
Abstract
Purpose
The objective of this prospective study was to evaluate the effectiveness and safety of a percutaneous closure system based on a polyglycolic acid plug for achieving hemostasis.
Material and Methods
In this study from 2011 to 2014, a percutaneous vascular closure system (ExoSeal) was used in 1000 patients (mean age 70.6 ± 10.2 years), using antegrade and retrograde techniques within the context of an angiographic intervention. The system was used in conjunction with transfemoral approaches with a sheath size of 6F. Post the intervention (on the following day and after 6 weeks), follow-up was conducted clinically and using color-coded duplex ultrasound.
Results
Immediate hemostasis was achieved in 939/1000 patients (93.9%). In the remaining 61 cases, a correct positioning of the polyglycolic acid plug was not possible because of malfunctioning of the device, massive vascular wall calcifications, postoperative scar tissue, or too steep a puncture angle. In these cases, manual compression was successful. There was one retroperitoneal bleeding requiring transfusion. Minor complications were observed (7.4% in total) with 10 pseudoaneurysm (1%), 63 inguinal hematomas (up to 3 cm; 6.3%), and 1 stenosis (0.1%).
Conclusion
Safe and effective hemostasis is possible with the percutaneous ExoSeal closure system at puncture sizes of 6F.
Introduction
To improve patient safety and patient comfort, but also to prevent prolonged patient bed rest, closure systems after angiographic procedures have been established in interventional radiology, especially from a sheath size of 6F. 1
Since 2010, another closure system has been in use. This is based on a synthetic, bioabsorbable grafting system that closes outside the puncture site. The material of the extravascular grafting is polyglycolic acid, which is absorbed by hydrolysis over a period of up to 90 days. Approved for access paths via the femora l artery, the system can be implemented on standard short sheath. The system is commercially available in three sizes (5F, 6F, and 7F). As part of the “ECLIPSE study”, the closure system has proven to be beneficial in comparison with manual compression in terms of security and reduction in the time to mobilization. 2
In this prospective study, the efficacy and safety of the percutaneous closure system (ExoSeal) was evaluated after antegrade and retrograde puncture to obtain hemostasis in routine clinical practice. Patients gave their written, informed consent to participate in the study, which was conducted in accordance with the Declaration of Helsinki. Ethics committee approval was not required, as the research comprised investigation of a standard procedure.
Materials and Methods
Patients
In 1000 patients with peripheral arterial occlusive disease (PAOD) in stage 3-5 according to Rutherford, a percutaneous 6F closure system (ExcoSeal, Cordis Europe, Waterloo, Belgium) was used in the context of angiographic intervention.
We examined 580 male and 420 female patients with an average age of 70.6 ± 10.2 years (42-93 years). Of these, 640 (64%) patients had PAOD stage 3, 164 (16.4%) patients stage 4, and 196 (19.6%) patients stage 5.
Patient characteristics and preinterventional clinical details.

Results.

In case of anticoagulation with phenprocoumon, this was changed to heparin therapy and required a prothrombin time (Quick test) of at least 50%. The puncture was performed in 447 (44.7%) patients using the antegrade and 553 (55.3%) patients using the retrograde technique. In all cases, only the ventral vessel wall of the common femoral artery was punctured in the single-wall technique.
All patients received 5000 IU heparin peri-interventionally via the arterial access. In the absence of phenprocoumon as a long-term therapy, a medication with acetylsalicylic acid (ASA) 100 mg/day per os was applied. After realizing the closure, a light compression bandage was used in all patients, and bed rest for six hours was recommended. On the first day after the intervention, all patients were examined clinically and by color-coded duplex ultrasonography. Another clinical and sonographic follow-up was performed after 6 weeks; this was realized in 917/1000 (91.7%) patients.
Closure system (ExoSeal)
The preparation of the percutaneous closure system was carried out immediately after the vascular intervention under sterile conditions. Initially, a specific angiographic assessment of the common femoral artery was performed. After transluminal intervention, the closure system was introduced at an angle of ~45° located via the sheath. After positioning the intravascular system, a small wire loop was released by the user, which rested against the inside of the vessel wall. The correct intravascular position was determined by the pulsatile blood flow through a marker lumen. The required extravascular location of the closure was ensured by the intravascular position of a wire loop that was in communication with an extravascular visual indicator. After release of the plug, an immediate hemostasis was estimated (Fig. 1A–F). Occasionally, there was a slight oozing of blood in the access by injured subcutaneous arterial branches, which could be stopped by slight compression.
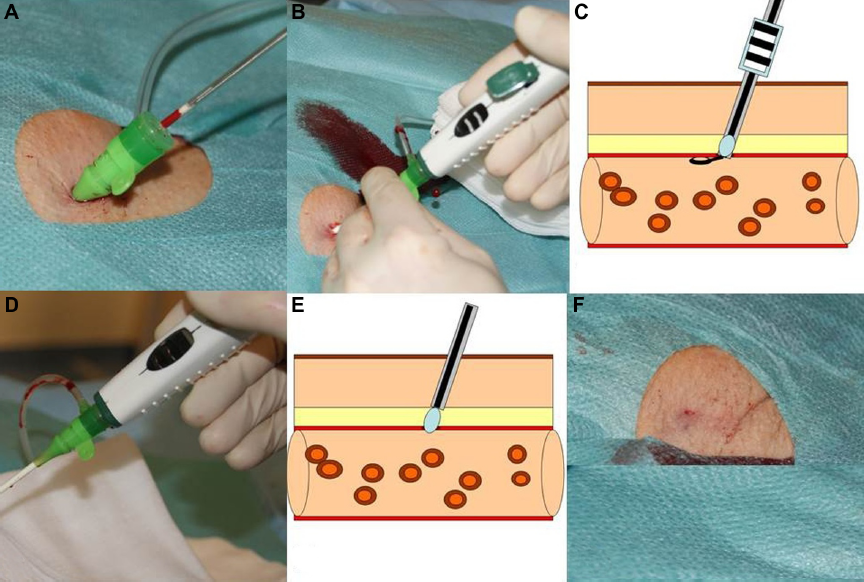
Procedure of the closure system. The systems can be introduced in a short 6F sheath (
Statistical Analysis
All values are expressed as means ± standard deviation or the number of patients and per cent. The calculation of the statistical significance level was performed using the chi- square test and was set at P < 0.05.
Results
After using the extravascular closure device, immediate hemostasis was achieved in 939/1000 patients (93.9%).
Primary hemostasis could not be achieved using the ExoSeal system in 61 cases (6.1%). In 15/61 cases, a technical problem arose. The system without triggering the plug had to be removed. The visual indicator showed the suboptimal location of the plug, so tripping was not possible. In the remaining 46/61 patients, hemostasis could not be achieved by the device. In these cases, significant vascular calcification (20/46), postoperative scarring (16/46), and a too steep a puncture angle (10/46), together with obesity, were seen.
In these cases, prolonged manual compression was utilized. In addition, a firm pressure bandage was applied for 12 hours.
In one case, a hemorrhage requiring transfusion resulted in a retroperitoneal space (major complication). In the follow-up, this patient was symptom-free.
A total of 74/1000 (7.4%) minor complications were observed: 10 (1%) pseudoaneurysms, 63 (6.3%) groin hematomas (up to a max. of 3 cm), and 1 stenosis (0.1%). The stenosis was detected by the partial intravascular position of the plug in color-coded duplex ultrasonography. In side comparison, there were no criteria for a hemodynamically significant stenosis.
Pseudoaneurysms, which were detected on the first postinterventional day by using color-coded duplex ultrasonography, were treated by ultrasound targeted compression in 3/10 cases and by selective thrombin injection in 7/10 cases.
The small groin hematomas described on the first postinterventional day reduced completely and could no longer be detected after 6 weeks. No statistically significant difference for the minor complications was observed with respect to the puncture technique (antegrade and retrograde).
Discussion
To achieve safe hemostasis, various closure systems have been developed. These systems are now used routinely in vascular interventional radiology. 1 Depending on the technique, three basic types can be distinguished: collagen-based (eg, Angioseal, Vasoseal, St. Jew Medical, St. Paul, Minnesota), Clip-based (eg, Star Close SE, Abbott Vascular, Redwood City, California), and suture-based (eg, Perclose/Proglide, Abbott Vascular). All these systems have to be evaluated with the “gold standard” of manual compression and have their clinical reliability proven in terms of the decrease in time to reach mobilization with increasing patient comfort.
Since 2010, there has been on the market a closure system that is based on synthetic, bioabsorbable grafting and closes the puncture site from the outside (ExoSeal). The ECLIPSE study evaluated the ExoSeal system in terms of patient safety and successful hemostasis. 2 Thus, a primary hemostasis resulted in 245/267 patients (91.8%). Similar to other closure systems, the primary success rate of >90% is possible. In our study, we reached primary hemostasis in 939/1000 cases (93.9%). Further advantages of our study – in addition to the large number of cases - are the evaluation in daily clinical routine as well as their use in antegrade and retrograde techniques.
The group of Schmelter et al. 3 , who studied the ExoSeal system in antegrade vascular punctures, was able to use the system successfully in 96/100 patients (96%). Even with repeated arterial punctures, the system was safe to use. Boschewitz et al. 4 , achieved primary hemostasis in 651/682 patients (95.5%) in spite of repeated access. In comparison with other systems, such as a percutaneous suture-mediated closure system (Perclose/Proglide), similar values were obtained. Immediate hemostasis could be achieved up to 95.6%. 5 Overall, the available closure systems are equivalent in terms of primary hemostasis.
The manufacturer's application recommendations describe no contraindications; however, demand for quality assurance certification by the user and special care in previously operated and heavily calcified arteries 6 are necessary. Only in rare cases a malfunction of the system has been noted. In our study, the system could not be applied successfully in 15 (1.5%) patients. Accordingly, the malfunction rates in other studies that evaluated the ExoSeal system are 0.4% and 3%.3,4 These values are similar to those while using other systems. The AngioSeal system malfunctioned rather frequently with 10% failures (12/120), 7 while in the Star Close system only 1% (13/1213) failure occurred. 8
According to the work of Mackrell et al. 9 , the patient in whom the placement of the closure system failed was treated with manual compression. The most common cause of the failure was the inability to introduce the system into the vessel, particularly in antegrade access routes, together with obesity. But this problem was also found in heavily calcified vessels and previous surgery. The clip-based closure system Star Close was used by Chiu et al. 10 in 142 cases. In 11/142 (7.7%) patients, the system could not be successfully placed, especially with the antegrade puncture technique. Wong et al. 2 described no major complications in the ECLIPSE study. In our evaluation, only one serious complication occurred, namely the formation of a postoperative hemorrhage requiring transfusion.
The groups to Schmelter et al. 3 and Boschewitz et al. 4 had no patients with major complications. After the application of a percutaneous suture closure system, in 0.4% (8/2103) serious complications occurred. 5 They consisted of deep infections and bleeding requiring transfusion. For the AngioSeal system, a major complication rate of 0%-1.1% was described.11–13 For the Star Close system, there were serious complications of up to 3.5%.8,14,15
In this study, the group of minor complications consisting of groin hematomas, pseudoaneurysms, and stenosis occurred. Overall, the sum of minor complications in this study was low at 7.4%. In the ECLIPSE study 2, in 9% cases minor complications were found. Minor complications after antegrade puncture technique and application of ExoSeal system were found in 7% of cases with four pseudoaneurysms and three minor rebleeding. 3 The group of Schmelter et al separated the occurrence of hematomas of minor complications: 10/100 (10%). Boschewitz et al. 4 found a small number of minor complications. There were a total of only 8/659 patients (1.2%) with small groin hematoma.
Steinkamp et al grouped groin hematoma of <5 cm into minor complications. 16 In our study, sonographically detected groin hematomas of maximum axial diameter up to 3 cm were found, and these were classified as minor complications. After percutaneous transfemoral access, postinterventional pseudoaneurysms were observed in 3%-9%. 17 According to Steinkamp et al. 16 , pseudoaneurysms that did not require surgical treatment were also classified as a minor complication and could be treated by a targeted ultrasound-guided compression or thrombin injection.18,19 A comparison with other closure systems shows similar rates of minor complications.
The AngioSeal system was associated with minor complication rates from 1.4% to 27.8%,12,20 while with a recirculation-clip-based system (Star Close) minor complications of 5.3%-22.5% were detected.8,10 For the percutaneous suture-mediated system (Perclose/Proglide) in pseudoaneurysms, groin hematoma and palpable groin suture-granuloma were described in 5% in a total of 15.6%. Granuloma or inflammatory reactions in the interventional access path were not found in our cases.
Summary
The percutaneous closure system (ExoSeal) is safe and effective in achieving hemostasis at puncture sizes of 6F after antegrade and retrograde techniques.
Author Contributions
Conceived and designed the experiments: PK, CW, TJ, JB, RA. Analyzed the data: PK, CW, FS, CWL, RA. Wrote the first draft of the manuscript: PK, CW, FS. Contributed to the writing of the manuscript: TJ, JB, CWL, RA. Agree with manuscript results and conclusions: PK, CW, TJ, JB, FS, CWL, RA. Jointly developed the structure and arguments for the paper: PK, CW, TJ, JB, FS, CWL, RA. Made critical revisions and approved final version: PK, CW, TJ, JB, FS, CWL, RA. All authors reviewed and approved of the final manuscript.