
Abstract
Cardiogenic shock remains a challenging disease entity and is associated with significant morbidity and mortality. Temporary mechanical circulatory support (MCS) can be implemented in an acute setting to stabilize acutely ill patients with cardiomyopathy in a variety of clinical situations. Currently, several options exist for temporary MCS. We review the indications, contraindications, clinical applications, and evidences for a variety of temporary circulatory support options, including the intra-aortic balloon pump (IABP), extracorporeal membrane oxygenation (ECMO), CentriMag blood pump, and percutaneous ventricular assist devices (pVADs), specifically the TandemHeart and Impella.
Introduction
With advancements in the management of coronary artery disease, arrhythmias, and congenital heart disease, in addition to the development of predisposing comorbidities, more and more patients are surviving heart failure (HF). There are an estimated 825,000 new diagnoses of HF in a year, and 5.1 million adult Americans suffer from the disease. 1 Though there has been a significant reduction in mortality from HF because of beta blockers, ACE-inhibitors, and automatic implantable cardioverter defibrillators, 2 many patients still present with cardiogenic shock. This remains a challenge for the practitioner and is associated with significant morbidity and mortality.
Over the last several decades, temporary mechanical circulatory support (MCS) devices have been an effective means of acute support in patients with cardiogenic shock or in the setting of high-risk interventions such as revascularization or ablation.3–6 There has been significant technologic development in the field of circulatory support, with options including intraaortic balloon pump (IABP), extracorporeal membrane oxygenation (ECMO), CentriMag® pump, and several percutaneous ventricular assist devices (pVADs), such as the TandemHeart® and Impella® systems. When the method of temporary circulatory support is chosen and applied to the appropriate setting, these devices can effectively aid in bridging patients to hemodynamic stabilization or more definitive management. This review focuses on describing the hemodynamic goals, clinical indications, and various device options for current generation temporary MCS devices, in addition to highlighting ongoing research and future directions in the field.
Goals of Temporary MCS
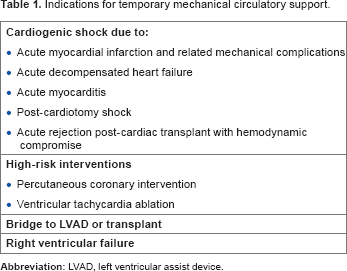
Indications for temporary mechanical circulatory support.
As MCS devices continue to develop, they must be practical in the real world of HF management. In addition to providing optimization of hemodynamics, these devices must have a desirable risk/benefit ratio with demonstrable safety and efficacy. Additionally, they should be feasible and economical, with relative ease of insertion and availability.
Circulatory Support Options
Intra-aortic balloon pump
The IABP was first developed on the hemodynamic basis of diastolic augmentation and counterpulsation. Kantrowitz and colleagues described the first published experience with an intra-aortic circulatory assist device in a case series of patients with cardiogenic shock in 1968. 3 A few years later, Scheidt and colleagues demonstrated improvement in hemodynamics, an increase in cardiac output by 500 mL/minute, and a decrease in lactate in 80 patients with cardiogenic shock. 7
Hemodynamic effects of mechanical circulatory support devices.

IABP placement initially developed as a surgical technique; however, it is now placed by interventional cardiologists in the cardiac catheterization laboratory and can be emergently placed at the bedside in an unstable patient. It is considered a safe and quick procedure in experienced hands. An alternative to the femoral approach, which requires patients to be immobilized, is axillary placement, which allows patients to be out of bed and is beneficial for prolonged use, such as in the bridge to transplant (BTT) setting. 8
Contraindications and complications associated with temporary circulatory support.

Relative contraindication.
Extracorporeal Membrane Oxygenation
ECMO involves use of a centrifugal pump to drive blood from the patient through an externalized membrane oxygenator system for carbon dioxide and oxygen exchange before returning to the patient's arterial system. Cannulation sites include femoral artery and vein (venoarterial, VA) or internal jugular vein/right atrium (RA) and common femoral vein (venovenous, VV) (Fig. 1). In addition to assisting in gas exchange, VA ECMO can augment cardiac output.
Aa schematic representation of peripheral VA (VA ECMO) and VV-ECMO. From Cove ME, MacLaren G. Clinical review: MCS for cardiogenic shock complicating acute myocardial infarction. 
Advantages of ECMO include the ability to oxygenate blood in hypoxemic states and unload both the right and left ventricles. Peripheral ECMO cannulas can be placed at the bedside in an emergency using a cut-down technique. The aim of ECMO is to provide acute, temporary support or serve as a bridge to more durable therapy. Complications include risk of limb ischemia, bleeding, and hemolysis. The American Heart Association Guidelines for Cardiopulmonary Resuscitation state that ECMO is reasonable to perform and its benefit outweighs risk in the setting of cardiac arrest or shock because of a potentially reversible condition, such as myocarditis. 11 Despite advancements in device technologies described below, ECMO has been shown to have comparable clinical outcomes when compared with percutaneously inserted ventricular assist devices (VADs). 12
CentriMag
The CentriMag® (Thoratec Corporation) is an extracorporeal, surgically implanted centrifugal pump that can provide up to 10 L/minute of blood flow. It is a third-generation continuous flow pump with a magnetically suspended rotor, which has minimal friction, thus reducing shear force on red blood cells with less hemolysis. The CentriMag system is currently Food and Drug Administration (FDA) approved for LV support up to six hours. It is approved for support when there is acute right ventricular (RV) failure for up to 30 days (Humanitarian Use Device), and longer term use is currently investigational only.
13
The CentriMag system can provide left and/or RV support with placement of outflow (22 Fr) and inflow (32 Fr) cannulas in the left atrium (LA)/Ao or RA/pulmonary artery (PA), respectively (Fig. 2). The pump can also be used peripherally in an ECMO circuit.
(
In a multicenter study of 38 patients supported by the CentriMag for various indications and a combination of left, right, or biventricular support, the device provided effective short-term support with a 47% 30-day mortality rate and low complication rate. The most common complications were infection, bleeding, and thromboembolic neurologic events (though three of four of these events were questionably related to device). 14 Contraindications include bleeding that precludes the use of heparin for anticoagulation during device support.
Percutaneous ventricular assist devices
TandemHeart
The TandemHeart System® (CardiacAssist, Inc.) is a LA to femoral artery bypass system (Fig. 1). This pVAD consists of a 21F venous transseptal inflow cannula, a continuous flow centrifugal blood pump with an electromagnetically suspended and driven impeller, and an arterial perfusion catheter. Oxygenated blood is withdrawn from the LA; which is accessed by standard transseptal technique involving placement of the 21F cannula, which contains 14 side holes and a large end hole; and pumped to the systemic circulation via a 17F femoral artery catheter, thereby bypassing the left heart. Patients should undergo an aortogram with runoff to assess the degree of peripheral vascular disease prior to catheter insertion. RV support can be achieved by placing the inflow cannula in the RA and outflow cannula in the PA. The TandemHeart pump can also be surgically implanted similar to the CentriMag described above to support either or both ventricles.
Thiele and colleagues first described the use of the TandemHeart in 18 patients with AMI complicated by cardiogenic shock. The device was implanted for a mean of 4 ± 3 days, and the use resulted in a significant improvement in cardiac index (from 1.7 L/minute/m2 to 2.4 L/minute/m2), increase in mean arterial pressure (from 63 to 80 mmHg), and decrease in filling pressures. In all, 30-day mortality was reported to be 44%. 15 The TandemHeart gained FDA approval in 2003.
Hemodynamically, the TandemHeart significantly reduces preload and augments cardiac output, with the ability to pump up to 4 L/minute. It has been shown to have superior effects on hemodynamics than the IABP.16,17 Of note, the device is preload dependent, with an ideal pulmonary capillary wedge pressure maintained between 18 and 20 mmHg. 18 Once the pump is started, pulmonary capillary wedge pressure should be monitored to ensure adequate filling and pump flow. Additionally, there is high risk of thromboembolism necessitating the need for systemic anticoagulation with heparin.
Contraindications include ventricular septal defect (which would then cause right to left shunting and hypoxemia), aortic insufficiency, severe peripheral vascular disease, and inability to be on systemic anticoagulation. The TandemHeart has several possible complications, and percutaneous placement requires an experienced operator familiar with the technique of transseptal puncture. Complications include distal limb ischemia, bleeding, infection, tamponade because of perforation at the time of transseptal puncture, thromboembolism, and air embolism at the time of insertion of large cannulae.19,20
Impella System
The Impella® 2.5 system (Abiomed) is a 9-Fr catheter-mounted, 2.5 L/minute, impeller-driven, axial-flow pump that is placed in a retrograde fashion across the aortic valve via a cardiac catheterization procedure (Fig. 3). The pigtail-tipped catheter sits in the left ventricle and pumps blood out to the ascending Ao. It received FDA approval in 2008. The 5.0 L/minute Impella® 5.0 or Impella® LD (both FDA approved in 2009) is larger and requires surgical cut down of the femoral or axillary artery or an open heart procedure, respectively. These devices can be inserted for short-term support, typically up to five days.
19
An illustration of options for MCS: (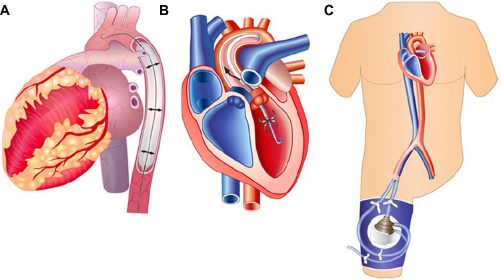
The Impella requires systemic anticoagulation. Complications include bleeding, vascular injury, infection, and hemolysis. Another concern is pump migration if the catheter becomes dislodged in any way. Contraindications include LV thrombus, moderate aortic stenosis or aortic insufficiency, recent stroke or TIA, and structural abnormalities of the Ao. 19
Total artificial heart (TAH)
The TAH is a complete cardiac replacement strategy, first successfully implanted in 1982. 21 The only current FDA-approved device in the United States as a BTT is the SynCardia temporary TAH (SynCardia Systems, Inc). It may be used for destination therapy under the Humanitarian Use Device designation in the United States. It consists of a 70-cc pneumatically driven pump with tilting disk valves and short outflow grafts replacing both ventricles, the proximal Ao and PA, and the four valves. A left ventricle is connected to the LA via a left atrial inflow connector and to the Ao via an outflow cannula. A right ventricle is connected to the RA via a right atrial inflow connector and to the PA via an outflow cannula. The ventricular drivelines tunnel through the chest wall and connect to the external console. Size requirements include a body surface area ≥1.7 m2 and chest AP diameter ≥10 cm.22,23 Additionally, there is a smaller, 50 cc, TAH in development for patients with a body surface area of 1.2-1.79 m2, which may help overcome the primary size contraindication for placement. In a single-center experience of 101 patients using SynCardia TAH as a BTT, mean support time was 87 days with 68.3% survival rate. Major adverse events were stroke (7.9%) and reoperation because of hemorrhage (24.7%). 23 The Freedom® portable driver, a wearable system that runs the SynCardia TAH and allows discharge to home, was recently FDA approved on June 26, 2014.
Clinical Indications for Temporary MCS
Cardiogenic shock because of AMI
Ischemic heart disease continues to be the most common cause of HF, and cardiogenic shock is still a frequent complication of AMI. In fact, most early studies of cardiogenic shock were performed in patients with AMI, and the majority of data regarding the use of MCS are still in this setting.
With its favorable hemodynamic effects of decreased afterload and increased coronary perfusion, it is not surprising that the American College of Cardiology and American Heart Association (ACC/AHA) initially deemed that there was enough evidence that IABP placement should be performed when managing cardiogenic shock in the setting of ST-elevation myocardial infarction (STEMI). However, much of these data were based on registries, with poor level of evidence, and the newest guidelines have actually changed the recommendation for IABP as well as other LV assist devices to
Sjauw and colleagues published a recent two-part meta-analysis of IABP utilization in STEMI.
25
The first included seven randomized trials encompassing a total of 1009 STEMI patients. In this population, IABP did not show any benefit for 30-day survival. The second looked specifically at studies of STEMI patients with cardiogenic shock and IABP. They divided the studies based on treatment: thrombolysis versus primary percutaneous coronary intervention (PCI). Though patients receiving thrombolytics and IABP placement had an 18% decrease in 30-day mortality (
In an attempt to address the lack of data on utility of IABP in shock with AMI, the IABP-SHOCK II investigation randomized 600 patients expected to undergo early revascularization (PCI or coronary artery bypass grafting) in a prospective, open-label, multicenter trial to IABP or no IABP.
27
The primary endpoint of 30-day mortality was met in 39.7% of patients in the IABP group and 41.3% of patients without IABP (
In a head-to-head randomized comparison between the TandemHeart and IABP in patients undergoing primary PCI, hemodynamics were significantly improved in the pVAD group; however, there were more complications with similar 30-day mortality rates (though the study was not powered for mortality). Of note, in this study, a high percentage of patients received thrombolytics and there was no screening aortogram/aortoiliac runoff prior to placement of either device. 16 Another study in patients with mostly myocardial infarction (MI)-related cardiogenic shock confirmed the hemodynamic benefit of the TandemHeart, though a lack of survival benefit, when compared with IABP. 17
Given the high mortality in patients with STEMI complicated by shock, continued attention has been focused at unloading the left ventricle and improving hemodynamics and survival in this patient population. With mixed data from IABP trials and the risks associated with the placement of the TandemHeart, focus was shifted to the Impella 2.5. The use of the Impella 2.5 has also improved outcomes in patients with shock in the setting of acute ischemia, especially when initiated early, ie, prior to revascularization. 29 The EUROSHOCK Registry was a retrospective study of 120 patients with cardiogenic shock because of AMI undergoing implantation of Impella 2.5. There was a decrease in lactate levels at 48 hours suggesting improved organ perfusion, but 30-day mortality remained high at 64.2%. 4 Patients who received Impella 2.5 support prior to primary PCI in the setting of AMI and cardiogenic shock, rather than after PCI, fared better. 30 The Impella 2.5 has also shown beneficial LV remodeling and unloading in anterior STEMI patients without cardiogenic shock. 31
When compared with the IABP, the Impella 2.5 more substantially improves hemodynamics though no randomized trials have been powered for a primary endpoint of mortality. 32 The most recent RE-COVER II trial, which also aimed to compare the Impella 2.5 with the IABP, was terminated because of incomplete enrollment. 33
Cardiogenic shock complicating AMI remains the leading cause for need of LV support. Though pVADs have shown an improvement in hemodynamics, further larger, randomized studies are necessary to demonstrate a clear mortality benefit.
High-risk PCI in the setting of cardiomyopathy
pVAD has an additional role in ischemic heart disease as an adjunct to high-risk PCI in the setting of severe LV dysfunction and/or cardiogenic shock. ECMO-assisted primary PCI in the setting of cardiogenic shock complicating AMI has been shown to improve survival.34,35 The IABP has been used for years to provide mechanical support in high-risk interventional settings; however, as outlined above, it provides only modest improvement in hemodynamics and cannot provide actual circulatory support.
Both the TandemHeart and Impella 2.5 can be used at the time of high-risk PCI, with periprocedural insertion and removal in the cardiac catheterization lab. Aragon and colleagues published their early results using the Tandem-Heart in a small (
The subsequent and larger prospective, randomized controlled trial, PROTECT II, compared periprocedural support using the Impella 2.5 versus IABP in 452 patients with systolic HF (mean ejection fraction [EF] 24%) undergoing high-risk PCI. After 69% of expected enrollment, the trial was stopped early because of futility. Though support with the Impella 2.5 provided a superior hemodynamic profile, there was no significant difference in the primary endpoint of 30-day major adverse cardiovascular events (MACE). However, at 90 days, the non-significant difference between the two groups’ 30-day MACE rate did trend toward a wider difference (40.6% versus 49.3%,
Ventricular Tachycardia
Ventricular tachycardia (VT) frequently accompanies end-stage cardiomyopathy and can lead to significant hemodynamic instability. Medical management and defibrillator therapy alone may not be enough to control VT; therefore, catheter ablation strategies are now more frequently pursued, especially when involving infarct-related scar. However, induction of VT during activation mapping can lead to further instability, and in this setting, substrate- and pace-mapping techniques can alternatively be used but may not be effective in eliminating VT. Though IABP support is indicated for decompensation in the setting of refractory arrhythmia, its optimal use can be challenging during VT. Percutaneous support devices can assist during arrhythmia induction by lending hemodynamic stability.
Friedman and colleagues first described the successful use of the TandemHeart in a single patient undergoing endocardial and epicardial VT ablation. 6 This has been shown to allow identification and ablation of a greater number of VT foci. 41 In this retrospective study, there was no difference in long-term outcomes between the TandemHeart-supported group and the substrate-mapped strategy group; however, the pVAD group may have been a sicker cohort to begin with since patients were not randomized.
The Impella 2.5 has also been successfully used during unstable VT ablation as described in case reports and a few small studies.42–44 Miller and colleagues retrospectively showed that the use of the Impella 2.5 allowed longer time in induced VT (66.7 versus 27.5 minutes;
Bridging refractory HF
Temporary MCS may be necessary to decide on more definitive therapy (bridge to decision, BTD) or to optimize patients prior to LVAD or transplant (bridge to bridge or BTT). Though patients requiring mechanical support do worse early on, if they survive to transplant, they do as well as their counterparts who did not require mechanical support. 45 Until recently, the only percutaneous option in this setting was IABP or ECMO; however, prolonged use is associated with complications (see Intra-Aortic Balloon Pump and Extracorporeal Membrane Oxygenation sections).46,47 Although more durable mechanical support may more effectively bridge a patient to definitive therapy, surgical placement may be too risky in a patient with acute cardiogenic shock, and percutaneously placed VADs may be more practical in this situation.48,49
Hemodynamic values before and after TandemHeart placement.

One of the most common nonischemic causes of acute HF that may require mechanical support as a bridge to recovery (BTR) is acute myocarditis. Though patients with acute, fulminant myocarditis have been shown to have better long-term outcomes than those with non-fulminant myocarditis, they often initially require temporary support if inotropes and IABP have failed.55,56 Several case reports and series have demonstrated the utility of pVAD insertion for this purpose.57–59 Chandra and colleagues described the first three patients with acute myocarditis who successfully recovered on the TandemHeart, with a mean duration of support of five days. 58 Khalife and Kar similarly described two patients with acute fulminant myocarditis who were successfully toward BTR using the TandemHeart. 59 When deciding on the mode of support (temporary versus more permanent) in patients with acute myocarditis, it is important to identify those who may require more durable support. Though a pVAD can be used as a bridge to a bridge (ie, to a durable LVAD), some patients, such as those with giant cell myocarditis, may benefit from more durable, or even biventricular, support from the outset as recovery times are longer and may entail waiting for heart transplantation. 56
Additionally, pVADs can be used in patients presenting with allograft rejection. IABP and ECMO are often used in this situation to stabilize patients while they are being treated for rejection; however, they may require longer-term support for recovery. Rajagopal and colleagues describe a patient who had biventricular pVAD support using the Impella 2.5 for the LV and the TandemHeart for refractory RV failure. 60 Both devices were successfully weaned and removed after adequate treatment of the patient's cardiac allograft rejection.
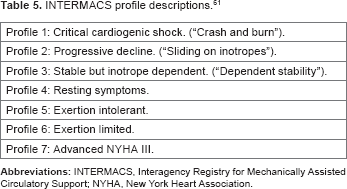
INTERMACS profile descriptions. 61
Postcardiotomy Shock
PCS is one of the leading causes of death after cardiac surgery, usually because of multiorgan failure. Approximately 0.2-6% of patients undergoing cardiac surgery develop PCS with survival to discharge ranging from 19.5% to 52.4%. 65 IABP and inotropic therapy alone may not suffice in patients who develop PCS when weaning off cardiopulmonary bypass (CPB). The use of ECMO, especially in patients with hypoxia or biventricular failure, is a common practice in this setting. Rastan and colleagues described 517 patients receiving ECMO support for PCS. The average duration of support was 3.28 days, and 74.1% of patients also had an IABP. In this cohort, 63.3% weaned successfully off ECMO; however, only 24.8% of all patients made it to hospital discharge. Cumulative survival was 17.6% at six months, 16.5% at one year, and 13.7% at five years. Unfortunately, these patients still have a high in-hospital mortality rate despite complete MCS. 66
Pitsis et al first described the use of the TandemHeart in two patients with postcardiotomy cardiac failure. 67 They then described a larger cohort of 11 patients who underwent TandemHeart support postcardiotomy, with the most common indication being failure to wean from CPB. The mean duration of support was 88 hours, and 72.2% of patients were successfully weaned off the pVAD. Survival to discharge was 54.54%. The major complication was pericardial bleeding. 68
The Impella also has been used in the postcardiotomy setting. Siegenthaler et al studied 24 patients with PCS undergoing Impella implantation (with or without IABP) and 198 patients who underwent IABP alone. The use of the Impella improved survival over IABP alone in patients with a residual cardiac output of 1 L/minute. 69 The CentriMag has also been demonstrated to be of more benefit when placed in patients in the operating room who have failed to wean from bypass rather than after decompensation in the intensive care unit postoperatively. 70 The CentriMag system has also been implanted with an ECMO configuration in 14 patients with PCS. Seven patients were successfully weaned, and six patients were discharged home. All of these patients remained on IABP support for at least five days after removal of the CentriMag system. 71
The Impella 5.0 was studied in the single-arm prospective feasibility study, RECOVER-1. A total of 16 patients underwent implantation for PCS. The primary safety endpoint of death or stroke at 30 days or discharge was noted in two patients (94% survived to 30 days, and of those, 93% were weaned off MCS). In all, 13 patients recovered their native cardiac function and were successfully weaned. The last patient required VAD implantation as a BTT. There were significant improvements in hemodynamic parameters, including mean arterial pressure and cardiac index. 72 In a larger retrospective review of 47 patients undergoing Impella implantation for acute cardiogenic shock, of those who had PCS (68% of patients), the one-year survival was 71.8%. 73 The Impella 5.0, which crosses the aortic valve, has been successfully placed in a patient with PCS after bioprosthetic aortic valve replacement. 74
Despite major technological advances, PCS remains a serious cause of mortality in patients undergoing cardiac surgery, with only about 25% of patients making it to hospital discharge. 75 Timely initiation of mechanical support, prior to complete loss of cardiac function, is imperative. Appropriate triage of these patients to centers skilled in the treatment of PCS and with the ability of offering advanced HF therapies is also of utmost importance in order to improve outcomes.
RV support
Preoperatively, RV function can be modified with pulmonary vasodilators, inotropes, and optimization of RV preload; however, in refractory situations, mechanical support may be necessary. The RV differs from the LV in that it usually recovers more rapidly. Therefore, temporary assist devices are preferred. If pulmonary dysfunction and oxygenation are issues, ECMO is the best option. Other strategies include the use of percutaneous right ventricular assist devices (pRVADs) such as the TandemHeart or CentriMag systems as previously described. 81
The use of the TandemHeart for RV support was first described by Giesler and colleagues in a 57-year-old female with RV infarction. 82 In a retrospective study of nine patients with primary RV failure, Kapur et al described significantly improved outcomes after insertion of a pRVAD. Patients underwent TandemHeart placement via right internal jugular-to-femoral or bifemoral cannulation to bypass blood from the RA to the main PA. The mean arterial pressure increased from 57 to 75 mmHg, right atrial pressure decreased from 22 to 15 mmHg, cardiac index increased from 1.5 to 2.3 L/minute/m2, mixed venous oxygen saturation increased from 40% to 58%, and RV stroke work increased from 3.4 to 9.7 g·m/beat. Four patients died during hospitalization, and those who survived had a shorter time to pRVAD implantation (0.9 days). 83 In the more recent, larger, multicenter THRIVE Registry, Kapur and colleagues found similar outcomes in 40 patients undergoing Tandem-Heart RV support. 84
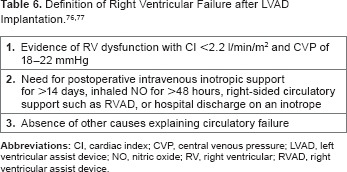
An RVAD may be temporarily placed in patients with RV failure after LVAD implantation. Takagaki et al have described successful conversion of a TandemHeart pLVAD to pRVAD after implantation of the HeartMate XVE LVAD. 85 Similarly, Anderson and O'Brien described the use of the Impella LP device during HeartMate II implantation. 86 The Impella RP (specifically designed for the right ventricle) can also be utilized for RV support and can deliver up to 4.8 L/minute. The inflow is in the inferior vena cava and the outflow in the PA, and the axial-flow pump is placed across the tricuspid and pulmonic valves in an antegrade fashion. This device is currently under investigation. It should be noted that there are no commercially available percutaneous devices, specifically for RV support, in the US.
Conclusion
Major technological advancements have enabled temporary MCS to take on a larger role in the treatment of HF over the last decade. Indications have broadened widely from its early uses. There are several considerations to keep in mind when deciding whether a patient is appropriate for temporary MCS. One must identify which device would suit him or her best, weighing the pros and cons of each method of support. Most patients requiring temporary support are acutely and critically ill, but an effort must be made to make decisions early when possible, ideally prior to a crash and burn (ie, INTERMACS 1 profile) situation. There must also be an exit strategy prior to insertion of temporary MCS, as its role is primarily for the short term as a BTR, permanent support, or transplantation.
Author Contributions
Conceived and designed the experiments: NAG, GRS. Analyzed the data: NAG, GRS. Wrote the first draft of the manuscript: NAG, GRS. Contributed to the writing of the manuscript: NAG, GRS. Agree with manuscript results and conclusions: NAG, GRS. Jointly developed the structure and arguments for the paper: NAG, GRS. Made critical revisions and approved final version: NAG, GRS. Both authors reviewed and approved of the final manuscript.