
Abstract
This study was designed to compare the effects of 12-month blood pressure (BP) control using cilnidipine and telmisartan on vascular damage in untreated hypertensive patients. One hundred patients were randomly assigned to either a cilnidipine group or a telmisartan group. The extent of vascular damage was assessed before and after treatment by measuring urinary albumin excretion (UAE), pulse wave velocity (PWV), and intima-media thickness (IMT) of the carotid arteries in each patient. Both drugs similarly decreased BP without altering plasma markers for oxidative stress or inflammation. Both UAE and PWV were significantly improved in both groups, but IMT was significantly reduced only in the cilnidipine group. Multiple regression analyses suggested that the UAE may have decreased as a result of a reduction in intraglomerular pressure caused by telmisartan or by efferent arteriolar dilation caused by cilnidipine. In addition, the PWV may have decreased as a result of the improvement in lipid metabolism caused by telmisartan or the reduction in plasma levels of aldosterone caused by cilnidipine. However, the analyses could not identify any definitive causal relationships or suggest the mechanism responsible for the improvement in IMT caused by cilnidipine. Thus, telmisartan and cilnidipine have unique properties for inhibiting vascular complications.
Keywords
Introduction
Recent studies comparing the long-term effects of calcium channel blockers (CCBs) and angiotensin II type 1 receptor blockers (ARBs) on hypertensive patients have demonstrated that both antihypertensive drugs have similar beneficial effects on lowering the risk of cardiovascular morbidity and mortality, (Julius et al. 2004) as predicted by a similar decrease in pulse wave velocity (PWV). (Ichihara et al. 2006a; Ichihara et al. 2006c; Ichihara et al. 2007) However, different mechanisms were thought to contribute to the benefits of CCBs and ARBs. Amlodipine, an L-type CCB, had a greater effect in reducing blood pressure (BP) (Julius et al. 2004) and its variability (Ichihara et al. 2006a) than ARBs such as valsartan and candesartan, and its pleiotropic effects on reducing oxidative stress and urinary albumin excretion (UAE) may make an important contribution to improving the cardiovascular benefits of valsartan and candesartan. (Ichihara et al. 2006a; Ichihara et al. 2006c)
A new generation of CCBs and ARBs was recently developed and has actually been prescribed for hypertensive patients. Cilnidipine is an N-type CCB that can inhibit sympathetic nerve activity and decrease intraglomerular pressure by dilating the efferent arterioles, (Hayashi et al. 2007) while telmisartan is an ARB that can bind to peroxisome proliferator-activated receptor-γ (PPAR-γ). (Benson et al. 2004) Recent studies demonstrated that reductions in UAE as a result of decreases in intraglomerular pressure were significantly associated with a reduction in the risk of micro- and macro-vascular events. (Olsen et al. 2006; Pontremoli et al. 2006) In addition, the PROactive study showed that the stimulation of PPAR-γ significantly decreased the secondary endpoint consisting of all-cause mortality, non-fatal myocardial infarction excluding silent myocardial infarction, and stroke. (Dormandy et al. 2005) Thus, prescription of the new CCB cilnidipine and the new ARB telmisartan may also have benefits for hypertensive patients.
The aim of this study was to compare the long-term effects of BP control using cilnidipine or telmisartan on markers for vascular complications in hypertensive patients who had never been treated with any antihypertensive drugs. The UAE was assessed as a surrogate marker, and PWV and intima-media thickness (IMT) of the carotid arteries were assessed as predictive markers for cardiovascular events.
Methods
Study Design
The subjects of the present study were 100 consecutive untreated hypertensive patients who attended the outpatient hypertension clinic of Keio University Medical School Hospital and for whom baseline arterial stiffness measurements by PWV were available. Patients with arrhythmias, previous cardiovascular events, or peripheral arterial disease were not included in the study. The 24-h ambulatory BP and three-times clinic BP were determined during a 3-month observation period before the start of the study. Clinic BP was measured in the right arm in the sitting position using a standard sphygmomanometer with appropriate sized cuff after the subjects were seated for at least 10 minutes. Hypertension was defined as a clinic systolic BP of > 140 mmHg at any time and/or a clinic diastolic BP of >90 mmHg at any time and as a 24-h ambulatory systolic BP of > 135 mm Hg and/or a 24-h ambulatory BP of >80 mmHg. No patients with any form of secondary hypertension, as diagnosed using classic laboratory and radiology tests, were included. All hypertensive patients were randomly assigned to a cilnidipine group or a telmisartan group, and life style modifications such as salt restriction, smoking cessation, and exercise were instructed to the patients throughout the study period. The cilnidipine group was started at a dose of 5 mg/day, and the dose was subsequently increased by 5-mg increments at intervals of 4 weeks. If the target BP of < 130/85 mmHg was not achieved at the maximum dose of 20 mg/day, a β-blocker was added; then, if necessary, a diuretic was also added. The telmisartan group was started at a dose of 20 mg/day, and the dose was subsequently increased in 20-mg increments at intervals of 4 weeks. If the target BP of < 130/85 mmHg was not achieved at the maximum dose of 80 mg/day, a diuretic was added; then, if necessary, a β-blocker was also added. Clinical and biological parameters were obtained before and 12 months after the start of medication with the anti-hypertensive drugs. The study was approved by the review board of Keio University Medical School Hospital, and written informed consent was obtained from every subject.
Venous blood samples were obtained in the morning after an overnight fast on the same days as the PWV measurements were made. Total cholesterol (TC), triglyceride (TG), and CRP concentrations were measured using the standard methods. Creatinine (Cr), uric acid (UA), total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), active renin concentrations (ARC), plasma aldosterone concentrations (PAC), and high-sensitive C-reactive protein (hsCRP) in venous blood samples were measured using standard methods and commercially available kits. Oxidized LDL-C was analyzed by assaying malondialdehyde LDL-C (MDA-LDL) using an enzyme-linked CMC.S353immune-sorbent assay (SRL Inc., Tokyo, Japan). Plasma 8-isoprostane levels were determined using a stable-isotope-dilution mass-spectrometric assay. (Morrow et al. 1995)
Ambulatory Blood Pressure Monitoring
Twenty-four-hour ambulatory BP monitoring was performed using an oscillometric-based device (TM-2431; A&D Co., Tokyo, Japan), as described in a previous study (Ichihara et al. 2006b; Ichihara et al. 2006a; Ichihara et al. 2006c; Ichihara et al. 2007) Briefly, BP was measured every 30 min during the daytime period (between 6:00 AM and 10:00 PM) and every 60 min during the nighttime period (between 10:00 PM and 6:00 AM). The mean values and standard deviations of ambulatory BP for each subject were calculated for 24 h and separately for the daytime and nighttime periods. The standard deviation of the ambulatory BP values was recorded as the variability of ambulatory BP in this study. The nocturnal decrease in BP was calculated as the average systolic BP during the daytime period minus the average systolic BP during the nighttime period. The morning BP surge was calculated as the average systolic BP during the first 2 h after waking minus the lowest systolic BP during the nighttime period. The ambulatory monitoring was repeated on the same day of the week, and the physical activity on the day of ambulatory monitoring was assessed in each patient.
Pulse Wave Velocity
Clinic BP and PWV were determined using a pulse pressure analyzer (model: BP-203RPE; Nihon Colin, Tokyo, Japan) using a previously described method. (Ichihara et al. 2002; Ichihara et al. 2003; Ichihara et al. 2005a; Ichihara et al. 2005b; Ichihara et al. 2006b; Ichihara et al. 2006a; Ichihara et al. 2006c; Ichihara et al. 2007) Briefly, the pulse volume waveforms were recorded using plethymographic sensors placed over the right brachial artery and both posterior tibial arteries. The PWV values measured using this method are significantly correlated with carotid-femoral PWV, (Sun et al. 2002) the heart-ankle PWV, (Ichihara et al. 2005a) and the aortic PWV measured by the catheter method, (Yamashina et al. 2002) with high correlation coefficients of 0.81, 0.89, and 0.87, respectively. The best ten consecutive pulses were analyzed in the present study, and the average PWV was recorded. The PWV was measured when the patients' heart rate was stable at 60 to 80 beats/min after at least a 5-min rest. Two measurements were performed in each leg, and the average values were used in the analysis. Values are expressed in units of cm/s.
Carotid intima-media thickness
Ultrasonography B-mode imaging of the carotid artery was performed with a PowerVision 6000 machine (Toshiba, Tokyo, Japan) at a transducer frequency of 7.5 MHz. Each subject was examined in the supine position. Up to 4 cm of the common carotid artery and the carotid bulb were scanned bilaterally in the longitudinal and transverse projections. The image was focused on the far wall of the artery. The intima-media thickness (IMT) was defined as the distance between the leading edge of the lumen-intima interface and the leading edge of the media-adventitia interface of the far wall, and the greatest IMT value in the bilateral longitudinal projections was recorded as the maximum IMT. All measurements were performed under blind conditions. The mean intraobserver and interobserver coefficients of variation for the maximum IMT were 4.3% and 4.7%, respectively.
Urinary Albumin Excretion
Urinary albumin excretion (UAE) was evaluated on the basis of the mean albumin-to-creatinine ratio in three nonconsecutive overnight urine samples collected one week before ambulatory BP monitoring was started. The urinary concentrations of albumin and creatinine were determined using a turbidimetric immunoassay with a Superior-Microalbumin kit (DPC Co., Tokyo, Japan) and using the Jaffe reaction with an autoanalyzer. The detection limit and coefficient variation of UAE was 0.4 mg/gCre and 10%, respectively.
Statistical Analyses
Sample size was calculated using SAS Institute JMP version 6.0 with SD of mean decrease (between-group variance) for parallel design assuming a power of 0.80 (α = 0.05). We calculated that 40 subjects would provide 80% power for detecting both an absolute decrease of 12 mg/ gCre in UAE and 200 cm/s in PWV during 1-year treatment with antihypertensive drugs with α = 0.05 based on our previous studies.(Ichihara et al. 2003, Ichihara et al. 2006a; Ichihara et al. 2006c; Ichihara et al. 2007) Because the distribution of hsCRP and UAE was highly skewed, the natural logarithm of hsCRP and UAE was used for statistical analyses. Analyses were performed with StatView 5.0. software (SAS Institute Inc., Cary, NC). The Fisher exact test was used to analyze gender and the frequency of the patients' characteristics, except for age and body mass index which were analyzed using the Mann-Whitney
Results
Patient Characteristics
The clinic BP and the 24-h ambulatory BP of the 100 patients in the present study averaged 154/98 and 149/94 mmHg, respectively; thus, the patients had mild hypertension, defined as a clinic systolic BP of <160 mmHg and a clinic diastolic BP of <100 mmHg. The average doses of cilnidipine and telmisartan that the patients were taking at the end of the observation period were 14 ± 2 and 50 ± 5 mg/day, respectively. A diuretic was additionally prescribed for 4 patients in the cilnidipine group and for 6 patients in the telmisartan group; the proportions of patients who received a diuretic were similar in both groups. A β-blocker was additionally prescribed for 3 patients in each group. In both groups, any cardiovascular events did not occur during the 12-month study period.
Table 1 shows no significant differences in the baseline values of the patients in the cilnidipine and telmisartan groups, and no significant changes were observed in either group during the 12-month observation period except for the serum levels of TC and LDL-C, the plasma ARC, and the PAC. In the telmisartan group, as shown in Figure 1, the serum levels of TC and LDL-C significantly decreased from 216 ± 9 to 201 ± 7 mg/dL and from 128 ± 8 to 115 ± 5 mg/dL, respectively, during the 12-month treatment period, although they did not change in the cilnidipine group during the 12-month treatment period. Plasma ARC significantly increased from 8.6 ± 1.2 to 36.1 ± 11.8 pg/mL in the telmisartan group, but the plasma ARC of the cilnidipine group did not change during the 12-month treatment period. Of interest, PAC significantly decreased during the 12-month treatment period in both the cilnidipine group and the telmisartan group, from 136 ± 12 to 117 ± 11 and from 126 ± 11 to 109 ± 9 pg/mL, respectively.
Patient characteristics at baseline.

Data are the means ± SD.
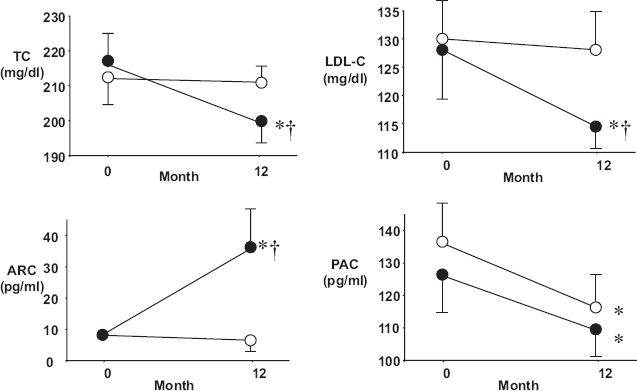
Serum levels of total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C) and plasma concentrations of active renin (ARC) and aldosterone (PAC) at baseline and after 12 months of treatment in the cilnidipine group (open circles, n = 50) and telmisartan group (closed circles, n = 50). *
The serum levels of hsCRP, MDA-LDL, and 8-isoprostane were similar at baseline in both the cilnidipine and telmisartan groups and remained unchanged during the 12-month treatment period. The hsCRP at baseline and after treatment averaged 595 ± 152 and 587 ± 204 ng/mL, respectively, in the cilnidipine group and 608 ± 207 and 593 ± 251 ng/mL, respectively, in the telmisartan group. The MDA-LDL at baseline and after treatment averaged 111 ± 22 and 108 ± 15 U/L, respectively, in the cilnidipine group and 106 ± 15 and 102 ± 15 U/L, respectively, in the telmisartan group. The 8-isoprostane at baseline and after treatment averaged 12.3 ± 1.4 and 12.3 ± 1.5 pg/mL, respectively, in the cilnidipine group and 12.3 ± 1.4 and 12.8 ± 1.0 pg/mL, respectively, in the telmisartan group.
Clinic and ambulatory BP
Table 2 shows the changes between the clinic BP, the 24-h, daytime and nighttime ambulatory BPs, and the heart rate (HR) in the cilnidipine and telmisartan groups at baseline and after 12 months of treatment. The clinic systolic/diastolic BP and 24-h, daytime and nighttime ambulatory systolic/ diastolic BPs significantly decreased during the 12-month treatment period in both the cilnidipine and telmisartan groups, and the decreases in BP were similar in both groups. HR significantly decreased in the cilnidipine group but remained unchanged in the telmisartan group, although the decrease in HR in the cilnidipine group was not statistically significant compared with the change in the telmisartan group. The BP variability assessed on the basis of the standard deviation of ambulatory systolic BP did not change in either the cilnidipine group or the telmisartan group. The 12-month treatment with cilnidipine or telmisartan did not affect either the nocturnal BP decrease or the morning surge.
Blood pressure before and after treatment.

Data are the means ± SD.
P < 0.05 versus baseline.
Target-organ damage
The baseline UAE values in the cilnidipine and telmisartan groups averaged 26.5 ± 7.7 and 34.8 ± 9.4 mg/gCr, respectively (n = 50 in each); these values significantly decreased to 14.0 ± 2.9 mg/gCr in the cilnidipine group and 11.1 ± 3.8 mg/gCr in the telmisartan group after the 12-month treatment, as shown in Figure 2. To the exclusion of six patients in the cilnidipine group and seven patients in the telmisartan group whose UAE was undetectable at the start of the study, the baseline UAE values in the cilnidipine and telmisartan groups averaged 29.1 ± 6.6 (n = 44) and 37.4 ± 7.7 mg/gCr (n = 43), respectively; these values significantly decreased to 15.3 ± 2.4 mg/gCr in the cilnidipine group and 11.9 ± 3.4 mg/gCr in the telmisartan group after the 12-month treatment. In either case, the magnitude of the decrease in the UAE was similar in both groups. The baseline PWV values in the cilnidipine and telmisartan groups were similar, averaging 1651 ± 72 and 1666 ± 51 cm/s, respectively. The PWV significantly decreased to 1489 ± 53 cm/s in the cilnidipine group and to 1476 ± 46 cm/s in the telmisartan group; the decreases in PWV were similar in both groups. In addition, the 12-month treatment with cilnidipine significantly decreased the maximum IMT of the carotid arteries from 1.06 ± 0.12 to 0.88 ± 0.05 mm, whereas the 12-month treatment with telmisartan did not alter it. In the telmisartan group, the maximum IMT at baseline and after the 12-month treatment averaged 1.00 ± 0.12 and 0.94 ± 0.09 mm, respectively.

Urinary albumin excretion (UAE), pulse wave velocity (PWV), and maximum intima-media thickness (IMT) of the carotid arteries at baseline and after 12 months of treatment in the cilnidipine group (open circles and bars, n = 50) and telmisartan group (closed circles and bars, n = 50). *
Multiple Regression Analysis
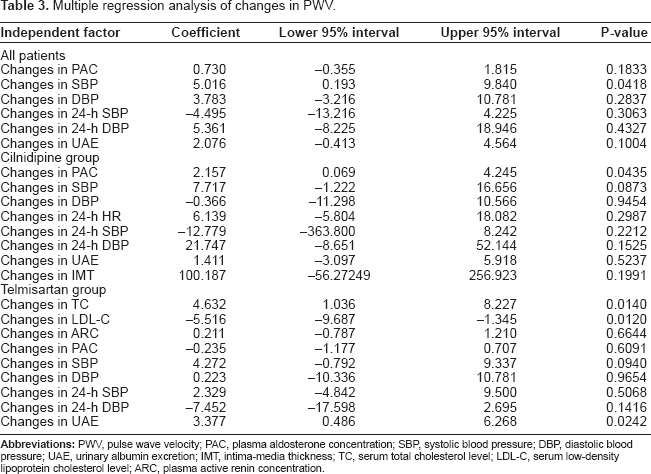
The changes in PWV were significantly associated with the changes in PAC in the cilnidipine group, the changes in TC, LDL-C, and UAE in the telmisartan group, and the changes in clinic systolic BP in all the patients treated with either cilnidipine or telmisartan (Table 3). The changes in UAE were significantly associated with the changes in PAC, 24-h diastolic BP, or PWV in the telmisartan group and the changes in PAC and 24-h diastolic BP in all the patients treated with either cilnidipine or telmisartan (Table 4). The changes in the maximum IMT observed in the cilnidipine group were not associated with any significant changes in parameters (Table 5).
Multiple regression analysis of changes in PWV.
Multiple regression analysis of changes in UAE.

Multiple regression analysis of changes in IMT in cilnidipine group.

Discussion
UAE is a surrogate marker, and PWV and IMT are predictive markers for cardiovascular events. Olsen et al. 2006; Pontremoli et al. 2006; London and Cohn, 2002; Tsivgoulis et al. 2006) Although significant correlations among these three markers have been reported, UAE and PWV can also predict micro- and macro-vascular complications, respectively, (Ruggenenti et al. 2004; Blacher et al. 1999) and IMT is known to be significantly associated with a high risk of stroke. (Tsivgoulis et al. 2006) In the present study, both cilnidipine and telmisartan similarly decreased clinic and ambulatory BPs and significantly improved both UAE and PWV, but IMT was significantly reduced only in the cilnidipine group.
Multiple regression analyses suggested that decreases in 24-h DBP, PWV, and PAC were significantly involved in the decrease in UAE in the telmisartan group. Previous studies demonstrated a significant association between decreases in UAE and decreases in BP and PWV (Ichihara et al. 2006a; Ichihara et al. 2006c; Ichihara et al. 2007) and reported that aldosterone blockade elicits a reduction in UAE through anti-inflammatory and anti-fibrotic effects on the kidneys. (Blasi et al. 2003) Although regression analyses do not provide any definitive causal relationships, telmisartan might decrease UAE by reducing BP, PWV, and PAC. However, decreases in 24-h DBP, PWV, and PAC were also observed in the cilnidipine group but did not significantly contribute to the decrease in UAE. Therefore, the mechanism accounting for the decreases in 24-h DBP, PWV, and PAC as a result of telmisartan, but not as a result of cilnidipine, may directly contribute to the decrease in UAE. ARBs lower BP, PWV, and PAC by inhibiting angiotensin II effects via a mechanism that is distinct from that of calcium channel blockers. The blockade of angiotensin II effects is well known to dilate efferent arterioles and thus to lower intra-glomerular capillary pressure. Thus, the UAE reduction in the telmisartan group might be caused by a reduction in the intraglomerular pressure as a result of angiotensin II antagonism.
In the cilnidipine group, none of the variables that changed significantly during the treatment period contributed to the decrease in UAE. Cilnidipine, an N-type CCB, (Uneyama et al. 1999) has an inhibitory effect on cardiovascular sympathetic neurotransmission (Sakata et al. 1999) and is reported to be able to reduce intraglomerular capillary pressure by dilating the efferent arterioles, suggesting a predominant presence of N-type calcium channels in efferent arterioles. (Hayashi et al. 2007) In the present study, the average HR for 24 h significantly decreased in the cilnidipine group, but the decrease in the HR did not statistically contribute to the UAE reduction. Thus, a reduction in the intraglomerular capillary pressure might also play a role in decreasing the UAE in the cilnidipine group. However, since the BP reduction plays an important role in the UAE reduction during anti-hypertensive treatment, (Casa et al. 2005) the UAE reduction observed in both groups might be directly due to the BP lowering.
Both telmisartan and cilnidipine significantly decreased PWV, which can be used to predict cardiovascular events in hypertensive patients. (London and Cohn, 2002) In the present study, multiple regression analyses suggested that both the decreases in TC and LDL-C in the telmisartan group and the decreases in PAC in the cilnidipine group may significantly contribute to the decrease in PWV. Among ARBs, telmisartan is the most powerful agonist of PPAR-γ in mouse adipocytes (Schupp et al. 2004) and exhibits properties that decrease the adipocyte cell size, reduce hepatic fat storage, and increase energy expenditure in hyperlipidemic rats fed a high-fat, high-carbohydrate diet. In addition, telmisartan significantly decreased plasma TC and LDL-C without altering the BMI or glucose metabolism in a manner that was independent of its BP-lowering effect in patients with type 2 diabetes mellitus. (Derosa et al. 2004) These results let us suppose that telmisartan might inhibit arterial stiffness through its potential effects on adipose tissue biology. However, another ARB, valsartan, which have no effect on adipose tissue biology, (Sugimoto et al. 2006) similarly decreased PWV. (Ichihara et al. 2006a) Further studies will be required to determine the contribution of a PPAR-γ agonistic property of telmisartan to the improvement of arterial stiffness.
Both telmisartan and cilnidipine significantly decreased PAC and PWV. Nevertheless, only the cilnidipine-induced reduction in PAC significantly contributed to a decrease in the PWV. These results suggest that the mechanism accounting for the decreases in PAC induced by cilnidipine, but not by telmisartan, may directly contribute to the decrease in PWV. CCBs decrease PAC by decreasing the intracellular concentration of calcium, which plays an important role in the regulation of human aldosterone synthase CYP11B2 expression. (Clyne et al. 1996) Thus, this calcium channel-blocking property may contribute to the decrease in PWV. Studies have reported that CCBs have antiinflammatory and anti-oxidative effects leading to the regression of atherosclerosis independently of their effect on lowering BP. (Cominacini et al. 1999; Yoshii et al. 2006; Ichihara et al. 2006a; Ichihara et al. 2007) Although no changes in hsCRP, MDA-LDL, or 8-isoprostane were noted during the treatment period, endothelial function and adhesive molecules at the tissue level, which were not analyzed in the present study, might be influenced by cilnidipine.
The 12-month monotherapy with a CCB did not improve the IMT, (Ichihara et al. 2006a) although CCBs combined with ARBs occasionally exert a slight but significant decrease in IMT. (Ichihara et al. 2006c; Ichihara et al. 2007) In the present study, however, the 12-month monotherapy with cilnidipine significantly decreased the IMT. Multiple regression analyses did not find any significant variables contributing to the decrease in IMT in the cilnidipine group. Anti-sympathetic, anti-inflammatory, and anti-oxidant effects of cilnidipine that were not represented by HR, hsCRP, MDA-LDL, or 8-isoprostane might contribute to the observed improvement in IMT.
We previously reported the effects of amlodipine and valsartan on vascular damage and ambulatory BP in 100 untreated hypertensive patients. (Ichihara et al. 2006a) The 12-month treatment with valsartan significantly decreased 24-h systolic BP, UAE, and PWV by 14 mmHg (9.4%), 18.6 mg/gCre (45.5%), and 182 cm/s (10.9%), respectively, and the decreases were similar to those of the telmisartan group observed in the present study [17 mmHg (11.5%), 23.7 mg/gCre (68.1%), and 190 cm/s (11.4%), respectively]. Neither 12-month treatment with valsartan or telmisartan significantly decreased the IMT of the carotid arteries. In addition, the 12-month treatment with amlodipine in our previous study significantly decreased 24-h systolic BP and PWV by 17 mmHg (11.3%) and 206 cm/s (12.0%), respectively, (Ichihara et al. 2006a) to the levels similar to those of the cilnidipine group observed in the present study [16 mmHg (10.7%) and 162 cm/s (9.8%), respectively]. Although the 12 or 24-month treatment with amlodipine was previously reported to reduce the UAE in elderly hypertensive patients with type 2 diabetes mellitus, (Fogari et al. 2000) our previous study showed that the 12-month treatment with amlodipine did not significantly decrease the UAE or IMT in untreated hypertensive patients. (Ichihara et al. 2006a) However, in the present study with a study design similar to our previous study, (Ichihara et al. 2006a) the 12-month treatment with cilnidipine significantly decreased the UAE and IMT by 12.5 mg/gCre (47.2%) and 0.18 mm (17.0%), respectively. These results suggest that the reduction in UAE or IMT is independent of the reduction in BP, and that the beneficial effects of cilnidipine are due to its inhibitory effects against N-type calcium channels. Since four hypertensive drugs which had decreased BP to a similar extent for 12 months similarly reduced the PWV, the reduction in PWV might be caused by the sustained reduction in BP itself.
In conclusion, both the 12-month treatments with telmisartan or cilnidipine similarly decreased the BP, the PWV predicting cardiovascular events, and the established surrogate maker, UAE, in untreated hypertensive patients. In addition, the 12-month monotherapy with cilnidipine significantly decreased the IMT, although the mechanism responsible for this effect requires further studies. Thus, cilnidipine and telmisartan are useful antihypertensive drugs for preventing vascular complication.
Support for Research
Ministry of Education, Science and Culture of Japan (16790474 and 17390249).
Footnotes
Acknowledgments
This work was supported in part by grants from the Ministry of Education, Science and Culture of Japan (16790474 and 17390249). We also appreciate the skillful secretarial work of Ms. Yukiko Prendergast and Ms. Shoko Watanabe.