
Abstract
Objectives
We studied the progression of coronary atherosclerosis over time as detected by multidetector computed tomography (MDCT) in relation to risk factors and plaque composition.
Background
Studies using MDCT are limited to the assessment of the degree of stenosis without taking into consideration the plaque composition that is seen by MDCT.
Methods
This study included 200 patients, complaining of chest pain and referred to do 64/128-contrast–enhanced MDCT for the second time, and both studies were retrieved and evaluated for the presence of plaque, plaque type, vessel wall remodeling, percent area, and diameter stenosis and compared in both studies. Plaque progression over time and its association with risk factors were determined.
Results
We included 200 patients, and 348 plaques were detected by 64/128 MDCT. The duration between follow-up and baseline studies was 25.9 ± 19.2 month. In all, 200 plaques showed progression (57.47%), 122 were stable (35.06%), and 26 regressed (7.47%). In longitudinal regression analysis, the presence of history of diabetes mellitus and dyslipidemia and the absence of intraplaque calcium deposits were independently associated with plaque progression over time (P < 0.0001).
Conclusion
Coronary plaque burden of patients with chest pain and no history of acute coronary syndrome significantly increased over time. Progression is dependent on plaque composition and cardiovascular risk factors. Larger studies and longer follow-up period are needed to confirm the determinant factors for plaque progression.
Introduction
According to the World Health Organization, cardiovascular disease is the number one cause of death. Globally more people die annually from cardiovascular disorders than from any other cause. 1 In particular, the Global Burden of Disease study classified ischemic heart disease as the leading cause of global mortality, accounting for 1.4 million deaths in the developed world and 5.7 million deaths in developing regions. 2
Assessment of the coronary plaque burden and disease progression added to the understanding of the natural history and pathophysiology of coronary artery disease (CAD) and is a surrogate end point for the evaluation of novel therapeutics.3,4
Invasive modalities such as intravascular ultrasound (IVUS) and serial selective quantitative coronary angiography (QCA) are considered gold standard methods to measure the progression of atherosclerotic plaque and stenosis over time. 5 However, these modalities are limited by their invasive nature and by the specific characteristics they are able to measure. 6
Multidetector computed tomography coronary angiography (MDCT) is a non invasive modality the can detect plaque composition and vessels wall changes as remodeling and provides actual plaque burden assessment.
Although a few serial studies with MDCT have been published,7,8 most prior analyses were confined to a small segment of the coronary tree or a specific subset of lesions (ie, noncalcified).
In the present study, our objective was to study the natural history of coronary atherosclerosis using 64/128 MDCT and to assess the serial changes in coronary plaque size, lumen dimensions, and arterial remodeling over an interval of time.
Methods
Patients
The study was conducted on 200 consecutive patients who underwent repeated coronary MDCT. This study complied with the principles of Helsinki. The first MDCT study could be retrieved retrospectively and reevaluated. Patients with a history of revascularization, intervention between the two studies, atrial fibrillation, or creatinine clearance <50 mL/min were excluded. All patients gave written informed consent, and the study protocol was approved by the institutional ethical committee.
History concerning the risk factors (diabetes mellitus [DM], hypertension, smoking, dyslipidemia, family history [FH]) and history of ACS (acute coronary syndrome) were noted.
Coronary MDCT Acquisition
Baseline and follow-up cardiac CT scans were performed using 64/128-slice MDCT (Toshiba Aquilion system) with the following parameters: gantry rotation time of 400 ms, slice thickness of 0.5 mm, helical retrospective gating and reconstruction interval of 1 mm. Patients were fasting for 4-6 hours. Oral beta-blockers were given to all patients with a heart rate more than 60 bpm, unless contraindicated. An intravenous (IV) nonionic contrast (lopamidol 370) (0.5-2.0 mL/kg, 80 mL maximum volume) was injected followed by a 10- to 30-mL saline flush at rates ranging from 1.5 to 2.5 mL/s. Image acquisition was performed with a 64-slice MDCT (Aquilion 64 Toshiba). First, a non–contrast-enhanced, prospectively electrocardiogram-triggered calcium score was performed at 75% of the R–R interval. The automatic bolus triggering technique was used for initiating image acquisition. An automatic raw data motion analysis tool was used to determine the optimal systolic and diastolic phases for reconstruction. Additional reconstructions at end systole (30% to 40% of the R–R interval) and mid-diastole (70% to 80% of the R–R interval) were routinely reconstructed. All phases were evaluated to identify the optimal phase for evaluation of each coronary artery.
Coronary MDCT Image Analysis
All data sets were transferred to an offline Vitrea 3D workstation for analysis using a semiautomated plaque analysis software. Two experienced observers blinded to the sequence of imaging evaluated the scans.
All three vessels were assessed in every patient, and all anatomically available segments were examined. The segments of poor quality due to stack, movement artifacts, or extreme calcification were excluded from analysis.
The following parameters were calculated per segment and per patient:
QCA-like parameters
Minimum lumen diameter (MLD) is the narrowest lumen diameter within each segment. Percent diameter stenosis (%DS) = [(reference diameter – MLD)/reference diameter] X 100.
IVUS-like parameters:
Percent atheroma volume = [(total vessel volume - total lumen volume)/total vessel volume)] X 100. Total atheroma volume (TAV) = total vessel volume - TAV. Percentage change in TAV = [(TAV follow-up – TAV baseline)/TAV baseline)] X 100. Minimum lumen area (MLA). Percent area stenosis (%AS) = [(reference lumen area – MLA)/reference lumen area] X 100.
Coronary remodeling
A change in vessel area from baseline to follow-up was calculated. Increase in vessel area was considered positive remodeling and decrease was considered negative remodeling. 9
Statistical analysis was done using IBM SPSS software package version 20, using chi-square test, F-test (analysis of variance), and Kruskal–Wallis test. Significant test results were quoted as two-tailed probabilities.
Results
Among the 200 patients, 170 patients (85%) were males and 30 patients (15%) were females with a mean age of 60.5 ± 7.8 years.
As for risk factors, 95 patients (47.5%) had DM, 155 patients (77.5%) had hypertension, 110 patients (55%) were current smokers, 130 patients (65%) were having a history of dyslipidemia, and 80 patients (40%) had a FH of CAD.
The mean duration between the baseline MDCT and the first follow-up was 25.9 ± 19.2 months ranging from 2 to 72 months.
A total of 348 plaques were detected, 200 atherosclerotic plaques (47.5%) had an increase in DS (change in %DS >10), 122 plaques (35.05%) had no change in %DS, and 26 plaques had a decrease in %DS.
A total of 205 plaques (58.9%) had an increase in AS (change in %AS >10), 118 plaques (33.9%) had no change in %AS, and 20 plaques (5.7%) had a decrease in %AS. Two hundred and thirty plaques (66.1%) had increased in TAV (% change in TAV >20), 40 plaques (11.5%) had no change in volume, and 78 plaques (22.4%) had decreased in volume.
To ensure the accuracy of change in plaque characters, we considered the change of the atherosclerotic plaque is significant if two of the three above characters (%DS, %AS, and% change in TAV) had increased, regressed, or did not change.
From the above criteria, we classified plaques as follows: 200 plaques (57.47%) had progressed, 122 plaques (35.06%) had no change, and 26 plaques (7.47%) regressed.
In our results, the most statistically significant risk factors associated with plaque progression were DM and presence of dyslipidemia. As seen in Table 1, from the total of 200 progressed plaques, 64.1% (128/200) were diabetics, while none of the regressed plaques were found in patients with DM (P > 0.001). Also we found that 65% (130/200) of progressed plaques were found in patients with dyslipidemia comparable to 20% (5/26) of regressed plaques (P = 0.012). The other risk factors did not reach statistically significant difference between the groups.
Comparison between the studied groups according to risk factors.

Statistically significant at P ≤ 0.05.
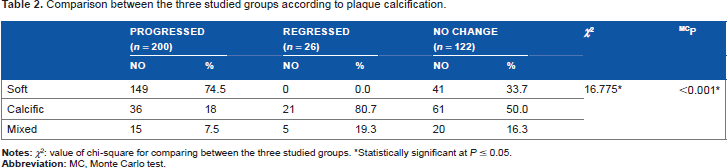
Of the 200 plaques that have progressed, 149 plaques (74.5%) were soft plaques, 36 plaques (18%) were calcific, and 15 plaques (7.5%) were mixed calcific plaques as seen in Table 2. Of the 122 stable plaques, 61 plaques (50%) were calcific plaques, 41 plaques (33.7%) were soft plaques, and 20 plaques (16.3%) were mixed calcific plaques.
Comparison between the three studied groups according to plaque calcification.
Statistically significant at P ≤ 0.05.
This proved the association between plaque stabilization and the presence of intraplaque calcium deposit and progression of the plaque in the absence of calcium (P = 0.001).
Of the 200 plaques that progressed, 16 plaques (8%) had no remodeling, 144 plaques (72%) had positive remodeling, and 40 plaques (20%) had negative remodeling. Of the 122 stable plaques, only 5 plaques (4.2%) had no remodeling, 66 plaques (54.1%) had negative remodeling, and 51 plaques (41.7%) had positive remodeling. Of the 26 plaques that regressed, 11 plaques (42.3%) had negative remodeling and 15 plaques (57.7%) had positive remodeling.
So, there was no significant association between vascular remodeling and plaque progression (P = 0.228) (as seen in Table 3).
Comparison between the three studied groups according to vascular remodeling.

Changes of Atherosclerotic Plaque over Time and its Association with Cardiovascular Risk Factors
In univariate longitudinal regression models, DM and the presence of dyslipidemia and absence of calcification were significantly associated with progression of any atherosclerotic plaque (Table 4 and Fig. 1). The duration of follow-up did not affect the progression or regression of the plaques significantly (Fig. 2).
Binary logistic regression for factors affecting plaque progression.

Statistically significant at P ≤ 0.05.
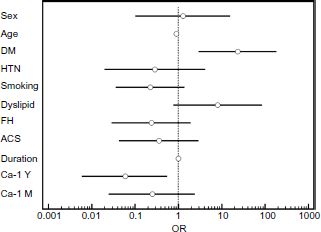
Predictors of plaque progression.

Relation of follow-up duration and atherosclerotic plaque changes.
Cases
Figures 3, 4 and 5 provide examples of progression and regression of coronary plaques detected by MDCT.

Patient No. 9, plaque No. 19: MDCT showing regression of proximal LAD soft nonobstructive plaque: (

Patient No. 21, plaque No. 127: MDCT showing stable LAD mixed obstructive plaque: (

Patient No. 21, plaque No. 128, 129: MDCT showing progression of proximal and distal RCA soft obstructive plaques: (
Discussion
Progressive atherosclerotic disease and its clinical sequel remain the number one cause of mortality in the United States. The majority of patients with ACS present with unstable angina, acute myocardial infarction, or sudden cardiac death secondary to sudden luminal thrombosis. 10
Until recently, the prevailing clinical perception of atherosclerosis was that of advancing luminal stenosis with less attention paid to the condition of the vessel wall.
In order to follow-up patients with CAD and assess the progression of atheromatous plaques, we need to use a noninvasive, feasibly repeatable method with low interobserver variability.
MDCT enables an accurate noninvasive identification and quantification of coronary plaques. The extent of coronary calcium is a surrogate marker for total plaque burden. However, there is a striking heterogeneity among human atherosclerotic lesions, and coronary plaques often consist of noncalcified tissue.10,11 Thus, even in coronary vessels without calcified plaques, severe atherosclerosis may be present. Hence, a more precise assessment of coronary atherosclerotic plaque burden and disease progression by noninvasive imaging tools that can detect and characterize calcified and noncalcified plaques can be expected to add important information, but it remains a challenge even by invasive methods.
We aimed to study the role of 64/128-MDCT using both QCA and IVUS-like parameters to assess plaque volume, composition, and degree of stenosis and see the changes of these parameters over time.
In this study, we did follow-up of 200 patients with chest pain but without ACS for 25.9 ± 19.2 months, using a semiquantitative assessment of coronary plaque burden. We found a significantly increased TAV, %AS, and %DS in 57.47% of plaques; regression in 7.4%; and stabilization in 35.06%.
Our results further indicate that there are differences in progression rate according to plaque composition as we found no significant progression for calcified plaque while noncalcified plaque progressed significantly over time (χ2 = 16.775, P < 0.0001). Progression of plaque was significantly associated with the presence of cardiovascular risk factors in adjusted analysis as DM and dyslipidemia.
Previous papers have shown that MDCT is comparable to QCA angiography regarding lumen stenosis assessment9,12; but QCA is a lumenography lacking the detection of the vessel wall changes, remodeling, and plaque characterization. Similarly, IVUS and MDCT comparative studies8,10 have shown that the MDCT can reasonably evaluate atherosclerotic plaque size, remodeling, eccentricity, and composition, despite the acknowledged limitations of the technique. Voros et al. 13 suggested that quantitative MDCT angiography could be acceptably used in population-based approaches, given the small mean differences between MDCT and IVUS measurements.
Most prior IVUS studies comparable with MDCT demonstrated lesions in the proximal segments of the three main vessels with high accuracy, but they were not able to study the distal and branching vessels by both techniques and comparing the plaque site and composition due to the invasive nature and long procedure of IVUS study.
Butler et al. 14 revealed that the extent and nature of overall CAD, defined as the cumulative stenotic and nonstenotic, calcified and noncalcified atherosclerosis burden, are underestimated by invasive coronary angiography and more accurately quantified with IVUS. MDCT is inferior to IVUS but may constitute an attractive noninvasive alternative to assess overall CAD burden. 15
Plaque Characterization
In our study, there was an association between plaque stabilization with the presence of calcium deposits in the plaque and plaque progression with the absence of calcium (P = 0.001). Of the 200 progressed plaques, 74.5% were soft noncalcific plaques and 50% of the stable plaques were calcific plaques.
In the analysis by Lehman et al. 16 , 69 patients were included who presented with acute chest pain to the emergency department but initially showed no evidence of acute coronary syndromes. All patients underwent contrast-enhanced 64-slice CT at baseline and after 2 years. There was significant progression in the mean number of cross-sections containing any plaque (16.5 ± 25.3 vs. 18.6 ± 25.5, P = 0.01) and noncalcified plaque (3.1 ± 5.8 vs. 4.4 ± 7.0, P = 0.04) but not calcified plaque (13.3 ± 23.1 vs. 14.2 ± 22.0, P = 0.2).
So, soft plaques were more liable for progression and vulnerability, and calcified plaques tend to be more stable.
The study by Schmid et al. 17 was conducted to measure the change in noncalcified coronary plaque volume in the left main coronary artery and in the proximal left anterior descending coronary artery over time using 64-slice MDCT. Fifty patients in whom noncalcified lesions had been detected on baseline MDCT received follow-up scans after an interval of 17 ± 6 months. They found that there is a significant increase of the amount of noncalcified plaque, which was observed over a mean interval of 17 months.
In our study, the most statistically significant (P = 0.001) risk factor associated with plaque progression is DM and dyslipidemia.
Wong et al. 18 revealed that individuals with metabolic syndrome (MetS) and DM have a greater incidence and absolute progression of coronary artery calcium (CAC) compared with individuals without these conditions, with progression also predicting coronary heart disease events in those with MetS and DM. 19
This study sought to examine and compare the incidence and progression of CAC among persons with MetS and DM versus those with neither condition. The MESA (Multiethnic Study of Atherosclerosis) included 6,814 African American, Asian, Caucasian, and Hispanic adults, free of cardiovascular disease at baseline. Relative to those with neither MetS nor DM, adjusted relative risks (95% confidence intervals [CI]) for incident CAC were 1.7 (95% CI: 1.4-2.0), 1.9 (95% CI: 1.4-2.4), and 1.8 (95% CI: 1.4-2.2) (all P < 0.01), and absolute differences in mean progression (volume score) were 7.8 (95% CI: 4.0-11.6; P < 0.01), 11.6 (95% CI: 2.7-20.5; P < 0.05), and 22.6 (95% CI: 17.2-27.9; P < 0.01) for those with MetS without DM, DM without MetS, and both DM and MetS, respectively. Similar findings were seen in an analysis using Agatston calcium score. In addition, progression predicted coronary heart disease events in those with MetS without DM (adjusted hazard ratio: 4.1, 95% CI: 2.0-8.5, P < 0.01) and DM (adjusted hazard ratio: 4.9 [95% CI: 1.3-18.4], P < 0.05) among those in the highest tertile of CAC increase versus no increase.
So in both studies, DM is definitely, especially if uncontrolled, associated with atherosclerotic plaque progression.
In our study, dyslipidemia is the second statistically significant (P = 0.012) risk factor. Of a total of 200 plaques that progressed, 130 patients (65%) were dyslipidemic patients.
Hoffmann et al. 19 found that the effect of statin treatment on noncalcified plaques was significant after adjusting for LDL levels and cardiac risk factors.20,21
This study supports ours, as with dyslipidemia and uncontrolled blood levels, LDL is strongly associated with plaque progression, and controlling of blood levels of LDL with statins is associated with atherosclerotic plaque stabilization.
Study Limitations
The relatively small number of patients studied was the main limitation in this study. Selection bias was another limitation, as the inclusion of the patients was based on the clinicians' opinion without clear preset recommendations. Repeating this study at a wider scale might yield different results.
In addition, this being a retrospective study made us unable to take detailed history about the medications, blood pressure, and dyslipidemic and diabetic control.
Conclusion
Coronary plaque burden of patients with acute chest pain significantly increases over time and the progression is dependent on plaque composition, especially for soft noncalcified plaque when compared to calcified plaque. Progression is further associated with cardiovascular risk profile at baseline. Larger studies are needed to confirm these results and to determine whether the MDCT can be used for noninvasive monitoring and follow-up of coronary atherosclerosis in high-risk patients.
Author Contributions
Designed the study: SME, MAS. Analyzed the data: EMS. Wrote the first draft: SWA. Contributed to writing: RL. Arranged the paper: EMS. Made critical revisions: EMS. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgment
This research was originally conducted and presented for the Master of Cardiology thesis of Reem H. Laymouna, under the supervision of Mohamed A. Sobhy, Salah M. ElTahan and Sherif W. Ayad, at Alexandria University.