
Abstract
Background
Over a 12-month period, adolescent heart-screening programs were performed for identifying at-risk adolescents for sudden cardiac death (SCD) in our community. Novel to our study, all adolescents received an abbreviated, ultraportable echocardiography (UPE). In this report, we describe the use of UPE in this screening program.
Methods and Results
Four hundred thirty-two adolescents underwent cardiac screening with medical history questionnaire, physical examination, 12-lead electrocardiogram (ECG), and an abbreviated transthoracic echocardiographic examination. There were 11 abnormalities identified with uncertain/varying clinical risk significance. In this population, 75 adolescents had a murmur or high ECG voltage, of which only three had subsequent structural abnormalities on echocardiography that may pose risk. Conversely, UPE discovered four adolescents who had a cardiovascular structural abnormality that was not signaled by the 12-lead ECG, medical history questionnaire, and/or physical examination.
Conclusions
The utilization of ultraportable, handheld echocardiography is feasible in large-scale adolescent cardiovascular screening programs. UPE appears to be useful for finding additional structural abnormalities and for risk-stratifying abnormalities of uncertain potential of adolescents’ sudden death.
Introduction
Although sudden cardiac death (SCD) in young athletes is rare, it often occurs without warning and is a devastating event for families. Overwhelming support for screening as a public health initiative exists in both the medical and lay communities. 1 However, controversy surrounding the utility of screening programs for prevention of SCD in young people exists. 2 Most of this controversy centers on the cost versus benefit of screening programs and methods of screening.
Over the past several years, various centers have introduced 12-lead ECGs in adolescent screening programs. The use of 12-lead ECG screening has potential value in the detection of underlying lethal cardiovascular disorders. 3 On the other hand, 12-lead ECG abnormalities are common, and determination of physiologic versus pathologic findings is challenging. Although 12-lead ECG screening increases sensitivity, it has poor specificity and cost (both direct and resultant downstream from additional testing). 4 Often, early repolarization/high QRS voltage and other S—T segment abnormalities are present on 12-lead ECG and prompt further investigation with transthoracic echocardiography to stratify physiologic versus pathologic structural disorders.
Utilizing limited transthoracic echocardiography during screening events is one of the potential methods to increase specificity (and perhaps sensitivity) of screening and thereby reduces downstream cost and worry. There are new advances in existing ultrasound technology to miniaturize size, improve speed, and continue to improve the cost/benefit ratio of screening programs. The recent development of a handheld, ultraportable echocardiography (UPE) at a cost of less than $10,000 is one such example. The introduction of transthoracic echocardiography in adolescents screening programs will be controversial because in its limited form, it does not screen for all structural abnormalities. However, transthoracic echocardiogram (TTE) is expected to lower the traditional high number of false-positive findings, thus reducing subsequent unnecessary investigations. Despite the controversy, it is still important to develop, refine, and report new methods of screening.
The present report describes the implementation of miniaturized, handheld echocardiography technology in a series of adolescent screening programs designed to recognize features in adolescents who signify risk for SCD. The purpose of this study is to describe the utility of screening UPE in identifying cardiac structural abnormalities that pose risk for SCD in adolescents.
Methods
Between 11 January 2012 and 14 October 2012, four screening events were performed at various locations across Southeastern Michigan. All 432 adolescent participants received a screening protocol that utilized UPE by cardiologists trained in echocardiography. We report observational data acquired during these screening events as it pertains to the use of UPE.
All screening events were community events that occurred in 2012. These structured adolescent voluntary screening programs were held for adolescent athletes free of charge in Southeastern Michigan facilitated by Hurley Medical Center/Michigan State University, Flint, MI (HMC); Genesys Regional Medical Center/Michigan State University, Grand Blanc (GRMC); and William Beaumont Hospital/Oakland University School of Medicine, Royal Oak, MI (WBH). Data from these screening events were collected, deidentified, and analyzed. The Institutional Review Board of Genesys Regional Medical Center approved the present study, and the research was conducted in accordance with the principles of the Declaration of Helsinki.
Screening Event
Screening event durations were six to eight hours per day. They were held in conference centers, highschool gymnasiums, or athletic centers. The layout was designed around a series of stations, designed to maintain privacy yet maximize throughput. Stations included a check-in/out area, a parent-waiting area, a blood pressure station, and 18-20 ECG and physical examination stations. The physical examination and ECG stations were curtained rooms to maintain privacy of the adolescent while obtaining the ECG, the physical examination, and UPE.
Before the screening event, the adolescents with their parents filled out medical history questionnaires and consent forms. Screening forms were consistent with the 12-element AHA recommendations. 5 Adolescents then received blood pressure checks, and a 12-lead ECG was performed. After reviewing the ECG and medical history, physicians performed a limited physical examination and UPE.
When abnormal cardiovascular findings were detected, the information was disclosed to the adolescent and parents, and questions were answered. Following review of all data, adolescents were either cleared for sports without further evaluation, cleared for sports but needed further follow up, or instructed to cease physical activity until further evaluation by their physician. All information was provided to parents in hardcopy form for their records.
UPE protocol
Cardiologists performed a limited two-dimensional echocardiogram during the screening event. Three UPE machines were used (VScan, GE, USA) by three cardiologists experienced in using this equipment in routine clinical practice. All cardiologists who performed UPE were trained in echocardiography (two cardiologists were board-certified in echocardiography and one cardiologist was board eligible with 11 years of echocardiography experience) and interpreted the adolescents scans in real time. All images were recorded and stored on the device for later review and documentation. Abnormal results as discovered during the screening event were recorded and entered into the study database.
Standardized images included assessment of cardiac chambers with anatomy by standard two-dimensional imaging and color flow and valve dynamics by color flow. The aortic root was visualized and graded subjectively. The image protocol was developed by using patterns previously published3,4,6 and echocardiographic measurement normal standards for adolescents. Left ventricular wall thickness was measured in the long-axis parasternal view at end diastole and LV thickness above 1.3 cm was considered abnormal and consistent with hypertrophy. Heavy trabeculations and deep intertrabecular recesses in the ventricular myocardium were considered abnormal when the ratio of non-trabeculated to trabeculated myocardium was > 2.0 in multiple echocardiographic views of the LV endocardium during end-diastole and when present adolescents labeled as left ventricular noncompaction (LVNC). Other imaging was performed at the discretion of the cardiologist who was performing the study. During the data entry phase, all adolescent echocardiographic images were downloaded and reanalyzed (by a noninvasive cardiologist with Level II board certification in echocardiography) using imaging software (Vscan Gateway Software, version 1.1.0.14).
Data collection and analysis
All screening questionnaires, ECGs, echocardiograms, and screening results were reviewed, recorded, and data were entered in a study database. Frequency of abnormal pathology and method of detection were recorded. Continuous variables are expressed as mean ± standard deviation or counts with proportions as appropriate. Statistical analysis was performed with SPSS software, version 16.0, Chicago, IL, USA.
Results
Four hundred thirty-two adolescents underwent the screening program and received UPE. Of these 53.2% (N = 230) were male. The mean age of participant was 16.3 ± 1.7 years. The majority of participants were Caucasian (84.2%); while African-Americans (6.4%), Hispanic (1.2%), and Asians/ other (0.6%) constituted the remaining ethnic background of this population.
Medical History Questionnaire
In this population, 49 adolescents (11.3%) reported a medical history of a heart murmur on a previous physical examination. Two adolescents (0.4%) had previously been advised to not participate in athletic competition. Eighty-nine adolescents (20.6%) reported experiencing chest pain/pressure, dizziness, or racing or “skipped beats” at rest or with exercise. Seventeen adolescents (3.9%) reported fainting or passing out during exercise or after having been startled. Twelve (2.7%) reported passing out after exercise or fainted. Seven adolescents (1.6%) had been told that they had high blood pressure, high cholesterol, or diabetes, while 32 (7.4%) had exercise-induced asthma. Only two adolescents (0.04%) admitted the usage of cocaine or anabolic steroids or smoking tobacco or non-tobacco substances. Twenty (4.6%) reported that someone in their family experienced sudden, unexpected death before the age of 45 years. Twenty-nine adolescents (6.7%) reported that someone in their immediate family with unexplained fainting or seizures. Only eight (1.8%) had a family member with a confirmed diagnosis of an “abnormally thickened heart, weakened heart, or Marfan's syndrome.”
Abnormal Findings
Eleven adolescents (N = 11/432 or 2.5%) had abnormal findings identified during the screening events and are described further in Table 2 and Figure 1. Eight of them (N = 8/432 or 1.8%) had an abnormal finding that was designated as being high clinical significance and resulted in a recommendation that the adolescent cessation of sports until further evaluation. Three (N = 3/432 or 0.7%) adolescents had bicuspid valves present which were assessed as having no clinical significance. One of the adolescents with a bicuspid valve had mild aortic insufficiency (AI). None of the adolescents with bicuspid valves had detectable aortic enlargement and none had known family history of valve problems. All the bicuspid valves were deemed incidental and these adolescents were not advised to stop playing sports; however, the presence of this valve finding was reported to the parents. (These findings and description of their identification are listed in Table 2 and the screening method of identification is demonstrated in Fig. 1.)

Identification of abnormalities from the screening program by screening modality and sequence of identification (N = 432).
Other abnormal findings were designated as being abnormal and required further evaluation but did not require immediate cessation of sports activity. This included 67 adolescents (15.5%) with abnormal blood pressure results. One hundred twelve adolescents (25.9%) had an abnormal medical history and 51 adolescents (11.8%) had an abnormal physical examination (excluding blood pressure and body mass index). Sixty adolescents had an abnormal ECG finding [N = 60/432 (13.8%)] and is given in Table 1.
List of abnormal 12-lead electrocardiography findings during the cardiovascular screening program (N = 432), of these 60/432 (13.8%) had an abnormal ECG * finding.
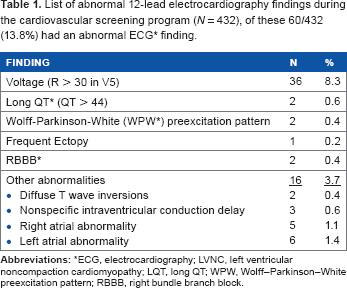
ECG, electrocardiography; LVNC, left ventricular noncompaction cardiomyopathy; LQT, long QT; WPW, Wolff-Parkinson-White preexcitation pattern; RBBB, right bundle branch block.
List of abnormal findings from the cardiovascular screening program and frequency of detection by screening modality (N = 11/432).

Abn., abnormality; BAV, bicuspid aortic valve; Al, aortic insufficiency; ECG, electrocardiography; LVNC, left ventricular noncompaction cardiomyopathy; LQT, long QT; WPW, Wolff-Parkinson-White preexcitation pattern; UPE, ultraportable echocardiography.
Deemed to not be of clinical significance.
Discussion
The presence of miniaturized, rapid ultraportable ultrasound technology is a major development in cardiovascular medicine (Fig. 2). There may be significant advantages in using this technology in adolescent screening programs with positive impact on sensitivity and specificity.3,4,6–9 This study describes the successful introduction of UPE in the workflow of an established adolescent cardiovascular screening protocol.

Example photographs of the UPE device (V-scan, GE, USA).
This study demonstrates that UPE finds additional structural abnormalities that have uncertain significance in an adolescent engaged in sports. The enhanced sensitivity and specificity provided by the ultrasound device could allow for the development of future risk stratification strategies. For example, in the 11 abnormalities discovered, 4 were discovered by UPE alone (normal ECG, physical examination, and medical history).
Findings of high QRS voltage on the 12-lead ECG were the most common electrocardiographic abnormality and auscultation of murmurs was the most common physical examination finding. These findings from our study are consistent with other studies from the medical literature.2,10–12 In the present study, 75 adolescents had a murmur on physical examination or high ECG voltage, of which only three were confirmed to have structural abnormalities on echocardiogra-phy that could pose risk.
Currently, the American College of Cardiology and American Heart Association limit screening to a physical examination and medical history, whereas the European Society of Cardiology and International Olympic Committee recommend using resting 12-lead ECG to detect cardiac abnormalities.9,10 Previous literature has reported that adding ECG to medical history and physical examination improves the overall sensitivity of preparticipation cardiovascular screening in athletes. However, this strategy is associated with an increased rate of false-positive results typically from high QRS voltage that may signify presence of hypertrophic cardiomyopathy (HCM). 11
Currently, echocardiography is not recommended for initial screening but often becomes a primary tool for follow up of abnormalities that are discovered on initial screening.9,12 A primary factor of this is the cost associated with the echocardiography examination. The availability of UPE with instant interpretation in the hands of qualified providers during screening eliminates most of this issue. 2
In these screening events, there are logistical time challenges to perform echocardiography. Production of ultrasound equipment into simple ultraportable, handheld devices reduces cost and affords the ability to perform point-of-care ultrasound examinations. Cost is reduced by elimination of devoted ultrasound technicians, significant cost reduction in the ultrasound device itself ($8,000/handheld device versus > $100,000/ formal device), and reduced time with real time image acquisition, interpretation, and instant availability of information.
Another challenge with screening programs that utilize echocardiography is dealing with abnormal findings that do not cause sudden death but have uncertain future risk (eg, bicuspid aortic valves, LVNC). This problem, however, is not unique to echocardiography, and the establishment of protocols for guiding these individuals with these findings will need to be developed.
Interestingly, the most common abnormal morphologic finding from UPE in our adolescent population was features that were consistent with LVNC. On UPE, these adolescents had heavy trabeculations and deep intertrabecular recesses in the ventricular myocardium that likely fit established criterion. 13 Our finding corresponds with recent reports that describe that phenotypes of LVNC are likely much more common than previously reported. In recent reports, phenotypic variants of LVNC have been reported to be present in upward of 1 in 500 individuals.14,15 The presence of LVNC in an adolescent and risk of sudden death with physical activity are virtually unreported in the current medical literature. Arrhythmias, thromboembolism, heart failure, and death are the reported consequences; however, frequencies of these events in individuals who have no clinical symptoms are unknown. One small study of 15 subjects with LVNC reported a high rate of ventricular tachycardia (27%) during 24 hour ambulatory ECG monitoring.13,14 At the present, there are no guidelines for exercise prescriptions or restrictions for LVNC in the literature. 14
In our population, one adolescent was diagnosed with a bicuspid valve with mild-to-moderate AI, another was found to have moderate Ebstein's anomaly, and others were found to have preexication pattern on 12-lead ECG. Although these might not confer immediate risk of SCD, early recognition may alter the future disease trajectory and provide benefit.16,17
UPE likely improves the specificity of adolescent screening programs that utilize 12-lead ECG; however, it is uncertain if it improves sensitivity. A large, prospective study is needed; however, several logistical issues arise. Most adolescent screening research has focused on identification of HCM. HCM is present in (1/500) and the rate of SCD in adolescents from HCM is approximately 0.3/100,000/year.18 In addition, several congenital disease states have uncertain risk or unknown risk (ie, LVNC). On the other hand, several benefits to screening program are not directly apparent as well. For instance, direct cardiovascular imaging with UPE likely provides a significant added degree of adolescent and parental satisfaction for the adolescent is deemed to be normal following the screening. Finally, this program provides additional direct interaction with adolescents and physicians (and other healthcare providers) in which counseling, education, and awareness of a multitude of other cardiovascular risk factors (weight, blood pressure, and social behaviors) are brought to light and may provide a behavioral change that may have significant future impact on that particular individual.
Limitations
The implementation of preparticipation screening programs designed to detect young athletes at risk has generated considerable debate. Contentious issues center on cost effectiveness, inability to predict all causes of SCD, and the added cost burden of downstream consultation resulting from false-positive results. Our study was not designed to address these questions and future studies are needed to elucidate answers to these questions. Furthermore, our data lack the statistical power and methodologic design to derive inferences regarding the core purpose of the program; mainly the effectiveness of screening on the prevention of sudden death in athletes.
This study shares the inherent limitations of registry data including the presence of selection bias and confounding factors. Patient variables (ie, medical and social history) were derived from patient questionnaires and may be subject to bias. Our study utilized experienced cardiologists performing UPE who provided instant interpretation with a priori knowledge of the medical history, physical examination, and ECG findings. Therefore, our study results may not be applicable to other physicians or healthcare providers who do not have this training.
Conclusion
The utilization of ultraportable, handheld echocardiography is feasible in large-scale adolescent cardiovascular screening programs. UPE appears to be useful for finding additional structural abnormalities and for risk stratifying abnormalities of uncertain potential for adolescent sudden death. Future studies that examine the additive benefit of this technology are needed.
Author Contributions
Conceived and designed the experiments: TEV, JEW, KB, ME, SA, DH. Analyzed the data: TEV, JEW, SR. Wrote the first draft of the manuscript: TEV. Contributed to the writing of the manuscript: TEV, JEW, ME, KB, SR, AO, FT, KF, MS, SA, DH. Agree with manuscript results and conclusions: TEV, JEW, ME, KB, SR, AO, FT, KF, MS, SA, DH. Jointly developed the structure and arguments for the paper: TEV, JEW, ME, KB, SR, AO, FT, KF, MS, SA, DH. Made critical revisions and approved final version: TEV. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
All the screening events in this study utilized patterns, individuals, expertise, equipment, and other resources provided at no cost by the Cardiovascular Department of William Beaumont Hospital/Oakland University School of Medicine, Royal Oak, MI. The screening programs were a collaborative effort between various physicians, healthcare workers, and other key individuals from these institutions and various other volunteers. In addition, key individuals include Adam DeJong, Lara Davis, Rheanon McDonald, Deborah Moresevan, Kimberly Barber PhD, MD, Monique Brand, Aaron Berman MD, Nancy Cutler MD, Justin Trivax MD, Scott Bonzheim, and Simon Dixon MD.