. 1). In contrast, the three more recent trials, TOAT, DECOPI and OAT revealed no significant benefit of late PCI on either the primary nor secondary endpoints (11,13,14). In these trials, a stent was implanted in more than 80% of the patients randomized to PCI, glycoprotein IIb/IIIa inhibitors and thienopyridines were widely used, and all the patients received aggressive medical therapy with beta-blockers, ACE-inhibitors, lipid lowering agents, and aspirin. These findings raise the question whether a late PCI of an occluded IRA might be beneficial only in the setting of suboptimal medical therapy.
The benefit of late PCI on reduction of LV remodeling observed in a number of the included trials (9-12) did not translate to a reduction in heart failure by meta-analysis. Maladaptive remodeling is associated with impaired prognosis in heart failure, and prevention of remodeling is an established therapeutic target. Horie and colleagues reported that increases among both end-diastolic and end-systolic volume index were significantly associated with adverse cardiac events (10). However, the evidence does not suggest benefit of late IRA intervention for the prevention of the clinical development of heart failure.
The trend of excess risk of reinfarction among PCI treated patients reported by the OAT investigators (14) did not reach statistical significance by our meta-analysis. However, there were relatively few events among the other 4 trials reporting this data (19% of total reinfarctions included in the meta-analysis). We await further analysis of the OAT data to clarify potential mechanisms for the trend towards increased reinfarction, such as loss of collateral flow or relation to dual anti-platelet therapy following stenting (27,28).
There are several limitations to this meta-analysis. First, there is a 14 year time span between the publication of the first and the last trial. Substantial progress has been made in improving outcomes both with medical therapy and PCI during this time period, and the results of the earlier trials might not be applicable in the present clinical arena. For example, in TOMIIS (1994), 68% of the entire post-MI cohort received beta blockers (9). Secondary prevention with statin usage was also not reported as the now firm evidence of benefit was only just emerging during the time frame of enrollment for the majority of the six included trials. Conversely, post-MI therapy in OAT (2006) included high rates of antiplatelet, beta blocker and ACE inhibitor use (14). Technical and adjunctive medical therapies among PCI patients in OAT, DECOPI and TOAT not available at the time of earlier trials include stents (bare metal and drug-eluting) and glycoprotein IIb/IIIa inhibitors. Second, we could not provide a reliable quantitative analysis of the changes in LV size or function as the techniques employed (echocardiography, angiography and nuclear contrast angiography) and timing of the measurement varied between the trials. Finally, the OAT trial included a substantially greater number of patients than all other trials, and therefore had the largest impact on the results in the meta-analysis.
Our meta-analysis of the currently available randomized data addressing late intervention of an occluded IRA fails to support any clinical benefit to the open-artery hypothesis. With no reduction in death, heart failure, and a potential increase in reinfarction, the available evidence does not support the role of late PCI among clinically stable post-MI patients with a totally occluded IRA as it is frequently being employed today. Unless contrary data from appropriately powered randomized trials becomes available, we believe any future policy recommendations should reflect these findings.