
Abstract
Background
Blood pressure (BP) control in hypertensives is important in preventing cardiovascular (CV) morbidity and mortality. This work was done to assess control of BP among Nigerian hypertensives at rest and during exercise.
Materials and Methods
A total of 85 male hypertensives were recruited consecutively and had clinical evaluation and treadmill (TM) exercise testing using the Bruce protocol. Independent t-test, chi-square, and Fisher's exact tests were used to compare patients with controlled and uncontrolled BP using SPSS version 16 software. Adjustment for confounders was by logistic regression and general linear model.
Results
Resting systolic BP (rSBP) (mmHg) and resting diastolic BP (rDBP) (mmHg) were significantly lower in the controlled group (115.0 ± 12.29, 133.1 ± 12.27, P = < 0.001 and 76.00 ± 6.55, 91.4 ± 8.00, P = < 0.001). The proportion of subjects with controlled BP was 37.7%. Adjusted peak SBP (PSBP) during exercise (mmHg) was significantly higher in the uncontrolled than in the controlled group (210.5 ± 27.31, 191.8 ± 20.77, P = 0.001). Adjusted exaggerated blood pressure response (EBPR) was found in 37 subjects (44%) in the uncontrolled group while seven subjects (0.1%) had EBPR in the controlled group (P = 0.003).
Conclusion
This study shows that EBPR is significantly higher in subjects with uncontrolled BP compared with those with controlled BP. Therefore, good BP control may be the key factor in preventing EBPR in hypertensives.
Introduction
Hypertension is a global cause of cardiovascular (CV) morbidity and mortality. Trie burden of this disease is particularly heavy in the sub-Saharan part of Africa because of ignorance, poverty, inadequate healthcare, and erosion of traditional lifestyles. 1 Apart from increasing prevalence of high blood pressure (BP) in this part of the world, BP control is also a challenge as BP control has been documented to be comparably low at 5-10%.1,2 This challenge appears to be due to poverty, 3 lack of proper education of patients, 4 proliferation of untested alternative treatments, poly-pharmacy, and having to take medications for long periods of time for an apparently benign condition. 1 The efficacy of BP treatment or control is traditionally assessed at rest and in certain cases; the advent of ambulatory BP monitoring has allowed BP control to be assessed on the go. 5 It has been suggested that end-organ damage progresses despite control of resting BP.6–8 This may be related to the level of BP control and the BP response that is generated as individuals go about their routine daily activities. Kokkinos et al. 9 in 2009 suggested that exercise BP reflects the BP during routine daily activities. Abnormal BP response like exaggerated blood pressure response (EBPR) during routine daily activities may therefore lead to target end-organ damage with consequent CV morbidity and mortality. The hypothesis for this work is that abnormal BP response like EBPR is dependent on the level of BP control. To assess this, this study looked at BP at rest and during exercise in essential hypertensives with or without adequate BP control.
Subjects and Methods
This study is a cross-sectional study. Eighty-five male subjects with essential hypertension were consecutively recruited at the outpatient clinic of the cardiac care unit of Obafemi Awolowo University Teaching Hospitals Complex (OAUTHC), Ile-Ife, Osun State, Nigeria. They were evaluated clinically with history taking and physical examination, 12-lead resting ECG, transthoracic echocardiography, and treadmill (TM) exercise testing.
We included adult males and females above 18 years with the diagnosis of essential hypertension. Subjects with heart failure, severe hypertension (BP ≥ 180/110), 10 secondary hypertension, diabetes mellitus (DM), contraindications to exercise testing, trained athletes, and conditions that may impair exercise testing were excluded from this study.
Subjects were exercised on the TM (Schiller CS-200, Switzerland) using the Bruce protocol. They exercised until exercise was completed or until an indication for exercise termination was met.11,12 BP was measured using a mercury sphygmomanometer (Accuson, Kris-Alloy, England) in the upright position and heart rate (HR) displayed on the digital HR meter was used for the study. The HR and BP were recorded at rest and during the last 30 seconds of each stage of exercise.
TM walking was demonstrated to subjects and was practiced prior to testing. The exercise laboratory and equipment conformed to the standard specifications for exercise testing 12 and emergency care facilities and medications were on hand.
Controlled BP was defined as baseline BP < 140/90 mmHg and Uncontrolled BP as baseline BP > 140/90 mmHg according to the guidelines of the Eight Report of the Joint National Committee (JNC 8) on prevention, detection, evaluation, and treatment of high BP. 13 EBPR was taken as SBP ≥ 210 mmHg. 14 BP was measured by the same individual for all subjects using the same calibrated mercury sphygmo-manometer (Accuson, Kris-Alloy, England). Subjects were seated comfortably with the arm supported at the level of the heart for five minutes before BP was taken. Appropriate cuff sizes were used.
Ethical clearance for the study was obtained from the Ethics and Research committee of the hospital, and subjects gave informed consent. Subjects’ confidentiality was ensured by the use of study identification serial numbers to replace their names.
Data Analysis
Data was analyzed using the SPSS version 16 software. Categorical variables were expressed as proportions and percentages, while continuous variables were expressed as means ± standard deviation or as ranges. Independent t-test was used to compare the means of the two BP control groups, while chi-square test was used for test of association. Where the expected value in any of the cells is < 5, Fisher's exact test was used. Logistic regression and multivariate general linear model were used to adjust for confounders. P < 0.05 was taken as statistically significant.
Results
Table 1 describes the characteristics of the two groups in the study population. Thirty-two of the subjects had controlled BP amounting to 37.7% of the total. The age (P = 0.064) and body mass index (BMI) (P = 0.515) in the subjects were similar in those with controlled BP and uncontrolled BP but duration of hypertension (DOH) was significantly higher in those with controlled BP (P < 0.001). The resting systolic BP (rSBP) and resting diastolic BP (rDBP) were significantly lower (P < 0.001) in subjects with controlled BP (115.0 ± 12.29 mmHg and 76.00 ± 6.55 mmHg) compared with subjects with uncontrolled BP (133.1 ± 12.27 mmHg and 91.4 ± 8.00 mmHg).
Descriptive characteristics of the study population.
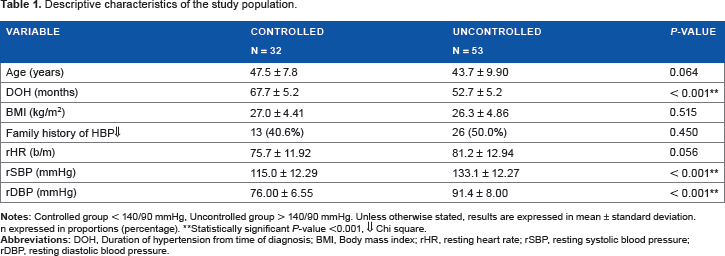
Statistically significant P-value < 0.001, ⇓ Chi square.
The pattern of antihypertensive medication use is shown in Table 2. Commonly used antihypertensive medications were moduretic, angiotensin converting enzyme inhibitors (ACEI), and calcium channel blockers (CCB). No difference was found in antihypertensive medication use except in beta-blockers (BB), which was more in the uncontrolled group compared to controlled group (P < 0.001).
Pattern of antihypertensive use.

Statistically significant P-value <0.001, ⇓ Fisher's exact test.
In Table 3, CV responses by the two groups to maximum TM testing are shown. Both groups exercised for the same duration (8.0 ± 1.30 minutes in the controlled and 8.4 ± 1.51 minutes in the uncontrolled, P = 0.208). The PSBP and rate pressure product (RPP) were significantly lower (P = 0.001 and P = 0.009) in the controlled BP group (191.8 ± 20.77 mmHg and 288.2 ± 54.00 mmHg bpm x 10−2) compared with the uncontrolled BP group (210.5 ± 27.31 mmHg and 326.1 ± 68.72 mmHg bpm x 10−2). Both remained significantly lower in the controlled group after adjusting for DOH (P = 0.001 and P = 0.03). There was a significant crude (P < 0.001) and adjusted (for DOH) difference (P = 0.003) in the EBPR, with higher EBPR in the uncontrolled BP group (44%) than in the controlled group (0.1%).
Cardiovascular responses during exercise in controlled anc uncontrolled BP groups.

Statistically significant P-value < 0.05,
Statistically significant P-value < 0.001. μAdjusted P-value (multivariate general linear model), μμLogistic regression.
Discussion
The percentage of BP control in this study is low at 37.7%. This is similar to low percentage or prevalence that have been previously reported in the literature.1,2,15 Also, rSBP and DBP were significantly lower in the controlled BP group despite similar age, BMI, and antihypertensive medications (with the exception of BB) in the two groups. Documented predictors of BP control in the literature include poverty, 16 low education, 17 lower age, BMI, DM, antihypertensive medications used, and adherence to and persistence with antihypertensive treatment plan.18–22 In this work, age, BMI, and the commonly used antihypertensive medications showed no effect on BP control. It is probable that adherence to antihypertensive treatment plan is one of the factors influencing BP control in this group of subjects, but this was not evaluated in this study. There is a need for more concerted and integrated public health and physician driven measures to combat major and peculiar reasons for this low prevalence, namely poverty 16 and low education. 17 This is because people who are poor and ignorant are less likely to be aware that they are hypertensive and may be unable to procure medications to treat the disease, thereby affecting compliance.
Commonly used antihypertensive medications in this study were diuretics, CCBs, and ACEIs. This is in keeping with the recommendations of the JNC 8 committee on prevention, detection, evaluation, and treatment of high BP for blacks. 13 Adherence to these recommendations by physicians in the sub-Sahara Africa is encouraging as it shows that efforts can now be concentrated on other causes of failure of BP control, particularly adherence to antihypertensive plan by patients. This appears to be a major challenge as a result of poverty, poor awareness, and education about hypertension in many low-income areas of sub-Saharan Africa.
Office or resting BP has been documented as an independent predictor of EBPR. 23 In this study, EBPR adjusted for DOH was significantly lower in those with controlled BP or normal resting BP. Also, PSBP adjusted for DOH was found to be significantly lower in those with controlled BP. This suggests that the level of BP control may be an important independent factor contributing to EBPR as documented in the literature. 23 Other factors that predict EBPR include QT dispersion, DM, and increased age. 24 In this study, age was not different for the two BP control groups while subjects with DM were excluded and QT dispersion was not assessed. It is likely, therefore, that adequate control of BP may completely eliminate the propensity toward EBPR in patients with essential hypertension.
The prevalence of EBPR adjusted for DOH in the uncontrolled group is 44%. This is similar to 45% prevalence in an earlier work in the same exercise laboratory. 25 Also, EBPR in the uncontrolled group is significantly higher than in the controlled group (0.1%). This suggests that the major determinant of EBPR in essential hypertension appears to be BP control. This high percentage in the uncontrolled group, therefore, calls for better BP control to stem CV morbidity and mortality. This can be achieved by prescription of antihy-pertensive medications according to guidelines, public health education about hypertension, and poverty alleviation. With the presence of EBPR in some of the patients with controlled BP, we suggest further work to look into factors predicting EBPR in those with apparently normal resting BP.
Conclusion
This study shows that good BP control may be important in preventing EBPR, which has been found to increase CV morbidity and mortality. A large scale study is needed to validate the findings of this study and to identify other predictors of EBPR in hypertensives with controlled and uncontrolled resting BP.
Limitation of Study
This is a predominantly male study because only few females volunteered for the study. Also, the sample size for this work is relatively small.
Author Contributions
Conceived and designed the experiments: OOA and MOB. Analyzed the data: OOA. Wrote the first draft of the manuscript: OOA. Contributed to the writing of the manuscript: OOA, MOB, RAA and AOA. Agree with manuscript results and conclusions: OOA, MOB, RAA and AOA. Jointly developed the structure and arguments for the paper: OOA, MOB, RAA and AOA. Made critical revisions and approved final version: OOA, MOB, RAA and AOA.