
Abstract
Context
Patients are frequently transferred during their care for acute myocardial infarction. The clinical risks and benefits associated with inter-hospital transfer have not been fully evaluated.
Objective
To compare and contrast the analytic methods used to handle transferred patients in previous acute myocardial infarction research.
Design
Systematic review of acute myocardial infarction literature over the past 10 years.
Main Outcomes
Benefits and risks of various methods used for handling transferred patients in acute myocardial infarction research.
Results
Seven major methods for dealing with inter-hospital transfer emerged: 1) Count each hospitalization as a separate event. 2) Delete transferred patients from analysis. 3) Link the data from different hospitals and produce a record of the “episode” of acute myocardial infarction. 4) Analyze data on transferred patients the same as on non-transferred patients. 5) Transfer patients are the specific population of interest. 6) Diagnosis, treatment, outcomes are attributed to the index hospital. 7) Control for transfer in logistic regression modeling. Several studies included a combination of these methods.
Conclusion
Inter-hospital transfer in the care of acute MI is common and increasing. From a clinical standpoint, determining the patient most likely to benefit from inter-hospital transfer will help guide clinicians faced with this difficult decision. From a health services standpoint it is essential to understand the implications of using a particular method for handling transfer patients, the impact on data collection, the data lost, the appropriate analyses, and the generalizability of findings.
Background
Patients are frequently transferred during their care for acute myocardial infarction. The clinical risks and benefits associated with inter-hospital transfer have not been fully evaluated. Inter-hospital transfer, particularly out of rural regions also has serious implications for clinical care and health services research. 1 There has been a recent rise in medical publications, both clinical trials and editorials on whether inter-hospital transfer or local care is better.2–6 A thorough understanding of the issues surrounding inter-hospital transfer will lead to a better understanding of its impact on patient outcomes from both a clinical and health services perspective. Numerous studies have analyzed patients with acute myocardial infarction and have dealt with patient transfers in various ways. The purpose of this paper is to review the published methods for handling inter-hospital transfers and discuss the benefits and risks of each method.
Definitions of Transfer
Patients suffering acute MI are frequently transferred into or out of a hospital for further medical care. Published literature on acute MI is the product of research studies; hence, we use the term “study hospital” to define a hospital involved in a research study. A “non-study hospital” is a hospital not involved in that specific research study. Figure 1 provides a graphic description of acute MI patient flow from the point of initial patient presentation through the potential locations for treatment and movement between locations.

Transfer of patients Into and Out of a “study hospital”.
There are four groups of patients related to inter-hospital transfer in acute MI research. 1) Non-transferred patients are patients who receive all their care at one acute care hospital; from presentation, through treatment, to discharge. 2) Transfer-in patients are patients that are transferred into a study hospital. There is little or no data on the care they received prior to transfer into the study hospital. Transfer-in patients can be transferred in from another acute care facility or from an emergency department at another acute care facility. 3) Transfer-out patients are patients who are transferred out of a study hospital. Transfer-out patients can be initially admitted to the study hospital, receive care, and then transferred to another acute care facility, or can be transferred out directly from the emergency department. Subsequent non-study hospital care, procedures, discharge treatments, and outcomes are often not available for transfer-out patients. 4) There is a small group of patients admitted to a hospital, transferred only for a particular treatment (e.g. angiogram, angio-plasty), immediately returned, and subsequently discharged from the index hospital.
The unit of analysis is an essential component of any research on acute MI. In acute MI research the unit of analysis may be; 1) the patient, 2) the treating physician, or 3) the hospital. The study objective should determine the unit of analysis. The unit of analysis should then help direct the decision of how to handle transferred patients. For example, if the clinical question is the incidence of acute MI the unit of analysis should be the patient. Choosing the patient as the unit of analysis then requires linking of the multiple hospital-izations to get an accurate incidence rate. If the clinical question is the use of reperfusion for acute MI in community hospitals then the unit of analysis may be the hospital. In this case the essential data is from the index hospital during the first 12 hours after the patient presents. For hospitals without angioplasty capabilities it may also be necessary to collect data on the number of patients transferred specifically for reperfusion with angio-plasty or to obtain data from the second hospital. Because treatment for acute MI includes immediate treatment (first 2-6 hours) and later treatment (1-5 days), identifying the most appropriate manner for collecting patient specific data and for handling transferred patients is important for accurate results and conclusions. It may be more difficult to enroll patients from rural and smaller community hospitals into clinical trails due to small numbers and limited availability of research staff and resources.
Methods
We searched Medline using keywords; “acute myocardial infarction” or “myocardial ischemia” and “rural” or “transfer”. We limited this set to human, English language and publication from 1995-2004. This provided 326 articles for initial review. We deleted 93 articles that related to genetictransfer. Because inter-hospital transfer was not the primary question in the vast majority of these articles, the Medline search did not adequately identify all research on acute MI that analyzed transferred patients. Therefore, we also culled the general literature on care and treatment of acute MI and obtained additional articles by reviewing the bibliography and endnotes of articles on care and treatment of acute MI. Rather than an exhaustive review of acute myocardial infarction, the purpose of this paper is to provide a thorough review of the wide range of methods for dealing with inter-hospital transfer in the published literature. While not including every article on acute MI, our final sample includes the major studies and numerous smaller studies on acute MI that dealt with transferred patients. Our final sample of articles which will be cited individually in the appropriate section includes examples from the Cooperative Cardiovascular Project (CCP), National Registry of Myocardial Infarction (NRMI), Pennsylvania Health Care Cost Containment Council (PH4C), California Health Outcomes Project (CHOP), the State Health Reports for Connecticut, Georgia, Washington, Colorado, the National Center for Health Statistics (NCHS), National Institute of Health Heart Lung and Blood Institute Chart book (NIH/NHLBI), Myocardial Infarct Triage and Intervention project (MITI), the Dartmouth Health Atlas of Medicare patients and numerous other individual studies on acute MI.
Results
Seven major methods for dealing with inter-hospital transfer emerged: 1) Count each hospitalization as a separate event. 2) Delete transferred patients from analysis. 3) Link the data from different hospitals and produce a record of the “episode” of acute myocardial infarction, regardless of how many hospitalizations occurred. 4) Analyze data on transferred patients the same as on non-transferred patients. 5) Transfer patients are the specific population of interest. 6) Diagnosis, treatment, outcomes are attributed to the index hospital. 7) Control for transfer in logistic regression modeling. Table 1 summarizes these methods and gives a brief overview of the benefits and risks for each.
Benefits and risks of various methods for dealing with transfer patients in health services research.

Several other methods were used in individual smaller studies and reflect subtle differences from the major methods listed above. Many authors utilized a combination of methods to handle transferred patients. Figure 2 provides a graphic description of the major analytic methods on a theoretical sample of 200 acute MI patients.
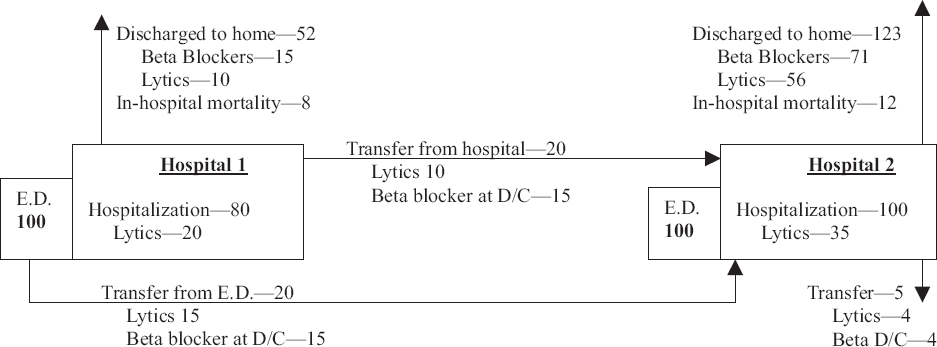
Theoretical treatment and outcomes of 200 patients with Acute MI depending on method of handling inter-hospital transfers.

Count each hospitalization as a separate event. Hospitalization is the unit of analysis in this method. This method provides a rough estimate of the incidence of acute MI and provides an accurate estimate of hospitalization for acute MI and the general utilization of health resources for acute MI. However, no linkage between hospitals is possible. Because each transferred patient accounts for 2 or more hospitalizations for acute MI, the true incidence of acute MI is less than the incidence of hospitalization for acute MI. The rate of inter-hospital transfers has increased rapidly over the last decade resulting in a growing discrepancy between hospitalization rate and incidence rate. 7 The discrepancy is particularly great in rural regions where a higher proportion of patients is transferred out for ongoing care of their acute MI. For studies on treatments and outcomes, counting each hospitalization will underestimate the treatment rates and mortality rates among the transferred patients.
Hospital discharge data does not include data on emergency department visits. Therefore, if a patient is transferred directly from the emergency department of one hospital to a second hospital they do not appear in the hospital discharge data from the first hospital.
The National Center for Health Statistics (NCHS), 8 National Institute of Health Heart Lung and Blood Institute Chart book (NIH/ NHLBI), 9 Dartmouth Health Atlas 10 of Medicare patients Dartmouth Health Atlas, and the state health reports for Connecticut, 11 Georgia, 12 Washington, 13 Colorado 14 utilize this method and base their published rates for disease and acute myocardial infarction on the number of hospital discharges making no attempt to correct for inter-hospital transfer. Their estimates of acute myocardial infarction incidence are likely inflated by 10-20% and even more so for rural regions. Kostis et al. used this method to determine time trends in “occurrence and outcome” of acute MI in New Jersey between 1986 and 1996. 15 Their estimate on the incidence of acute MI is likely overestimated because the transferred patients were counted twice. Their finding of a decrease in in-hospital mortality is inaccurate because of the increasing number of transferred patients who show up in the denominator for calculations of in-hospital mortality. In contrast, Naylor et al. linked hospitalization using a matching algorithm specifically to obtain an accurate denominator for calculation of case-fatality rates. 16
Delete transferred patients/data from analysis. There are four subsets within this major heading; a) delete all transferred patients, b) delete only transfer-in patients, c) delete only transfer-out patients. d) Transfer is an exclusion criterion for “ideal” candidate of therapy. Deleting transferred patients removes those patients from the study. If inter-hospital transfer were a random event, deleting transferred patients would have little impact on the study results. The published findings that transferred patients are more likely to be young, male, and have lower in-hospital mortality means that deleting transferred patients from the analysis introduces a major bias against hospitals with high transfer-out rates.1,17
Several CCP18,19 and NRMI20,21 publications deleted transferred patients from their analysis. Thiemann et al. reported from the CCP that mortality from acute myocardial infarction was higher in smaller and rural hospitals and in patients cared for by primary care physicians; however, they deleted 25% of their sample due to inter-hospital transfer. 22 Casale's report from the Pennsylvania data also found higher in-hospital mortality in rural hospitals and in patients cared for by primary care physicians. 23 Their study deleted over 9000 patients (23% of the total sample) due to inter-hospital transfer. Using the CCP data, Baldwin et al. reported specifically on rural patients with AMI. 24 They deleted patients transferred-in to the study hospitals. They found that patients transferred out of study hospitals were younger, less ill, and more likely to receive recommended treatments.
A method of patient identification that leads to inadvertent deletion of transfer-out patients is retrospective identification of acute MI patients from admission and discharge data. 25 Patients transferred from an emergency room to another hospital are not included because they do not appear in the transfer-out hospital discharge data. No information on the care provided in the first emergency room is available for analysis.
Deleting only transfer-in patients may be an attractive alternative because it still allows for analysis using large secondary and administrative datasets and decreases the risk of enriching the pool of patients in hospitals with high transfer-in rates. It may be appropriate for studying early treatment of MI.26,27 However, it also removes them from the transfer-out hospital patient pool, specifically in terms of later hospital care and discharge medications and treatments.
Similarly, deleting transfer-out patients from analysis penalizes hospitals with high transfer-out rates. Krumholz et al. deleted transfer-out patients because they could not determine their ultimate discharge medications. 28 At the time of transfer, many patients are not receiving beta-blockers, ace-inhibitors, and have not undergone revascularization. These transferred patients may receive these treatments at the second hospital, but because they did not receive them in the index hospital prior to discharge, the index hospital appears to have lower rates for these treatments. 29
Another method under this rubric is to include transferred patients but only include data from the index hospitalization. Transferred patients are identified by the “type of admission” code and hospital data on patients identified as transferred from another acute care facility are not included in analysis. This method is attractive as it allows for analysis of secondary databases and large administrative databases that include no way of linking multiple hospitalizations for a single patient. This method is effective for studying early treatment of acute MI and for studying the indications for inter-hospital transfer. However, because there is no data on subsequent hospitalizations in the transferred patients and no way to link hospitalizations, it is not possible to compare later treatments, discharge medications, and mortality. 30
Transferred patients may be deleted from the group of “ideal” candidates for specific treatments. 31 This is another mechanism similar to deleting transferred patients. For example, a patient is seen in an ER, diagnosed with ST elevation acute MI, treated with thrombolytics and transferred to an urban hospital. Because they were transferred they are not considered an “ideal” candidate and are excluded from the data analysis. Conversely, if they did not receive lytic therapy even though he/she was a candidate for it, because of transfer the patient is erroneously considered not an “ideal” candidate for therapy. Transferred patients are younger and healthier, thus more likely to be “ideal” candidates for therapy. However, because they are deleted, the transfer-out hospital does not get credit for providing treatment or take responsibility for not providing treatment.
Link the data from multiple hospitals and produce a record of the “episode” of acute myocardial infarction. This linking should occur prospectively so that a complete record of presentation, treatment, discharge, and outcome is collected. However, for large retrospectively collected data it is possible to link multiple hospitalizations for a single patient using matching algorithms or patient identifiers. The downside of linking hospitalizations is the increased cost and time necessary to create reliable “episodes” for individual patients.
One recent article utilizing CCP data attempted to link patients transferred between two CCP hospitals, but also deleted all patients in whom their first hospitalization was a transfer from a non-CCP hospital. 32 The Connecticut substudy of the CCP linked transfers between hospitals to study the impact of on-site catheterization. 33 They linked data for 3 years and found little difference in cost and mortality between hospitals with and without on-site catheterization.
The CHOP and MITI studies linked hospital transfers to produce a complete continuous record for each episode.34,35 The MITI also found that transferred patients were younger and had a lower mortality than patients who were not transferred. In contrast, the CHOP found higher rates of adverse outcomes among transferred patients. 36
Vermeer et al. studied a comparison between thrombolysis and primary PTCA in patients presenting to a hospital without PTCA capabilities. 37 A random sample of patients were transferred to a hospital with PTCA capabilities and then transferred back to the index hospital immediately or within one day. The authors linked the data from the transfer, however, in this case, the transfer was short and for one specific reason, therefore it did not require an enormous amount of extra work. Because transfer simply for a procedure and then transfer back to the index hospital is rare in the United States, it is unlikely that this type of analysis will become common.
Analyze data on transferred patients the same as on non-transferred patients. This method analyzes all patients the same, whether they were transferred in or out. This is a simple method for an individual hospital to analyze the care it provides and is accurate for hospitals with low transfer-in and transfer-out rates. This method works well for individual hospital quality improvement projects. Patil et al. studied the admissions for AMI to one hospital to better understand their own population of patients. 38 Because there is no subsequent data on transfer-out patients, this method may underestimate the treatments of smoking cessation, aspirin and beta-blockers on discharge. Because transfer-in patients have little data from their index hospital it may underestimate reperfusion strategies such as thrombolytics or early transfer for angioplasty. There is no inter-hospital linkage even for patients transferred between 2 study hospitals so an individual patient may be counted twice.
Transfer patients are the specific population of interest.39–41 This analysis studies the transferred patients as a separate group of specific interest. They may be compared to each other and to non-transferred patients. Comparisons between transferred and non-transferred patients should account for the demographic and clinical differences between these groups. Theroux et al. studied the impact of early treatment of acute MI in hospitals with high transfer-out rates. 42 While they reported differences in treatment and outcomes between transferred and non-transferred patients they caution that this comparison had “limited significance” due to the biased selection process inherent in non-randomized assignment of transfer. Madsen et al. conducted a randomized trial of transfer for PTCA with local conservative treatment. 43 They studied only patients with post infarction ischemia after the initial treatment for acute MI but prior to discharge. This randomized, controlled trial found improvement in clinical outcomes for patients undergoing the more invasive treatment.
Subsequent care/procedures are attributed to the index hospitalization. 44 This method requires linkage of data from multiple hospitalizations. It is attractive because the data from subsequent hospitalizations dealing with procedures, costs, and disposition can be obtained from administrative databases rather than requiring complete data from full chart abstraction from all hospitals involved in the care of the patient. However, this method focuses the unit of analysis on the index hospital and may overestimate the impact of early care. The index hospital gets credit for appropriately transferring patients for specialized care. The index hospital also gets “credit” for the care provided by subsequent hospitals/providers. 45 Hospitals with high transfer-in rates do not get adequate “credit” for the care they provide. Any subtle volume-outcome relationship will be lost because this method assumes that other than the major quality indicators, the care provided in all institutions is roughly equivalent.
Control for transfer differences with logistic regression modeling. Transferred and non-transferred patients are very different demo-graphically and clinically. Logistic regression attempts to control for these differences. Giles et al. only used data from the index hospitalizations to compare race and gender differences in rates of invasive cardiac procedures. 46 They attempted to control for transfer in their analysis. However, because transfer may occur specifically to obtain invasive cardiac procedures and transferred patients are substantially different than non-transferred patients, bias was introduced into the analysis. Regression analysis may not fully control for significant differences between transferred patients and non-transferred patients. It does not adequately control for the subtle differences between transfer-in patients and transfer-out patients and variations in the types of hospitals with high transfer-in or high transfer-out rates, for example, presence of E.R. Physicians, telemetry technicians, cardiac trained nurses, and the presence of an ICU. The official report from the Pennsylvania Health Care Cost Containment Council (PHC4) developed two regression models, one for patients admitted directly and one for transfer-in patients.47,48 While partially sorting out the assignment of “credit” and “responsibility”, because the transfer-in patients are younger and healthier, the PHC4 hospitals with high transfer-out rates are penalized by not including the transferred patients in their pool. 1
Several newer methods for controlling for differences have been recently proposed. Propensity score analysis uses a similar approach to logistic regression to control for differences in measured variables by replacing the multiple confounding covariates with one function of these covariates. 49 However, neither logistic regression nor propensity score analysis can control for unmeasured differences between patient populations.
Instrumental variable (IV) analysis attempts to control for the unmeasured patient differences often found in non-randomized retrospective and cross-sectional data. The goal of IV analysis is a post-hoc pseudo randomization of patients to better define the impact of a specific treatment. McClellan used IV analysis to determine the incremental benefit of angioplasty of elderly patients with acute MI. 50 Instrumental variable analysis is limited in application due to the difficulty identifying an appropriate instrumental variable and limited experience of health services researchers with this method.
Discussion
The inclusion, exclusion, or linkage of transferred patients in a study should be determined by the research question. Quality improvement studies may focus on the hospital admission as the unit of analysis, while studies on case-fatality or incidence should focus on the patient or episode of acute myocardial infarction. However, several large studies have utilized hospital discharges as a proxy measure for incidence of acute MI and inappropriate handling of transfers in other studies has lead to biased results.
Much of the problem has been due to uncertainty in whether transfer should be an independent variable or a dependent variable. That is, is transfer a treatment of acute myocardial infarction, an outcome of the treatment of acute myocardial infarction, or a neutral occurrence that has no relationship to treatment or outcomes? Many researchers have chosen to handle transfer as a neutral occurrence, but because transfer is so common and transferred patients are different than non-transferred patients have had difficulty adequately handling transfer status in their analysis.
Transfer issues related to clinical care
Ultimately, the goal of cardiac research is to improve patient care, decrease mortality, improve quality of life, and decrease unnecessary costs. The impact of inter-hospital transfer on clinical care is generally unknown. Only several studies were designed specifically to study transfer and these were looking at transfer for specific treatments, not transfer in general. Transfer muddies the waters of cardiac research and most research has dealt with transfer as a problem to be overcome rather than as an important component of care to be studied and understood. Overwhelmingly, the inferences made and conclusions published about transfer were done so based on studies not designated to answer any questions about transfer. Newer studies designed specifically to answer the question of whether immediate transfer for angioplasty is better than local care with intravenous thrombolysis promise to shed some light on this difficult decision. However, these trials need to include truly rural and remote communities in order to fully answer this important question. The impact of transfer for other acute MI care deserves further investigation.
Because transfer is increasingly common, understanding the risks and benefits is essential to providing the best care to patients suffering acute MI or acute coronary syndromes. The benefit of transfer to a hospital with a higher level of service seems intuitive. Certainly, patients who benefit from angioplasty, coronary artery bypass surgery, or invasive monitoring will, by definition, benefit from transfer to receive those services. The benefit to other groups is less clear. The volume/outcome relationship previously reported should be reinterpreted carefully due to the significant bias introduced into the analyses by deleting transferred patients. The potential downsides to transfer include; complications occurring during transport, delay in reperfusion therapy and other medical care, and separation of patients from their family and/or support group. Theroux et al. reported a higher rate of bleeding complications among the transferred patients in their study. 34 With the growing emphasis on the relationship between depression and acute MI mortality, the clinical impact of transferring a patient from their current social support network will also require further study. Additionally, the emerging interest in pay-for-performance provides additional impetus to clearly identify the care and outcomes associated with individual physicians and hospitals.51,52 As seen in Figure 2, the method chosen for handling transferred patients can dramatically alter the reported performance outcomes of interest to payors.
Transfer issues related to health services research
Health services researchers have spent considerable time evaluating the diagnosis and treatment of acute MI. As the number one cause of death in the U.S., even small changes in diagnostic accuracy and incremental improvement in outcome translates to hundreds if not thousands of patients with better outcomes each year.
Health services researchers have sought to determine the best physicians, hospitals, insurance programs, and delivery systems for acute MI care27,39. To do this requires the ability to determine the responsibility for the care patients receive. For patients cared for in 1 hospital by 1 physician this is simple. Add in a physician group, primary care v specialist care, co-insurance, and risk adjustment, and determining responsibility and/or credit becomes less clear. Move patients between hospitals and the relationship between care and outcomes becomes nearly impossible.
Commonly studied outcomes for acute MI include both intermediate outcomes (reperfusion therapy, use of aspirin, beta-blocker, ACE-Inhibitors, rehabilitation services, etc) and patient-oriented outcomes (mortality, quality of life, functional status). If there is a firm link between intermediate outcomes and final outcomes then measurement of intermediate outcomes may be appropriate. If there is no firm link between intermediate outcomes and final outcomes then it is important to measure final outcomes. For example, it is firmly established that aspirin is associated with a significant improvement in mortality for patients with acute MI. It is reasonable to measure aspirin use as an accepted measure of good care. The difference between reperfusion with lytics vs. angioplasty is less well established; therefore it is not adequate to simply measure the rate of angioplasty as a measure of good care. Transfer is an important unresolved issue in this sense. The link between transfer and outcomes has not yet been established; therefore it is essential to study inter-hospital transfer more rigorously. Many of these same issues have been identified in the area of trauma care; regionalization of trauma management, timing and method of patient transport53,54. Unfortunately, no clear outcomes data or consensus has emerged from the trauma transfer literature.
The focus in much cardiac research has been on describing differences and assigning responsibility rather than identifying the best strategy of care for patients with acute MI (Cardiologist v noncardiologist, rural v urban, males v females). The crucial question that addresses both the clinical care of acute MI and the health services questions on acute MI should be; what is the best process of care for this patient? The answer may be different depending on where the patient lives, what hospital the patient presents to, the type of acute MI or acute coronary syndrome the patient is suffering, the availability of specialized cardiac services and cardiology consultants. Not all patients with acute MI will present in the first hour of chest pain to a tertiary hospital with a high volume angioplasty lab during the regular workday. For patients presenting to rural and frontier hospitals, or urban hospitals without angiography services, what is the best process of care for this patient? In the context of inter-hospital transfer, which patient will benefit from transfer?
Conclusion
Inter-hospital transfer in the care of acute MI is common and increasing. Transfer patients have been handled in numerous ways in health research; from full inclusion to complete deletion from the analysis. While this article has focused on the issues surrounding transfer in acute MI, many of the issues are similar for transfer patients with other medical conditions. From a health services standpoint it is important to understand the implications of using a particular method for handling transfer patients, the impact on data collection, the data lost, the appropriate analyses, the generalizability of the findings. From a clinical standpoint it is crucial to further study the issue of inter-hospital transfer and determine the risks and benefits to transfer in acute MI care.
Competing Interests
The authors declare that they have no competing interests.
Authors' Contributions
The author warrants that his submission to the article is original and that he has full power to enter into this agreement. Neither this article nor a similar work has been published nor shall be submitted for publication elsewhere while under consideration by this Publication. Dr. Westfall conceived of the project, reviewed the literature, developed the conceptual models related to inter-hospital transfer and wrote the manuscript.
Footnotes
Aknowledgements
None to report