
Abstract
Coronary artery disease (CAD) is recognized as an inflammatory disease. In the present study, we investigated the effect of green tea consumption on plasma inflammatory markers and the association between green tea consumption and CAD. In 22 healthy volunteers, green tea consumption (7 cups/day) significantly decreased serum malondialdehyde-modified low-density lipoprotein (MDA-LDL) concentrations, whereas green tea consumption tended to decrease plasma C-reactive protein and interleukin (IL)-6 concentrations. In 725 patients undergoing coronary angiography, the percentage of patients drinking <1 cup/day of green tea was higher in patients with myocardial infarction (MI) than in CAD patients without MI and patients without CAD (29% vs. 15% and 18%,
Introduction
Inflammation has been recognized to play an important role in both the initiation and progression of atherosclerotic diseases, such as coronary artery disease (CAD). 1 Several prospective studies2,3 demonstrated that plasma high-sensitivity C-reactive protein (hsCRP) levels, which are some of the markers of systemic inflammation, are powerful predictors of future myocardial infarction (MI) and cardiac death among apparently healthy individuals. The high hsCRP levels were also reported to be associated with an increased risk of further coronary events in patients with CAD. 4 We previously reported plasma hsCRP levels to be associated with the presence and extent of coronary stenosis in patients with stable CAD. 5 Moreover, we showed that plasma hsCRP levels correlated with the severity of both coronary and aortic atherosclerosis using magnetic resonance imaging (MRI). 6
Low-density lipoprotein (LDL) oxidation plays a key role in the development of atherosclerosis. 7 Several enzyme-linked immunosorbent assay (ELISA) methods had been developed to measure oxidatively modified LDL levels in blood.8,9 Elevated levels of malondialdehyde-modified LDL (MDA-LDL), an oxidized LDL, have been reported in patients with CAD, especially in those with MI.8,9
The intake of dietary antioxidants such as polyphenols is a potential therapy to prevent LDL oxidation and atherosclerosis progression. Polyphenols are mainly found in fruits, vegetables, and beverages. In Japan, green tea, which is very rich in catechins, is the most popular beverage and the major source of polyphenol intake (>80% of polyphenol intake).10,11 We previously reported that the daily consumption of green tea decreased serum MDA-LDL concentrations in 22 healthy Japanese male volunteers.
12
Using animal models, green tea was also shown to have anti-inflammatory effect in addition to the inhibitory effect against LDL oxidation.13–15 However, anti-inflammatory effect of green tea has not yet been elucidated
Methods
Study Design and Subjects
The study design was reported previously. 12 Briefly, the study consisted of a one-week run-in period, a two-week water intake period, and then a subsequent two-week green tea intake period with 22 healthy Japanese male volunteers. Over the course of the study, we asked all study subjects to maintain their regular dietary habits but not to consume any kind of tea, wine, citrus liquor, or vitamin supplements. After the run-in period, all subjects consumed seven cups/day of water for two weeks (water period) and then consumed seven cups/day of green tea for the next two weeks (green tea period). During the water or green tea periods, they drank four cups (breakfast and lunch, two cups each) and three cups (dinner) of water or green tea after each meal (a total of seven cups/day comprising 700 mL). The green tea used in our study was a commercially available freeze-dried tea, sarasara ryokucha (Itoen Co.), which is on sale for drinking in Japan. One stick (0.9 g) of the freeze-dried tea can be dissolved in 100 mL of hot water and then be drunk as one cup of green tea. As a result, seven cups of green tea contain 542.5 mg of catechins. At the end of each period, subjects fasted overnight and blood samples were taken at 9:00 am on the next morning. Plasma hsCRP concentrations were measured using a BN II nephelometer (Dade Behring), and plasma interleukin (IL)-6 concentrations were measured by ELISA with a human IL-6 immunoassay kit (BioSource International). Plasma LDL-cholesterol concentrations were measured by the direct enzymatic method with a commercially available kit (Cholestest LDL, Daiichi Pure Chemicals), and serum MDA-LDL concentrations were measured by ELISA, as reported previously.12,17 Plasma epigallocatechin gallate (EGCg), gallocatechin gallate (GCg), and epicatechin gallate (ECg) concentrations were measured by the high-performance liquid chromatography with electrochemical detection. 12 Total catechins concentration was defined as the sum of EGCg, GCg, and ECg values.
Study Patients
The study protocol was reported previously. 16 We investigated the intake of green tea, other beverages, and antioxidant foods in 725 consecutive Japanese patients who underwent coronary angiography for suspected CAD at the National Defense Medical College Hospital. CAD was defined as at least one coronary artery having >50% luminal diameter stenosis on angiograms. MI was confirmed by the documentation of coronary artery stenosis plus either elevation of cardiac enzymes or diagnostic electrocardiogram changes. The results were compared with clinical and angiographic data. After admission, the intakes of antioxidant beverages and foods were evaluated by questionnaires. Regarding antioxidant beverages, questions regarding the intakes of green tea, coffee, black tea, cocoa, and wine were asked, and each was determined by three categories (<1 cup/day, 1-3 cups/day, and >3 cups/day). Antioxidant foods common in Japan were divided into three groups (soybeans products, green/yellow vegetables, and fruits). The intakes of these antioxidant foods were determined by three categories (<3 times/week, 3-4 times/week, and >4 times/week).
Our two studies were approved by the Institutional Ethics Committee of the National Defense Medical College Hospital. Our studies complied with the principles of the Declaration of Helsinki. All study subjects and patients provided informed consent prior to participating in the studies.
Statistical Analysis
Regarding the data of 22 healthy volunteers, to test whether or not the distributions of variables are deviating from a normal distribution, the
Regarding the data in 725 patients undergoing coronary angiography, any differences between two groups were evaluated by the unpaired
Results
Green tea intake and inflammatory markers
Of the 22 study subjects, 20 had been in the habit of drinking green tea before the study. As reported previously,
12
plasma total catechin concentrations significantly decreased at the end of the water period and then increased at the end of the green tea period (Table 1). Although there was no change in LDL-cholesterol concentrations, serum MDA-LDL concentrations (84 ± 45 vs. 76 ± 40 IU/L,
Plasma catechins, hsCRP, and IL-6 concentrations at the end of each period in 22 healthy subjects.

Green tea intake and CAD
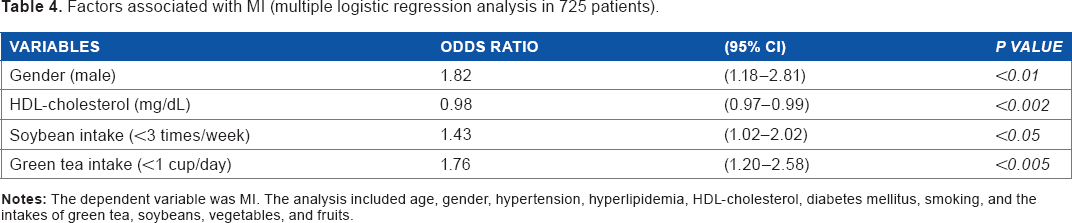
Of the 725 study patients, 517 (71%) were found to have CAD on coronary angiograms, of whom 225 (43%) had MI. Clinical characteristics of study patients are shown in Table 2. Compared with patients without CAD, CAD patients with and without MI were predominantly male and had lower HDL-cholesterol levels and higher rates of diabetes mellitus and smoking. With regard to the intake of antioxidant foods, there were no significant differences between patients without CAD and CAD patients with or without MI (Table 3). However, the percentages of patients with <3 times/week intake of soybeans and fruits were significantly higher in CAD patients with MI than in those without MI (38% and 41% vs. 26% and 32%,
Clinical characteristics in patients with and without CAD.

Intakes of antioxidant beverages and foods in patients with and without CAD.

Factors associated with MI (multiple logistic regression analysis in 725 patients).
Discussion
As shown in our previous report,
12
plasma catechin concentrations significantly increased with green tea consumption (seven cups/day). Although there was no change in plasma LDL-cholesterol concentrations, green tea consumption significantly decreased serum MDA-LDL concentrations and the ratio of MDL-LDL/LDL-cholesterol, thus suggesting that green tea has an inhibitory effect against LDL oxidation
We previously reported that green tea consumption was inversely associated with MI in 393 Japanese patients undergoing coronary angiography. 16 The present study extended our previous report by increasing the number of study patients (from 393 to 725 patients) to elucidate the associations between antioxidant beverages and foods, and CAD. In line with our previous report, 16 we confirmed that green tea consumption was inversely associated with MI in 725 patients. A recent meta-analysis including our data from 393 patients indicated that routine green tea consumption was significantly associated with a decreased risk (17%) of CAD. 19 In hypercholesterolemic rabbits, green tea ingestion was reported to reduce aortic atherosclerosis, whereas the ingestion of black tea or vitamin E did not, suggesting the stronger anti-atherogenic effect of green tea than those of black tea or vitamin E. 20 In our present study, the consumption of soybeans products was also associated with MI, but this association showed only borderline significance. Therefore, our results suggest that green tea consumption is more likely to play a major role in the prevention of CAD, especially MI, in Japanese patients than other antioxidant beverages and foods.
Our study has some limitations. First, one of our study limitations is the small number of study subjects (22 healthy subjects). Moreover, our study had no control group without green tea period, and our study was a sequential but not crossover design, thereby making it impossible to separate period effects from treatment effects. To clarify the results of our study, a further study should be done using a crossover design in a larger number of study subjects. Regarding the association between green tea consumption and CAD, our study is cross-sectional. Such a study cannot establish causality. It only shows some association and is hypothesis generating. Therefore, a prospective study is required to elucidate the preventative effect of green tea on CAD and MI.
Conclusion
Green tea consumption was found to be inversely associated with MI in Japanese patients. Green tea consumption significantly decreased serum oxidized LDL concentrations, but green tea consumption tended to decrease inflammatory markers; thus, suggesting the protective effect of green tea against atherosclerosis is more likely to be because of the inhibitory effect of LDL oxidation than because of anti-inflammatory effect.
Author Contributions
Conceived and designed the experiments: RO, YM. Analyzed the data: YM. Wrote the first draft of the manuscript: RO. Contributed to the writing of the manuscript: YM, KK. Made critical revisions and approved the final version: RO, YM, KK. Agreed with the manuscript results and conclusions: RO, YM, KK. All authors reviewed and approved the final manuscript.