
Abstract
The atheroprotective role of high-density lipoprotein cholesterol (HDL-C) in cardiovascular disease has been unequivocally established, and epidemiological data have clearly demonstrated a strong inverse relationship between HDL-C levels and the risk of cardiovascular events, which is independent of the low-density lipoprotein cholesterol (LDL-C) levels. Thus, it would be logical to hypothesize that raising HDL-C might potentially lead to a reduction of cardiovascular risk. Cholesteryl ester transfer protein (CETP) promotes the transfer of cholesteryl esters from HDL to very low-density lipoprotein and LDL. Therefore, CETP inhibition raises HDL-C levels and decreases LDL-C levels. The first trials with CETP inhibitors failed to show a reduction in cardiovascular events. However, newer CETP inhibitors with more favorable effects on lipids are presently being tested in clinical trials with the hope that their use may lead to a reduction in cardiovascular risk. This review aims to provide the current evidence regarding CETP inhibition, as well as the clinical and scientific data pertaining to the new CETP inhibitors in development.
Keywords
Introduction
The role of low-density lipoprotein cholesterol (LDL-C) in the pathophysiology of atherosclerosis has been unequivocally established, and the use of LDL-lowering agents, especially statins, has led to a significant reduction of cardiovascular events in both primary 1 and secondary 2 prevention. However, a significant cardiovascular risk remains even after the achievement of optimal LDL concentrations, and among the major statin trials, the maximum relative risk reduction has not exceeded 47%.3,4
On the other hand, epidemiological data have clearly demonstrated a strong inverse relationship between high-density lipoprotein cholesterol (HDL-C) levels and the risk of cardiovascular events, which is independent of the LDL-C levels and remains relevant even when LDL-C levels are below 70 mg/dL.4–6 Furthermore, the absolute benefits of LDL lowering are greater in patients with low HDL-C concentrations.4,7 Thus, extensive research is being carried out to identify new HDL-raising drugs in the hope that this would lead to further reduction of cardiovascular risk, and cholesteryl ester transfer protein (CETP) inhibitors are being actively studied for that purpose.
CETP Inhibitors
CETP is a hydrophobic glycoprotein that is secreted mainly from the liver, predominantly derived from Kupffer cells, 8 and circulates in the plasma, bound mainly to HDL. In individuals with essentially normal lipid levels, CETP concentration is ~1-4 μg/mL,9,10 while the concentration may be 70-80% higher among those with hyperlipidemia.10,11 The role of CETP is to promote the transfer of cholesteryl esters from HDL to very low-density lipoprotein and LDL. 12 Therefore, CETP inhibition raises HDL-C levels and decreases LDL-C levels (Fig. 1). CETP inhibition became an attractive antiatherogenic target when rodents lacking plasma CETP activity were found to have elevated HDL levels and resistance to diet-induced atherosclerosis.10,12 Subsequently, patients with CETP gene mutations were also found to have elevated HDL levels and decreased incidence of coronary heart disease (CHD).13,14
ABCA1-specific Cholesterol Efflux Capacity (CEC).
Torcetrapib
The first CETP inhibitor studied was torcetrapib. In animal studies, torcetrapib has been shown to inhibit the development of atherosclerosis.
15
Furthermore, in human studies, torcetrapib produced a dose-dependent increase of HDL-C up to 106% and a reduction in LDL-C up to 42%.16,17 Thus, the “Investigation of Lipid Level Management to Understand Its Impact in Atherosclerotic Events” (ILLUMINATE) trial was conducted to test the hypothesis that torcetrapib would decrease cardiovascular events in high-risk populations.
18
In this study, 15,067 patients at high cardiovascular risk were randomized to receive atorvastatin plus 60 mg of torcetrapib daily versus atorvastatin plus placebo. In patients who received torcetrapib, there was an increase of 72.1% in HDL-C and a decrease of 24.9% in LDL-C, as compared with baseline (
In another independent parallel study called the “Investigation of Lipid Management Using Coronary Ultrasound to Assess Reduction of Atherosclerosis by CETP Inhibition and HDL Elevation” (ILLUSTRATE), it was shown that there was no difference on atherosclerosis plaque burden using combination therapy of torcetrapib plus atorvastatin versus atorvastatin alone. 20 Furthermore, in two other double-blind, randomized trials, the combination of torcetrapib and atorvastatin, compared with atorvastatin alone, failed to decrease the rate of progression of carotid intima-media thickness in patients with heterozygous familial hypercholesterolemia (RADIANCE 1) 21 and mixed dyslipidemia (RADIANCE 2). 22 In view of these disappointing results, development of torcetrapib was subsequently abandoned.
Dalcetrapib
The second CETP inhibitor studied was dalcetrapib. In phase 2 studies, dalcetrapib reduced CETP activity and produced a dose-dependent increase of HDL-C up to 36% without any significant effects on LDL-C levels. In addition, blood pressure, aldosterone production, cytochrome P450 11B2 messenger ribonucleic acid levels, NO-dependent endothelial function, markers of inflammation, and oxidative stress were not affected by dalcetrapib.23,24
Thus, the “Effects of Dalcetrapib in Patients with a Recent Acute Coronary Syndrome” (dal-OUTCOMES) trial was conducted to assess the effect of dalcetrapib on cardiovascular outcomes.
25
In this study, 15,871 patients with an acute coronary syndrome 4-12 weeks prior to enrollment were randomized to receive 600 mg of dalcetrapib versus placebo, in addition to the best available evidence-based care (including statins). The primary efficacy end point was a composite of death from CHD, nonfatal myocardial infarction, ischemic stroke, unstable angina, or cardiac arrest with resuscitation. Over the course of the trial, HDL-C levels increased from baseline by 31%-40% in the dalcetrapib group versus 4%-11% in the placebo group. Dalcetrapib had a minimal effect on LDL-C levels. Similarly, at the end of the trial, there was a 9% increase in the levels of apolipoprotein A1 (Apo-A1), while there was a minimal only effect on the levels of apolipoprotein B (Apo-B). However, the trial was halted after a second interim analysis because as compared with placebo, dalcetrapib did not alter the risk of the primary end point (cumulative event rate of 8.0% and 8.3%, respectively; HR with dalcetrapib = 1.04;
It has to be noted though that a more recent study showed that the effects of dalcetrapib on atherosclerotic outcomes were determined by polymorphisms in the ADCY9 gene, with approximately one in five patients having the appropriate genetic profile and thus deriving substantial protection against cardiovascular events. 26 Thus, as the authors suggested, a prospective pharmacogenomics-guided clinical trial may need to be performed in these responsive patients to allow regulatory review of results and provide personalized cardiovascular therapy with dalcetrapib. Actually, this observation may provide a greater source of hope for CETP inhibitors than the current trial methodology.
Potential Reasons for which CETP Inhibition may not Lead to a Reduction in Cardiovascular risk
There are several hypotheses attempting to explain the failure of the CETP inhibitors that have been tried so far to reduce cardiovascular risk. Of course, as it was mentioned earlier, the torcetrapib-evoked off-target hyperaldosteronism is considered to be the main reason for the disappointing results of torcetrapib in the ILLUMINATE trial.18,19 Furthermore, in a study in spontaneously hypertensive rats, torcetrapib induced a sustained impairment of endothelial function, decreased endothelial nitric oxide synthase mRNA and protein, as well as NO release, and it stimulated vascular reactive oxygen species and endothelin production. 27
On the other hand, the absence of any meaningful effect of dalcetrapib on LDL-C and Apo-B levels 25 and its neutral effect on NO-dependent endothelial function, as it was mentioned earlier, 24 may be at least partially responsible for the failure of dalcetrapib to reduce cardiovascular events. Another interesting observation is that dalcetrapib increased the level of C-reactive protein (CRP) by 18% compared to placebo in the dal-OUTCOMES trial. 25 The clinical significance of this observation is questionable, but it may potentially indicate vascular inflammation.
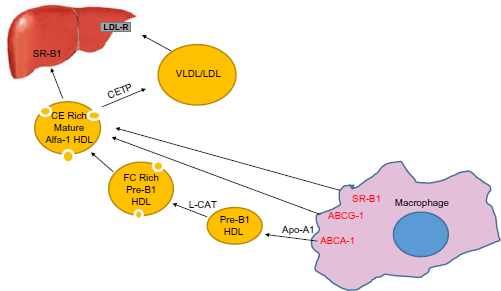
On the other hand, the role of CETP inhibitors in the macrophage-to-feces reverse cholesterol transport (RCT) remains unclear. Macrophage-to-feces RCT is a critical antiatherogenic process and involves efflux of excess cellular cholesterol from arterial macrophages to extracellular HDL-based acceptors through the action of transporters, such as ATP-binding cassette transporter A1 (ABCA1) and ATP-binding cassette transporter G1. After efflux to HDL, cholesterol may be esterified in the plasma by the enzyme lecithin–cholesterol acyltransferase and is ultimately transported from HDL to the liver, either directly via the scavenger receptor BI or after transfer to Apo-B-containing lipoproteins by CETP. From the liver, cholesterol is excreted in the bile and ultimately the feces. 28 Available research in animal studies regarding the consequences of CETP activity for the atheroprotective RCT pathway has provided ambiguous data, as both elevation and inhibition of CETP activity can be favorable. 29 In addition, in a study in dyslipidemic hamsters, it was shown that CETP inhibition alone did not stimulate RCT and that additional effects mediated by the LDL-lowering drug berberine were required to upregulate this process. 30 This observation raises the possibility that CETP inhibition cannot independently decrease atherosclerosis dramatically but its combined effect with other lipid-modifying drugs may be impactful. In contrast, however, another study showed that in statin-treated male patients with coronary artery disease (CAD), a genetic variation conferring low CETP levels was associated with increased 10-year mortality. This suggests that the efficacy of statin therapy to reduce cardiovascular risk depends on CETP genotype and associated CETP plasma levels. This effect may need consideration when administering CETP inhibition to patients with CAD. 31
Furthermore, it has become evident that the HDL particle number, rather than the HDL-C concentration per se, is of greater importance for the prediction of cardiovascular risk. 32 This may provide another possible explanation for the lack of benefit of CETP inhibition in CAD, because torcetrapib reportedly raised HDL-P by only 1% despite a 53% increase in HDL-C and dalcetrapib reportedly raised HDL-P by only 9.3% despite a 29.1% increase in HDL-C.4,33,34 In addition, there is evidence that small, dense HDL particles exhibit more potent antioxidant, anti-inflammatory, cytoprotective, and anti-infectious activities and promote more potently cholesterol efflux from lipid-loaded macrophages compared with larger HDL particles.4,35,36 In contrast, very large HDL particles, such as the ones associated with CETP deficiency, may have a lesser antiatherogenic potential.4,37 This is supported by the results of an earlier study, where marked hyperalphalipoproteinemia caused by CETP deficiency, secondary to a CETP gene mutation, was not associated with longevity. 38 Actually, in a very recent study, it was shown that cholesterol-overloaded HDL particles are independently associated with the progression of carotid atherosclerosis in a cardiovascular disease-free population. 39
Finally, some experts feel that CETP inhibition may be potentially harmful, as there are studies showing that the incidence of cardiovascular disease was inversely related to plasma CETP, and certain alleles of the CETP gene that lower hepatic CETP secretion have been found to be associated with an increased risk of myocardial infarction. 40
Future of CETP Inhibition
Despite the past failures, newer CETP inhibitors devoid of off-target hyperaldosteronism and with more dramatic HDL-raising and LDL-lowering effects are being studied with the hope that these new agents may actually reduce cardiovascular risk.
Anacetrapib is a CETP inhibitor studied in the “Determining the Efficacy and Tolerability of CETP INhibition with AnacEtrapib” (DEFINE) trial. This was a 76-week randomized, double-blind, placebo-controlled study designed to assess the safety, tolerability, and efficacy of anacetrapib, 100 mg daily, versus placebo, when added to ongoing lipid therapies in patients with CHD or at high risk for CHD (Framingham Risk score of >20% per 10 years). 41 In the anacetrapib group, as compared with placebo, there was a 138.1% increase in HDL-C levels and a 39.8% reduction in LDL-C levels. In addition, anacetrapib, as compared with placebo, increased Apo-A1 levels by 44.7% and decreased Apo-B levels by 21.0%. Furthermore, treatment with anacetrapib was associated with a 31.7% reduction in non-HDL cholesterol, a 36.4% reduction in lipoprotein(a) levels, and a 6.8% reduction in triglyceride levels, beyond the changes seen in the placebo group. 41 There were no appreciable differences between the anacetrapib group and the placebo group in the percentage of patients with adverse events that were thought to be related to the study drug or that led to its discontinuation. There were also no significant differences between the two groups in the mean change in systolic or diastolic blood pressure or in the percentage of patients with a reported increase in blood pressure. Moreover, there were no significant between-group differences in the serum levels of potassium, chloride, bicarbonate, or aldosterone, thus proving that anacetrapib was devoid of off-target hyperaldosteronism. 41 A two-year extension to the DEFINE trial showed that an additional two years of treatment with anacetrapib was well tolerated with durable lipid-modifying effects on HDL-C and LDL-C. 42 Of note, anacetrapib has been shown to increase Apo-B clearance in mildly hypercholesterolemic subjects and this effect may also be responsible for the observed anacetrapib-induced LDL-C lowering. 43 In an animal model, anacetrapib has been shown to dose-dependently reduce atherosclerosis and improve lesion stability. 44
The effects of anacetrapib on cardiovascular outcomes are currently being evaluated in the ongoing “Evaluation of the Effects of Anacetrapib through Lipid modification” (REVEAL) trial (ClinicalTrials.gov Identifier: NCT01252953) [www.clinicaltrials.gov/ct2/show/NCT01252953]. This is a phase III trial designed to determine whether treatment with anacetrapib could reduce the risk of a composite end point (coronary death, myocardial infarction, or coronary revascularization) in patients with circulatory problems who have their LDL-C optimally treated with a statin. It has randomized 30,624 subjects to anacetrapib 100 mg daily or matching placebo with a predicted median follow-up of four years. The study will include men and women ≥50 years of age with a history of myocardial infarction, cerebrovascular atherosclerotic disease, peripheral arterial disease, or diabetes mellitus with other evidence of symptomatic CHD. The results of this trial are expected to be released in 2017.
Evacetrapib is a novel, potent, and selective CETP inhibitor, which has been shown to elevate HDL-C without inducing aldosterone or increasing blood pressure. 45 As monotherapy, evacetrapib produced dose-dependent increases in HDL-C from baseline of 53.6%-128.8% and decreases in LDL-C of 13.6%-35.9%. 46 In combination with statin therapy, evacetrapib, 100 mg daily, compared with statin monotherapy, produced increases in HDL-C of 78.5%-88.5% and decreases in LDL-C of 11.2%-13.9%. 46 In a meta-analysis of 14 randomized treatment arms over a mean of two months, evacetrapib significantly increased HDL-C by an average of 86% and reduced LDL-C by an average of 21.11% without any effect on the level of triglycerides. 47 Meta-regression suggested a dose-dependent effect of evacetrapib on HDL-C and LDL-C, but not triglyceride levels. This meta-analysis also suggested equivalent rates of adverse events in subjects receiving evacetrapib and placebo. 47 In a recent study, evacetrapib, alone or in combination with statins, was found to increase cholesterol efflux capacity (CEC), including the ABCA1-specific CEC, and also increase pre-beta-1 HDL. 48 These effects made evacetrapib a promising target for the potential reduction of cardiovascular risk, given the recent evidence that CEC has a strong inverse correlation with incident cardiovascular events, 49 although the hypothesis that a therapeutic increase of cholesterol efflux improves cardiovascular outcome remains to be proven in clinical studies. The process of the ABCA1-specific CEC is shown and described in Figure 2.
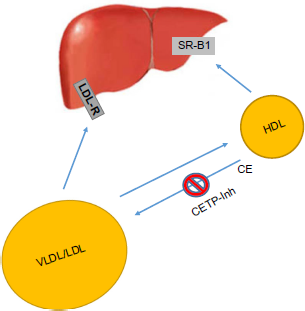
Cholesteryl ester transfer protein Inhibitors (CETP-Inh). CETP promotes the transfer of Cholesteryl Esters (CE) from HDL to VLDL and LDL. Therefore, CETP inhibition raises HDL-C levels and decreases LDL-C levels.
The LDL-lowering effects of evacetrapib were being evaluated in the multicenter “Addition of Evacetrapib to Atorvastatin Compared to Placebo, High Intensity Atorvastatin, and Atorvastatin With Ezetimibe to Evaluate LDL-C Lowering in Patients With Primary Hyperlipidemia” (ACCENTUATE) study (ClinicalTrials.gov Identifier: NCT02227784) [www.clinicaltrials.gov/ct2/show/NCT02227784]. This study had enrolled 396 hypercholesterolemic patients with atherosclerotic cardiovascular disease and/or diabetes mellitus, and its primary outcome measure was the percent change in LDL-C from baseline to three months. In addition, the effects of evacetrapib on cardiovascular outcomes were being evaluated in the “A Study of Evacetrapib in High-Risk Vascular Disease” (ACCELERATE) trial (ClinicalTrials.gov Identifier: NCT01687998) [www.clinicaltrials.gov/ct2/show/NCT01687998]. This was a trial designed to determine whether treatment with evacetrapib could reduce the risk of a composite end point (cardiovascular death, myocardial infarction, stroke, coronary revascularization, or hospitalization for unstable angina) in clinically stable patients with high-risk vascular disease (history of acute coronary syndrome, cerebrovascular atherosclerotic disease, peripheral arterial disease, or diabetes mellitus with documented CAD). The study had enrolled 12,095 patients and had a predicted median follow-up of four years. However, on October 12, 2015, Eli Lilly and Company and the ACCELERATE study's academic leadership have accepted the recommendation of the independent data monitoring committee to terminate the trial due to insufficient efficacy. Lilly discontinued the development of evacetrapib for the treatment of high-risk atherosclerotic cardiovascular disease and concluded all the other studies in the program. The study was not stopped for safety findings, but the independent data-monitoring committee based its recommendation on data from periodic data reviews, which suggested that there was a low probability that the study would achieve its primary end point based on results to date [https://investor.lilly.com/releasedetail.cfm?ReleaseID=936130].
More recently, another novel CETP inhibitor, TA-8995, was studied in a multicenter, randomized, phase 2, double-blind, placebo-controlled, parallel-group study (TULIP trial) in patients with mild dyslipidemia, as monotherapy and in combination with statin therapy. 50 Administration of TA-8995 caused a dose-dependent increase of HDL-C levels by up to 179.1% and of Apo-A1 levels by up to 63.4%, whereas it reduced the LDL-C levels by 45.3% and the Apo-B levels by 33.7%. In addition, the levels of lipoprotein(a) were reduced by up to 36.9%. In combination with statins, 10 mg of TA-8995 conferred an additional decrease of LDL-C by 39.8%-50.2%. Furthermore, treatment with the 10 mg dose of TA-8995 resulted in a 36.7% increase in serum-mediated cholesterol efflux. 50 In this study, there was no effect of TA-8995 (whether given as monotherapy or in combination with a statin) noted on any laboratory safety parameter, including serum aldosterone, salivary cortisol, high sensitivity CRP, or endothelin 1. In addition, there was no effect of TA-8995 on serum electrolyte concentrations, blood pressure, or insulin resistance. 50
Conclusion
The critical role of HDL in atheroprotection has been well established. CETP inhibitors comprise a new class of agents that significantly increase HDL-C and also have an LDL-lowering effect. However, the first trials with the CETP inhibitors torcetrapib and dalcetrapib failed to show a reduction in cardiovascular events, and another trial with the CETP inhibitor evacetrapib was recently stopped, because the independent data-monitoring committee suggested that there was a low probability that the study would achieve its primary end point. Nevertheless, newer CETP inhibitors with more favorable effects on lipids and devoid of any detrimental off-target characteristics, such as anacetrapib, are presently studied in ongoing clinical trials. The results of these outcome trials are expected to provide a final answer to the question whether CETP inhibition might actually be effective for the reduction of cardiovascular risk or the CETP inhibition chapter will need to come to an end.
Author Contributions
Conceived the concepts: CEK. Analyzed the data: CEK. Wrote the first draft of the manuscript: EDJ, CEK. Contributed to the writing of the manuscript: DR, TJV. Agreed with manuscript results and conclusions: CEK, EDJ, DR, TJV. Jointly developed the structure and arguments for the paper: CEK. Made critical revisions and approved the final version: CEK. All the authors reviewed and approved the final manuscript.