
Abstract
Background
Endomyocardial fibrosis (EMF) is a restrictive cardiomyopathy, the prevalence of which is declining globally. This study was carried out to determine if there were changing patterns in its local prevalence in South-West Nigeria.
Methods
We reviewed the medical records of all patients admitted to or attending the cardiology clinic or medical outpatient/specialty clinics in the Department of Medicine, Ladoke Akintola University of Technology Teaching Hospital, Osogbo, South-West Nigeria. Medical data for those with EMF from January 2003 to December 2009 were retrieved and analyzed.
Results
Only three cases of EMF were identified from a total of 12,794 medical patients containing a subset of 7956 cardiac patients. The prevalence of EMF was 0.02% and 0.04% for medical and cardiac patients, respectively. All the patients with EMF were in the second or third decades of life, and had right ventricular EMF and atrial fibrillation, but no eosinophilia.
Conclusion
This study shows that the prevalence of EMF has declined in the study area from 10% in the 1960s and 1970s to 0.02% for medical cases and 0.04% for cardiac cases in the first decade of the 21st century. Right ventricular EMF still predominates, but without eosinophilia. Improved health care delivery's positive impact on the control of communicable diseases might be responsible for these observed changes. More work needs to be done both within and outside Nigeria to follow this trend and unravel the mystery surrounding this poorly understood cardiac disease.
Background
Endomyocardial fibrosis (EMF) is an idiopathic disease that is mostly confined to the tropical and subtropical rainforest regions of the world. 1 However, subsequent reports have shown its occurrence in the guinea savannah of Nigeria,2,3 and even outside the tropical zones.4–7 It is the most common cause of restrictive cardiomyopathy worldwide. 8 The disease causes fibrosis of the endomyocardium of the ventricles, leading to impaired filling and subsequent heart failure of the affected ventricle. 9 The right ventricle is the most commonly affected, followed by biventricular and then left ventricular involvement. 9
Although several theories have been put forward as to the etiopathogenesis of EMF, there is no consensus of opinion on any of these, and the disease has therefore remained an enigma. 10 There are reports that the prevalence of EMF is decreasing globally, hence this study was undertaken to determine the prevalence of EMF as well as any changing patterns at Ladoke Akintola University of Technology Teaching Hospital, Osogbo, South-West Nigeria.
Materials and Methods
This was a retrospective descriptive study involving review of all medical admission cases, and all cases seen at the cardiology clinic and medical outpatient/specialty clinics at Ladoke Akintola University of Technology Teaching Hospital, Osogbo, South-West Nigeria, over a 7-year period covering January 2003 to December 2009. A total of 12,794 patients were studied to identify cases of EMF. More than half (n = 7956) of these patients were attending the cardiology clinic. Demographic, clinical, investigation, treatment, and follow-up data were retrieved from the case notes of patients identified to have EMF. Demographic data collected included age, gender, religion, occupation, marital status, and socioeconomic background. Ethical approval was given by the ethical committee of Ladoke Akintola University of Technology Teaching Hospital.
Results
The total number of patients attending our medical outpatient and cardiology clinics in the period spanning January 2003 to December 2009 was 12,794, with a subset of 7956 attending the cardiology clinic. Only three cases of EMF were found, giving an EMF prevalence in the study period of 0.04% and 0.02% for those attending the cardiology clinic and the medical outpatient clinics, respectively. There was one male and two females, giving a male to female ratio of 1:2. The mean age was 25 ± 4.95 years, with an age range of 17-30 years, whilst the duration of symptoms before reporting at our center was 3-5 years. All the patients were from a poor socioeconomic background.
The clinical features of the patients with EMF are shown in Table 1. The two female patients had New York Heart Association Class III disease, necessitating admission to stabilize them. Table 2 shows the results of the relevant investigations. All three of these patients had right ventricular EMF with atrial fibrillation and no eosinophilia. They were all seronegative for human immunodeficiency virus. All were stabilized on frusemide, spironolactone, amiodarone, and warfarin. Figure 1 shows the electrocardiogram of patient No 1 after having had amiodarone for some months to control the atrial fibrillation. Low voltage recording in most leads and frequent atrial ectopics are seen with atrial fibrillation in lead aVF. Figure 2 shows a recent chest × ray of patient No 2 with globular heart and oligaemic lung fields. The two female patients are still attending the clinic, but the male patient was lost to follow-up. Financial constraints precluded them from having definitive surgery.
Clinical features of patients.

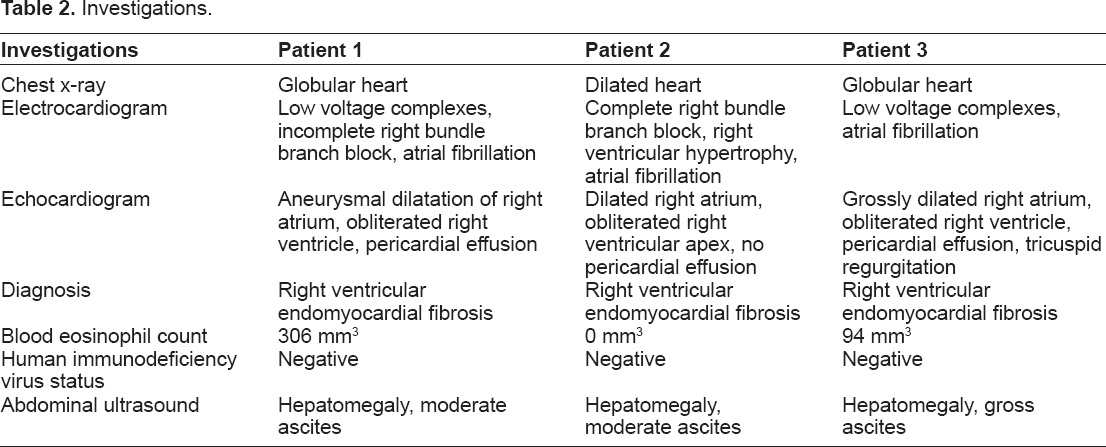
Investigations.

A 12-lead electrocardiogram for patient 1, a 17-year-old woman, showing atrial fibrillation in aVF and frequent atrial ectopics in other leads, with low voltage recording in most of the leads.

Chest x-ray for patient 2, a 30-year-old woman, showing a globular heart with oligemic lung fields.
Discussion
The prevalence of EMF in this study was 0.02% for cardiac cases and 0.04% for all medical cases, which compares favorably with a study in Enugu, South-East Nigeria, in which the prevalence of EMF was found to be 0.09% and 0.8% amongst admitted cases and echo-scanned cases, respectively. 11 This contrasts with a prevalence of 10% obtained in Nigeria during the 1960s and 1970s. 9 In 2001, Falase indicated that the prevalence of EMF might have decreased. 9 In Kampala, Uganda, where a high prevalence of 10%-15% was reported in the 1960s by Davies,12,13 a very low prevalence of 0.08% based on autopsy of 147 patients was reported by Farrer-Brown and Jarbit at the Mulago hospital in 1972. 14 Similarly in Kerala, India, the number of newly diagnosed cases of EMF decreased from 20 per year in 1976-1999 to 10 per year in 1991-2001, and to 7-8 per year in 2001-2007, further underscoring the global decline in prevalence of EMF.15,16 The majority of studies that reported a prevalence of 10% in Nigeria were carried out in South-West Nigeria, which is located in the heart of the tropical rain forest. This is also the location of the tertiary health facility reporting this very low prevalence. More recently, a study of 1441 cardiac patients referred for echocardiography at a tertiary health facility in Abeokuta, South-West Nigeria, did not find a single case of EMF. 17
The decline in the prevalence of EMF from 10% in the 1960s and 1970s to 0.02% in medical patients and 0.04% in cardiology patients in our study may be due to improvement in primary to tertiary health care delivery in the 21st century in Nigeria.
A lot of emphasis had been placed on primary health care since the mid 1980s to provide basic health care to the whole population, and coupled with this is the issue of free health care by different state governments across the country at both the primary and secondary health care levels. Also, the federal, state, and local governments have established and equipped more health facilities at all levels. More training institutions for doctors, nurses, community health extension workers, and other health care workers have also been established. There are now better facilities at all tertiary facilities, with every center having an echocardiography machine, hence it is easier to diagnose most cardiac lesions noninvasively. There is also a lot of aid from international bodies and communities to help stem the tide of all types of infection.
The overall effect of this is better control of infection, and early and prompt treatment of infected people. We are of the opinion that the etiology of EMF may be infections and/or parasites as hypothesized in earlier studies, and hence the fall in incidence of the disease with improved infection control. There is now an epidemiological transition under way in sub-Saharan Africa from communicable diseases to noncommunicable diseases, further underscoring the fact that infectious diseases are on a downward trend. A recent study performed in the same center as the current study showed that 44.99% of total admissions over a 3-year period were due to noncommunicable diseases. 18
The male to female ratio of 1:2 seen in this study is at variance with the previously reported gender distribution for EMF in Africa. D'Arbela et al reported a ratio 1:1 for 56 autopsies in Uganda, 19 and in an 8-year study, Andy et al reported a ratio of 3.1:1 for 41 cases in South-West Nigeria and 3.1:1 for 48 cases in South-East, Nigeria. 1 Similarly, Ike et al, working in South-East Nigeria, reported male to female ratios of 1.3:1 for adults, 1:1 for pediatric cases, and 3:1 for cases diagnosed by echocardiography. 11 Hence the gender distribution is not helpful, having shown a lot of inconsistency over the years. The mean age of the cases in our study was 25 ± 4.95 (range 17-30) years, because data were retrieved only for adult cases. However, it had been shown that people of any age can be affected. 20 Further, the age range in the study done by Ike et al was 2.5-74 years. 11 A recent study in Kerala, India, showed that most of the 54 newly diagnosed patients were older than 30 years, with only 23% being younger than 10 years; however, two of the patients (3.7%) were older than 60 years. 16 Duration of symptoms was 3-5 years, even in our only male patient, who presented with florid signs and symptoms of chronic right-sided heart failure. This is a common finding in this environment, whereby most of our patients present very late to the hospital and do not report the correct duration of symptoms. Only our male patient showed the classical egg-on-stick appearance. All the three patients presented to hospital during the rainy season (April–October), as had been reported in other studies in Nigeria.21,22
Table 2 shows the results of the relevant investigations done for the three patients in this study. Right ventricular EMF was the echocardiographic diagnosis in all cases. This is in agreement with the majority of the work done in Nigeria.9,11,23 However, some studies have shown that autopsies may reveal left ventricular or biventricular EMF despite the preponderance of clinical right ventricular EMF.1,24 All the patients had low voltage complexes on electrocardiography but only two had pericardial effusion. Low voltage complexes are usually caused by myocardial fibrosis with or without pericardial effusion. 25 Complete or incomplete right bundle branch block was common, indicating conduction pathway disruption on the right side. Atrial arrhythmias are common, especially atrial fibrillation,6,9,16,25 which was found in all of the study patients. Electrocardiography in patients with EMF is usually nonspecific or sensitive,2,6 and similarly the chest x-ray; these investigations only act as leads to the possible diagnosis and support the echocardiography findings.
Eosinophilia was not found in any of our patients, as reported earlier by some other studies performed in the same environment as this current study, where a strong association was found between hypereosinophilia induced by helminthes/microfilaria and endomyocardial fibrosis.1,26,27 Conservative treatment with frusemide, spironolactone, and warfarin was given. Amiodarone was then offered to the patients as needed to control atrial fibrillation, because financial constraints precluded their referral for definitive surgery.
Conclusion
The prevalence of EMF in our study area has declined from 10% in the 1960s and 1970s to 0.02% for medical cases and 0.04% for cardiac cases. Right ventricular EMF still predominates, but without eosinophilia. EMF essentially remains a poorly understood restrictive cardiac disease, although its prevalence is now on the decline globally. We suggest that the decline in the tropics is due to better control of communicable diseases occasioned by an improved health care delivery system in the last few decades. More studies still need to be done to follow this trend of prevalence and offer plausible answers to the mystery surrounding its etiology and possible preventive strategies.
Author Contributions
Conceived and designed the experiments: PO, AO. Analysed the data: PO. Wrote the first draft of the manuscript: PO. Contributed to the writing of the manuscript: PO, AO. Agree with manuscript results and conclusions: PO, AO. Jointly developed the structure and arguments for the paper: PO, AO. Made critical revisions and approved final version: PO, AO. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.
Footnotes
Acknowledgments
We sincerely appreciate the assistance of Mr. Asa and his team from the medical records department in retrieving the patient case notes used in this study. We are also grateful to the house officers in the cardiology unit for their assistance with data collection, and to EO Asekun-Olarinmoye, associate professor of community medicine, for reading the manuscript and offering useful suggestions. Finally, we thank Mrs. Ogunyemi, our departmental secretary at Osun State University, for her secretarial assistance.