
Abstract
The objective of this document is to review the clinical applicability of coronary artery calcium (CAC) scoring in both asymptomatic and symptomatic patients at risk for cardiovascular disease. We begin by describing the pathological basis of atherosclerosis, the characteristic stages of atherosclerotic plaque development, and the mechanism and role of arterial calcification in advanced atherosclerotic lesions. We also explain the utility of CAC scoring in cardiovascular risk assessment, discuss the most current clinical methods for measuring CAC, and examine major clinical studies reporting CAC scores in both asymptomatic and symptomatic heart patients. Lastly, the current recommendations for CAC scoring as stated by the American College of Cardiology/American Heart Association (ACC/AHA) are outlined, and a number of considerations for future research are provided. Atherosclerosis begins when certain factors cause chronic endothelial injury, which eventually leads to the build up of fibrofatty plaques in the intima of arterial blood vessels. In time, blood vessel walls can weaken, thrombi can form and plaques can send emboli to distal sites. There are six characteristic stages of plaque development. Mature plaques may be calcified in an active process comparable to bone remodeling, where calcium phosphate crystals coalesce among lipid particles inside arterial walls. Calcification is only present in atherosclerotic arteries, and the site and levels of calcium are non-linearly and positively associated with luminal narrowing of coronary vessels. Calcification is also postulated to stabilize vulnerable plaques in atherosclerotic vessels. Recent studies have shown that CAC scoring can improve the management of both asymptomatic and symptomatic heart patients. Electron beam computed tomography (EBCT) and Multidetector computed tomography (MDCT) are two fast cardiac CT methods used to measure CAC. No matter what technique one uses, CAC is scored with either the Agatston or the “volume” score system. The ACC/ AHA currently finds it is reasonable for asymptomatic patients with intermediate Framingham risk scores (FRS) to undergo CAC assessment because these patients can be re-stratified into the high risk category if their CAC scores are ≥400. Conversely, CAC measurement in asymptomatic patients with low or high FRS is not warranted. There is also no evidence to suggest that high risk asymptomatic patients with no detectable coronary calcium should not be treated with secondary prevention medical therapy. For symptomatic patients, the ACC/AHA recommends CAC assessment as a second line technique to diagnose obstructive CAD, or when primary testing modalities are not possible or are unclear. Furthermore, they do not recommend the use of CAC measurement to determine the etiology of cardiomyopathy, to help identify patients with acute MI in the emergency room, or to assess the progression or regression of coronary atherosclerosis. Future research needs to incorporate calcium scores with percentile rankings, larger population samples, more women with at least intermediate Framingham risk, sufficient numbers of non-Caucasians, reports on cost-effectiveness, and data on populations with Chronic Kidney Disease, End Stage Renal Disease and Diabetes.
Introduction
Coronary artery calcification (CAC) is a pathological process related to atherosclerosis that has recently received significant attention by both scientists and clinicians alike. Consequently, it is essential to understand the basis and progression of these processes, how they are related, and how they can be used clinically to improve the management of patients at risk for cardiovascular disease. This review discusses the pathological basis of atherosclerosis, the characteristic stages of atherosclerosis, the mechanism and role of calcification in atherosclerotic plaque development, and the most current clinical methods for measuring coronary artery calcium. In addition, the utility of CAC scoring in cardiovascular risk assessment is explained, major clinical studies reporting CAC scores in both asymptomatic and symptomatic heart patients are examined, current recommendations as stated by the American College of Cardiology/American Heart Association are outlined, and future research needs are addressed.
Overview of Atherosclerosis and Coronary Artery Calcification
Atherosclerosis is responsible for more mortality and morbidity than any other disorder in Western society, leading to conditions such as myocardial infarction, stroke, aortic aneurysm and peripheral vascular disease. In light of its impact, it is essential to understand the pathologic basis of atherosclerosis and the characteristic stages of its progression. Currently, atherosclerosis is postulated to occur via a mechanism referred to as the response to injury hypothesis. This process begins with chronic endothelial injury caused by factors such as hyperlipidemia, hypertension, smoking, immune reactions and infectious agents. Endothelial injury subsequently leads to endothelial dysfunction by way of increased endothelial permeability, leukocyte adhesion and thrombotic potential. Around this time, lipoproteins such as LDL begin to accumulate in the vessel wall and are modified via oxidation. Monocytes and other leukocytes then adhere to the endothelium of the blood vessel, migrate into the intimal layer and transform into macrophages and foam cells. Platelets also begin to adhere and release factors such as platelet-derived growth factor, which signals smooth muscle cells to migrate from the media to the intima. While smooth muscle cells are proliferating in the intima, extracellular matrix synthesis increases and intra- and extracellular lipid accumulation is enhanced (1).
Atherosclerotic lesions are named according to Roman numerals that signify their particular stage of progression. The initial, or type I lesion, consists of atherogenic lipoprotein, macrophages and scattered foam cells, and is localized in areas of adaptive intimal thickening. Type II lesions, or fatty streaks, are flat lesions that form in the coronary arteries during adolescence and contain layers of foam cells and smooth muscle cells loaded with lipids. Type III, or intermediate lesions, are made up of the same components as Type II lesions, however, they also contain extracellular lipid droplets (mainly cholesterol and cholesterol esters) and substances that disturb the coherence of intimal smooth muscle cells. Type IV lesions, or atheromas, have a larger and more deleterious extracellular lipid core than Type III lesions, and can potentially produce symptoms. Type V lesions, or fibroatheromas, appear around the fourth decade of life and are characterized by a lipid core and a layered cap of thick fibrous connective tissue. Type V lesions can further be classified as significantly calcified type Vb lesions, or type Vc lesions that contain mostly fibrous connective tissue and minute amounts of lipid or calcium. Lastly, Type VI, or complicated lesions, are distinguished by fissure, hematoma, and/or thrombus (1, 2).
Investigators have recently focused much of their attention on the mechanism and role of calcification in atherosclerotic plaque development. Coronary artery calcification (CAC) is a process that occurs just after fatty streak formation during the development of atherosclerosis. While some calcified lesions appear as early as the second decade of life, most are observed in advanced atheromas and in the elderly. Although it is not completely clear how they form, calcium phosphate crystals (hydroxyapatite) have been found to coalesce among lipid particles inside arterial walls via an active process comparable to bone formation and remodeling. The calcium phosphate crystals are postulated to arise from vesicles that pinch off of cells that make up the vessel wall. Gamma carboxyglutamate (Gla) containing proteins, in addition to other polypeptides, are thought to play a major role in this process because of their high affinity for calcium and their known involvement in bone formation, mineralization and osteoblastic differentiation. Specifically, proteins such as osteonectin, osteopontin, osteocalcin and bone morphogenetic protein-2a have been implicated because of their localization in calcified atherosclerotic lesions (3).
It remains unclear why atherosclerotic blood vessels become calcified. Some believe calcification might serve to strengthen weakened atherosclerotic plaques in an effort to prevent future rupture, but the relationship between calcification and the probability of plaque rupture has not yet been established. Nevertheless, it is clear that calcification almost always occurs in atherosclerotic arteries as opposed to normal arteries, and that the site and amount of coronary calcium is nonlinearly and positively correlated with luminal narrowing of coronary vessels. Moreover, patients that have calcified plaque are also more likely to have non-calcified plaque, which are vulnerable to thrombosis and rupture (4).
Fast CT Methods and CAC Scoring
Coronary artery calcification can be detected and measured using a variety of imaging techniques. Some of these methods include but are not limited to plain chest radiography, fluoroscopy, cardiac CT (conventional, helical and electron beam computed tomography), intravascular ultrasound, MRI and echocardiography (3). In the past ten years, cardiac CT has made most considerable advancements compared to alternative imaging options. Specifically, Electron beam computed tomography (EBCT) and Multidetector computed tomography (MDCT) have become the two principal fast CT methods used to measure CAC (4).
Electron Beam Computed Tomography
EBCT was developed almost 20 years ago and is currently the best available method for measuring CAC. This technology uses a stationary multi-source/split-detector combination joined to a rotating scanning electron beam to produce 30-40, 3 mm serially sliced scans during the heart cycle. Electrocardiographic trigger time is determined by ECG tracing during the scanning process and is most commonly set at 80% of the R-R interval to diminish the effects of heart motion. The ultra fast scan acquisition times (80, 100 and multiples of 100 milliseconds per slice) of EBCT are particularly noteworthy because they decrease motion artifact and improve contrast-to-noise ratio. Moreover, fast acquisition times allow CAC to be assessed in 10-15 minutes with only seconds devoted to actual scanning time (5).
Multidetector Computed Tomography
Multidetector computed tomography is an additional fast CT method used to measure CAC. In contrast to EBCT, MDCT uses a traditional x-ray tube and a mechanical rotation device that physically circles around the patient. The photons generated within the tube traverse the patient and are recorded by an array of detectors that can take multiple (4 to 64) adjacent sections at the same time. Section thickness depends on the number of sections acquired, such that 8 sections have 2.5 mm section widths and 16 sections can have either 0.5-0.75 mm or 1-1.5 mm section widths. Present MDCT systems allow tube current and the number of x-ray photons to be increased, in contrast to EBCT which used a fixed tube current. In addition, MDCT can operate in axial mode or spiral mode, depending on whether the CT couch advances at a fixed speed or in a step-wise fashion. Axial mode moves the patient forward in a step-wise fashion and is currently the principal mode of MDCT used to measure CAC (5).
Radiation and Effective Dose
Computed tomography generates images using x-rays that can potentially increase a patients risk for cancer. Consequently, it is essential for clinicians to consider the safety of cardiac CT when assessing cardiovascular risk in patients. The amount of radiation a patient receives while undergoing CT screening is estimated by the effective dose, which is recorded in either millirem (mrem) or millisieverts (mSv) (100 mrem equals 1 mSv). CT examinations with effective doses of 10 mSv (equivalent to 1000 mrem) may be associated with a one in 2000 chance of fatal cancer. While this risk appears to be small, it can become significant if an increased number of patients receive CT scans more routinely. In terms of radiation, MDCT is at a disadvantage when compared to EBCT. Specifically, MDCT systems have an effective dose of 1 to 1.5 mSv for men and 1 to 1.8 mSv for women, whereas EBCT systems have an effective dose of 0.7 to 1 mSv for men and 0.9 to 1.3 mSv for women (5).
Calculating Calcium Scores
The Agatston method and the “volume” score method are two different scoring systems currently used to quantify coronary calcium (5). Agatston et al. (6) developed a way to score calcification by first calculating the area of hyperattenuating calcium lesions with X-ray attenuation coefficients above a threshold of 130 Hounsfield units for all pixels. This number is then multiplied by a density factor to derive an Agatston calcium score (ACS), reported for either single or total coronary arteries. Two limitations of this method include its requirement for 3 mm CT scan slice thicknesses, and its score variability caused by partial volume artifacts that may alter the density factor. Volumetric calcium scoring (VCS), developed by Callister et al. (7), resolves these issues to some extent by computing a volume above threshold and depending less on slice thickness.
Cardiovascular Risk Assessment and the Use of CAC Scoring
Cardiovascular risk assessment is usually the first step taken by clinicians to manage patients with cardiovascular risk factors, enabling them to categorize patients, predict future risk and select the most appropriate therapy (4). In 1948, a research project named the Framingham Heart Study was initiated to identify common factors that cause cardiovascular disease. A large number of study participants without prior cardiovascular complications were followed over time and a multifactorial scoring system was created based on determined risk factors such as diabetes, gender, LDL cholesterol, HDL cholesterol, blood pressure, cigarette smoking and age (8). Age and gender are the two most influential risk factors. This system is currently the most popular and valid algorithm used by United States physicians to assess 10-year absolute risk for hard CHD events such as angina pectoris, myocardial infarction, or coronary disease death. The National Cholesterol Education Program (NCEP) has created four, 10-year absolute risk categories (i.e. high, moderately high, moderate and low risk) based on the Framingham risk score and major risk factors. Specifically, high risk patients are those with CHD or CHD risk equivalents, including patients with two or more risk factors plus a >20% 10-year risk for hard CHD events. Moderately high risk patients are those with two or more risk factors plus a 10%-20% 10-year risk for hard CHD events. Moderate risk patients are those with two or more major risk factors plus a < 10% 10-year risk of hard CHD events and lower risk patients are those with one or less major risk factors (4).
Risk factors can be evaluated for their additive ability to predict future cardiovascular events (predictive power) by calculating a C-Statistic. A C-Statistic is the area under a receiver-operating characteristic (ROC) curve, where sensitivity of a risk factor is plotted against one minus its specificity. When determining the predictive power of a risk factor, an increase in the C-statistic would indicate that the risk factor has improved discriminative ability. The Framingham algorithm generally offers a C-statistic of about 0.8. Currently, investigators are interested in whether CAC scores obtained by fast cardiac CT methods could potentially be added to the Framingham algorithm to increase the C-statistic and discriminative ability. In other words, they are interested in whether CAC scores could serve as an additional risk factor to improve categorization and assessment of 10-year absolute risk in patients. In the past 5-10 years, fast cardiac CT and CAC measurement have clinically been used to facilitate CHD risk assessment and management in both asymptomatic and symptomatic patients (4).
CAC scoring in Asymptomatic Patients
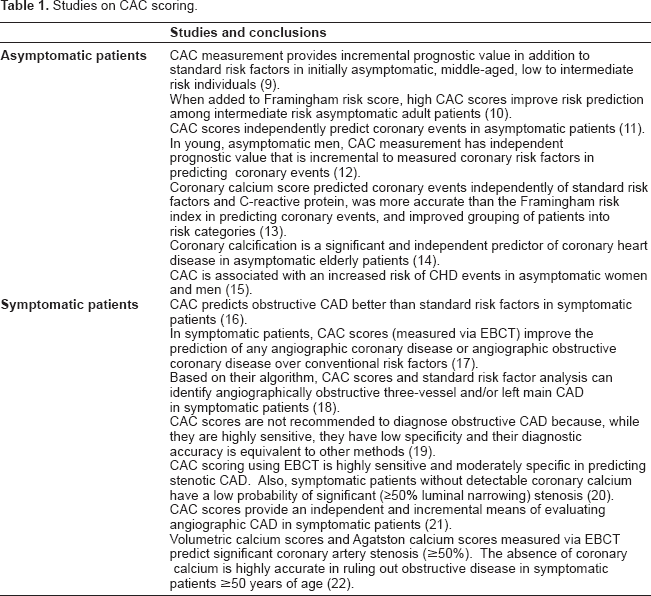
Prior to 2002, CAC scoring was not recommended as a means of assessing cardiovascular risk in asymptomatic patients because clinical evidence of its utility was limited. Recent studies have addressed this issue by incorporating hard endpoints such as MI and CHD death, and data on the independent prognostic value of CAC measurement (Table 1) (4). Kondos et al. (9) investigated the association between CAC levels (measured via EBCT) and cardiac events in initially asymptomatic, low- to intermediate-risk individuals. The study was performed in 8855 self-referred adults aged 30 to 76 years who had their CAC screened and were followed up after 37 ± 12 months. Men experienced 192 events that were associated with CAC (relative risk (RR) = 10.5, p < 0.001), diabetes (RR = 1.98, p = 0.008), and smoking (RR = 1.4, p = 0.025), while women experienced 32 events that were only associated with CAC (RR = 2.6, p = 0.037). Moreover, CAC measurement was found to offer incremental prognostic information on top of other risk factors. Overall, the authors concluded that CAC measurement provides incremental prognostic value in addition to standard risk factors in initially asymptomatic, middle-aged, low to intermediate-risk individuals. In a comparable study, Greenland et al. (10) wanted to establish whether CAC scores combined with Framingham risk scores (FRS) have superior prognostic value than either method alone when evaluating asymptomatic adult patients. They conducted a prospective, observational, population-based study of 1461 asymptomatic adults, where persons with at least 1 coronary risk factor received CT examination and were followed yearly for up to 8.5 years. Of the 1312 participants included in the study, 84 experienced MI or CHD death and 70 patients died of any cause. In addition, there were 291 (28%) participants with an FRS of more than 20% and 221 (21%) with a CAC score of more than 300. An FRS of more than 20% predicted the risk of MI or CHD death when compared with an FRS of less than 10% (HR, 14.3; 95% CI, 2.0-104; p = 0.009). Moreover, a CAC score of more than 300 was predictive of MI or CHD death when compared with a CAC score of zero (HR, 3.9; 95% CI, 2.1-7.3; p < 0.001). Lastly, CAC score predicted coronary risk among patients with an FRS higher than 10% (p < 0.001), but not among those with an FRS less than 10%. Overall, the authors concluded that when added to FRS, high CAC scores improve risk prediction among intermediate risk adult patients. In a systematic meta-analysis, Pletcher et al. (11) searched for studies published between 1980 and 2003 that measured CAC scores in asymptomatic subjects and that followed those subjects for coronary events. Publications also had to report score-specific relative risks that were adjusted for risk factors. The authors estimated adjusted relative risks for three CAC score categories (1-100, 101-400, and >400), compared those categories with a CAC score of 0, and used a random-effects model for meta-analysis. CAC scores between 1 and 100 had an adjusted relative risk of 2.1 (95% CI, 1.6-2.9), while higher calcium score categories had higher relative risk estimates that varied significantly between 3.0 and 17.0. Overall, the authors concluded that the CAC scores independently predict coronary events in asymptomatic patients. Taylor et al. (12) examined the independent predictive value of CAC measurement for coronary outcomes such as acute coronary syndrome and sudden death. They evaluated a non-referred cohort of 2000 men and women (mean age 43 years) using measured coronary risk variables and coronary calcium scores. The men experienced a total of 9 coronary events where 7 of 364 men had coronary calcium (1.95%) and 2 of 1,263 men did not have coronary calcium (0.16%; p < 0.0001 by log-rank). Moreover, coronary calcium was associated with an 11.8-fold increased risk for developing CHD (p = 0.002) after controlling for the Framingham risk score. Participants with coronary artery calcification also displayed an incremental increase in the risk of coronary events across coronary calcium tertiles (hazard ratio (HR) 4.3 per tertile). Overall, the authors concluded that in young, asymptomatic men, CAC measurement has independent prognostic value that is incremental to measured coronary risk factors in predicting coronary events. In a similar study, Arad et al. (13) had two primary objectives: 1) To determine the prognostic accuracy of EBCT scanning of the coronary arteries; and 2) To investigate the relationship of CAC to standard risk factors and C-reactive protein (CRP) in predicting atherosclerotic cardiovascular disease (ASCVD) events in healthy middle-age persons. Their participants included 4,903 asymptomatic persons aged 50 to 70 years that underwent EBCT scanning of the coronary arteries and were followed up at 4.3 years. Subjects that experienced at least one ASCVD event (119 of the 4,613) had higher baseline coronary calcium scores than those without events (median = 384, interquartile range = 127800 vs median = 10, interquartile range = 0-86, (p < 0.0001)). Also, when comparing coronary calcium score thresholds of ≥100 versus < 100, the relative risks (95% confidence interval (CI)) were 9.6 (6.7 to 13.9) for all ASCVD events, 11.1 (7.3 to 16.7) for all CAD events, and 9.2 (4.9 to 17.3) for non-fatal myocardial infarction and death. Overall, the authors found that coronary calcium score predicted coronary events independently of standard risk factors and CRP (p = 0.004), was more accurate than the Framingham risk index in predicting coronary events (area under the ROC curve of 0.79 ± 0.03 vs 0.69 ± 0.03, p = 0.0006), and improved grouping of patients into risk categories (p < 0.0001). In a related study, Vliegenthart et al. (14) examined the prognostic value of CAC scores (measured via EBCT) in 1795 asymptomatic elderly participants (mean age, 71 years; range, 62 to 85 years) as part of the Rotterdam Study. Of the participants included in the study, 88 cardiovascular events (including 50 coronary events) occurred during a mean follow-up time of 3.3 years. Multivariate-adjusted relative risk of coronary events were 3.1 (95% CI, 1.2-7.9) for calcium scores between 101 and 400, 4.6 (95% CI, 1.8-11.8) for scores between 401 and 1000, and 8.3 (95% CI, 3.3-21.1) for scores >1000, when compared with calcium scores between 0 and 100. Risk prediction was also improved after adding CAC scores to standard cardiovascular risk factors. Overall, the authors concluded that coronary calcification is a significant and independent predictor of coronary heart disease in the elderly. LaMonte et al. (15) studied the association between CAC score and coronary events in 10,746 healthy asymptomatic adults (aged 22-96 years) by measuring their CAC via EBCT at baseline and following them for a mean of 3.5 years. Of the total participants included in the study, 81 hard events (CHD death, nonfatal MI) and 287 total events (hard events plus coronary revascularization) took place. Age-adjusted rates (per 1,000 person-years) of hard events were calculated for four CAC categories (1 undetectable CAC category plus 3 detectable incremental sex-specific CAC categories). Rates were 0.4, 1.5, 4.8, and 8.7 (trend p < 0.0001) respectively for men, and 0.7, 2.3, 3.1, and 6.3 (trend p = 0.02) respectively for women. CAC levels were also shown to be positively correlated with total CHD events in both women and men (trend p < 0.0001 each), even after adjusting for risk factors. Lastly, CAC was associated with CHD events in persons with no baseline CHD risk factors and in younger (aged <40 years) and older (aged >65 years) study participants. The authors concluded that CAC is associated with an increased risk of CHD events in asymptomatic women and men.
Studies on CAC scoring.
The American College of Cardiology Foundation (ACCF) Task Force on Clinical Expert Consensus Documents (CECD) has established management guidelines based on all of the available data regarding the prognostic value CAC measurement in asymptomatic patients (Table 2). Specifically, they consider it reasonable for asymptomatic patients with intermediate FRS (10%-20% 10-year estimated risk of coronary events) to undergo CAC assessment because these patients can be re-stratified as high risk if their CAC scores are ≥400. Conversely, CAC measurement in asymptomatic patients with low FRS (<10% 10-year estimated risk of coronary events) is discouraged because of its limited clinical value. Similarly, asymptomatic patients with high FRS (>20% 10-year estimated risk of coronary events) do not require CAC assessment because they are already eligible to receive aggressive therapy based on the National Cholesterol Education Program guidelines. Currently, there is no evidence to suggest that high risk asymptomatic patients with no detectable coronary calcium (CAC = 0) can go without medical treatment (4).
ACC/AHA recommendations for CAC scoring (4).

CAC Scoring and Obstructive CAD in Symptomatic Patients
Various diagnostic modalities such as stress electrocardiography, myocardial perfusion imaging and echocardiography have historically been used to predict obstructive CAD (4). Recent studies, however, have evaluated the potential of CAC scores as a noninvasive method to predict obstructive angiographic CAD in symptomatic patients (Table 1). Kennedy et al. (16) sought to compare the independent predictive power of CAC scores versus conventional risk factors in diagnosing obstructive angiographic CAD in symptomatic patients. Their study included 368 symptomatic patients with coronary risk factors that underwent coronary angiography and CAC assessment via EBCT. Of the total number of participants included in the study, 158 (43%) had obstructive angiographic CAD (defined as >50% luminal stenosis) and 297 (81%) had CAC. Using bivariate analysis, the authors found that male sex and log-transformed coronary calcification were predictive of angiographic disease (p = 0.008, p = 0.001), whereas multivariate analysis indicated that male sex and coronary calcification were predictive of angiographic disease (p = 0.001, p = 0.001). Moreover, coronary calcification demonstrated a 90% negative predictive value and was found to have a stronger predictive power than conventional risk factors based on ROC analysis. Overall, the authors concluded that CAC predicts obstructive CAD better than standard risk factors in symptomatic patients. In an analogous study, Guerci et al. (17) were interested in whether the addition of CAC scores to standard cardiac risk factors could improve the prediction of angiographic obstructive CAD in symptomatic patients. Study participants included 290 men and women undergoing coronary angiography whose CAC scores were measured and whose standard cardiac risk factors were assessed. The authors found that CAC scores >80 were independently associated with an increased chance of any coronary disease regardless of the number of risk factors, and that CAC scores ≥ 170 were independently associated with an increased likelihood of obstructive coronary disease regardless of the number of risk factors (p < 0.001). Overall, they concluded that in symptomatic patients, CAC scores (measured via EBCT) improve the prediction of any angiographic coronary disease or angiographic obstructive coronary disease over conventional risk factors. In a different study, Schmermund et al. (18) were interested in creating an algorithm for identifying angio-graphically obstructive three-vessel and/or left main disease using standard cardiac risk factors and CAC scores. Their study included 291 patients with suspected CAD who underwent coronary angiography and coronary calcium assessment via EBCT. Of the total number of participants included in the study, 68 (23%) had angiographic three-vessel and/or left main CAD. Male sex, diabetes, left anterior descending CAC scores and circumflex CAC scores were all found to independently predict three-vessel and/or left main CAD by way of multiple logistic regression analysis. The authors used these four variables to create the following noninvasive index (NI): log(e)(LAD score) + log(e)(LCx score) + 2[if diabetic] + 3[if male]. ROC analysis of the noninvasive index yielded an area under the curve of 0.88 ± 0.03 (p < 0.0001), with various NI cutpoints showing 87%-97% sensitivity and 46%-74% specificity. NI values > 14 increased the probability of angiographic three-vessel and/or left main CAD from 23% to 65%-100%, and NI values <10 increased the probability of no three-vessel and/or left main CAD from 77% to 95%-100%. Overall, the authors concluded that based on their algorithm, CAC scores and standard risk factor analysis can identify angiographically obstructive three-vessel and/or left main CAD in symptomatic patients. In 2000, the American College of Cardiology (ACC) and the American Heart Association (AHA) published a consensus document that contained a meta-analysis of 16 studies evaluating the diagnostic accuracy of EBCT for detecting obstructive CAD (19). The studies included a total of 3683 symptomatic patients without prior coronary disease or cardiac transplantation, that underwent cardiac catheterization for diagnosis of obstructive CAD. An average of 57.2% of the patients reported significant coronary disease and an average of 65.8% of the patients reported significant CAC. The weighted-average sensitivity and specificity of CAC scores to predict obstructive CAD were 80.4% and 39.9%, respectively, while the pooled sensitivity and specificity were 90.5% and 49.2%, respectively. Abnormal coronary calcium score elevated the summary odds 20-fold (95% CI, 4.6 to 87.8). Moreover, summary odds increased from 6.8-fold (95% CI, 3 to 15.6) to 16.4-fold (95% CI, 5.1 to 53.1) to 50-fold (95% CI, 24.1 to 103.0) for detecting >50% and >70% stenosis, respectively. Higher coronary calcium scores were more accurate in detecting significant coronary disease, and a threshold of detectable calcium (CAC score ≥5) was associated with 25.6-fold increased odds of significant CAD (95% CI, 9.6 to 68.4). Overall, the authors did not recommend using CAC scores to diagnose obstructive CAD because, while CAC scores are highly sensitive, they have low specificity and their diagnostic accuracy is equivalent to other methods. Haberl et al. (20) correlated CAC scores and coronary angiography results to assess the value of CAC scores in evaluating CAD in symptomatic patients. Their study included 1,784 patients (1,225 men and 539 women) with suspected CAD that underwent coronary angiography and CAC screening. Significant coronary stenosis, defined as ≥50% luminal narrowing, was observed in 50% of men and 47% of women. Fourteen percent of the patients had no detectable coronary calcium, which was associated with a < 1% probability of stenosis. As CAC scores increased in age groups, the sensitivity to detect stenosis decreased and the specificity increased in both men and women. Overall, the authors concluded that CAC scoring using EBCT is highly sensitive and moderately specific in predicting stenotic CAD. They also concluded that symptomatic patients without detectable coronary calcium have a low probability of significant (≥50% luminal narrowing) stenosis. In a related study, Budoff et al. (21) incorporated CAC scores in a model to predict angiographic CAD in symptomatic patients. Their study included 1,851 patients with suspected CAD who underwent coronary angiography and had their CAC scored via EBCT. CAC scores were added to logistic regression models to predict severity and extent of angiographically significant CAD. CAC scores demonstrated 95% sensitivity and 66% specificity overall for predicting obstructive angiographic CAD. As calcium scores progressively increased, the sensitivity to predict stenosis decreased, while the specificity to predict stenosis increased. Moreover, the logistic regression model displayed excellent discrimination (ROC curve area, 0.842 ± 0.023) and calibration (chi-squared goodness of fit, 8.95; p = 0.442). Overall, the authors concluded that CAC scores provide an independent and incremental means of evaluating angiographic CAD in symptomatic patients. In a different study, Knez et al. (22) investigated age-and gender-based distribution of the CAC scores in a large group of symptomatic patients with suspected coronary artery disease. A total of 2,115 patients, including 1,404 men (63 ± 18 years old) and 711 women (59 ± 15 years old), received coronary angiography and CAC assessment via EBCT. CAC levels were measured using both volumetric calcium scoring (VCS) and Agatston calcium scoring (ACS). Patients with positive calcium scores (n = 1,789) had mean values of 323 ± 842 for ACS and 310 ± 714 for VCS (p = 0.83), with a Pearson's correlation coefficient of 0.99 between methods. Significant CAD was observed in 62% of men and 54% of women, and total calcium scores were significantly different for patients with or without CAD (492 ± 1,124 vs 76 ± 217 for ACS (p <0.01) and 486 ± 940 vs 53 ± 175 for VCS (p < 0.01)). In addition, CAD was found in the 326 patients (n = 208 men) without coronary calcium, and calcium was not found in 7 of 872 men and in 1 of 383 women who had significant CAD. CAC scores had an overall sensitivity and specificity of 99% and 28%, respectively, for predicting obstructive angiographic disease. Overall, the authors concluded that VCS and ACS measured via EBCT predicted significant coronary artery stenosis (≥50%), and that the absence of coronary calcium is highly accurate in ruling out obstructive disease in symptomatic patients ≥50 years of age.
Based on all of the available research, the American College of Cardiology (ACC) and the American Heart Association (AHA) have reached certain conclusions regarding the use of CAC scores in symptomatic patients (Table 2). Specifically, they found that CAC scores have a high sensitivity and negative predictive value for evaluating obstructive CAD, but they are not very specific. Furthermore, CAC scores <100 are associated with very low probability of abnormal nuclear stress tests or cardiac catheterization (<2% and <3%, respectively). Overall, CAC assessment is only recommended as a second line technique to diagnose obstructive CAD, or when primary testing modalities are not possible or are unclear (4).
Other Potential Uses of CAC Scoring
CAC measurement has other potential uses such as determining the etiology of cardiomyopathy, improving the triaging of chest pain patients in the emergency room, and assessing the progression or regression of coronary atherosclerosis. Some studies have shown that CAC scoring can distinguish ischemic from non-ischemic cardiomyopathy, and that it might be more accurate than conventional methods (23, 24). In addition, studies have indicated that CAC scores might facilitate the triaging of patients with chest pain and non-specific electrocardiograms by improving the identification of acute MI (25). Recent evidence also suggests that CAC monitoring can be used to modify treatment for CAD and can assess changes in cardiovascular disease prognosis. Nevertheless, more studies need to confirm that: 1) coronary calcium progression is biologically related to atherosclerosis; 2) coronary calcium progression can be detected relative to inter-test variability; 3) changes in the amount of coronary calcium relate to prognosis; and 4) coronary calcium progression can be altered by modifying cardiovascular risk factors. Overall, CAC scoring has a variety of potential applications in the future, however, more conclusive evidence and data need to be acquired to warrant its use. Currently, the ACC/AHA does not recommend CAC scoring for any of the purposes just discussed (Table 2) (4).
Summary and Conclusions
Atherosclerosis is a process characterized by the build up of fibrofatty plaques in the intima of arterial vessels. It begins when certain factors cause chronic endothelial injury, which subsequently increases endothelial permeability, leukocyte adhesion and thrombotic potential. Platelets, leukocytes and LDL accumulate in the vessel wall and smooth muscle cells migrate from the media to the intima. Ultimately, blood vessel walls can weaken, thrombi can form and plaques can send emboli to distal sites. Atherosclerotic plaques undergo a characteristic development that begins with an initial lesion and progresses into fatty streaks, intermediate lesions, atheromas, fibroatheromas and complicated lesions. Mature plaques may be calcified in an active process comparable to bone remodeling where calcium phosphate crystals coalesce among lipid particles inside arterial walls. Proteins such as osteonectin, osteopontin, osteocalcin and bone morphogenetic protein-2a have been implicated to play a role in this process. Although the exact relationship between atherosclerosis and calcification has yet to be resolved, calcification is only present in atherosclerotic arteries, and the site and levels of calcium are non-linearly and positively associated with luminal narrowing of coronary vessels. Calcification has also been postulated to stabilize vulnerable plaques in atherosclerotic vessels, but this relationship remains unclear.
Cardiovascular risk assessment is the first step a physician must take when managing patients with cardiovascular risk factors. The Framingham Heart study produced the most popular and valid algorithm used by United States physicians to assess 10-year absolute risk for hard CHD events. Essentially, a multifactorial scoring system was created based on determined risk factors such as diabetes, gender, LDL cholesterol, HDL cholesterol, blood pressure, cigarette smoking and age. Patients are categorized into low, intermediate, or high risk depending on their Framingham score. Recently, investigators have been interested in whether CAC scores could be added to the Framingham algorithm to improve cardiovascular risk assessment in intermediate risk, asymptomatic patients. Many of these studies evaluate the additive ability of CAC scores to predict future cardiovascular events by calculating the area under a receiver-operating characteristic (ROC) curve, or a C-statistic. An increase in the C-statistic indicates that the risk factor has improved discriminative ability. Based on all of the available research, the ACC/AHA currently finds it is reasonable for asymptomatic patients with intermediate FRS to undergo CAC assessment because these patients can be re-stratified into the high risk category if their CAC scores are ≥400. Conversely, CAC measurement in asymptomatic patients with low FRS is discouraged because of its limited clinical value. Asymptomatic patients with high FRS do not require CAC assessment either because they are already eligible to receive aggressive therapy. There is no evidence to suggest that high risk asymptomatic patients with no detectable coronary calcium (CAC = 0) can go without medical treatment. Many studies have evaluated the diagnostic value of CAC scores in symptomatic patients with obstructive coronary artery disease (CAD) as well. Based on this research, the ACC/AHA only recommends CAC assessment as a second line technique to diagnose obstructive CAD, or when primary testing modalities are not possible or are unclear. Also, the ACC/AHA does not at this time recommend the use of CAC measurement to determine the etiology of cardiomyopathy, to help identify patients with acute MI in the emergency room, or to assess the progression or regression of coronary atherosclerosis.
Future studies concerning the role of CAC scores in cardiovascular disease must address several issues. Specifically, most studies have reported CAC levels in terms of absolute scores, however, investigators must now focus on reporting calcium scores with percentile rankings, as these are clinically more useful for prognosis (4). Furthermore, CAC measurement has been shown to overestimate cardiovascular risk due to selection bias, creating the need for studies that include large population samples (10, 14). As far as gender and ethnicity are concerned, future studies should include more women with at least intermediate Framingham risk, and a sufficient number of non-Caucasians. Cost-effectiveness is another question that must be addressed because current data has not unequivocally established that CAC scoring enhances and prolongs life. Lastly, future studies must include data on populations with Chronic Kidney Disease, End Stage Renal Disease and Diabetes (4).