
Abstract
Computed tomography (CT) has been used as the reference imaging technique for the initial staging of diffuse large B-cell lymphoma until recent days, when the introduction of positron emission tomography (PET)/CT imaging as a hybrid technique has become of routine use. However, the performance of both examinations is still common. The aim of this work was to compare the findings between low-dose 2-deoxy-2-(18F)fluoro-D-glucose (18F-FDG) PET/CT and full-dose contrast-enhanced CT (ceCT) in 28 patients with localized diffuse large B-cell lymphoma according to PET/CT findings, in order to avoid the performance of ceCT. For each technique, a comparison in the number of nodal and extranodal involved regions was performed. PET/CT showed more lesions than ceCT in both nodal (41 vs. 36) and extranodal localizations (16 vs. 15). Disease staging according to both techniques was concordant in 22 patients (79%) and discordant in 6 patients (21%), changing treatment management in 3 patients (11%). PET/CT determined a better staging and therapeutic approach, making the performance of an additional ceCT unnecessary.
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common type of lymphoma, representing approximately 30% of all lymphomas and appearing in a localized stage in about 30% of the cases. It is a fast growing neoplasm, with high proliferative rate and favorable response to chemotherapy. Complete response after first-line treatment ranges about 70%-80%, with a five-year survival rate over 60%. 1
Once the diagnosis is established, it is of paramount importance to define the extension of the disease in order to evaluate the individual prognostic and the best therapeutic approach. Computed tomography (CT) has been the most commonly used imaging technique until recent days; 2 its diagnostic criteria depend on size, shape, and contrast enhancement of lesions. On the other hand, fundamentals of positron emission tomography (PET) are based on the use of certain molecules labeled with radioactive isotopes (positron emitters), which allow obtaining functional images. The most commonly used radiopharmaceutical is 2-deoxy-2-( 18 F) fluoro-D-glucose ( 18 F-FDG), a glucose analog that is captured by cells with high metabolic needs. 3 The introduction of the hybrid technique PET/CT provides metabolic and anatomic information, solving the main limitations of both techniques separately, improves anatomic resolution of PET, and allows the detection of increased metabolic activity in lymph nodes and organs without CT abnormalities.
However, in some centers, a thoracic and abdominal contrast-enhanced CT (ceCT) scan is still of routine use for staging of lymphomas, as it is a highly available examination and in many situations is used as the initial test in patients with constitutional symptoms, while PET/CT is a less accessible technique in which the use of iodinated contrast is controverter. The aim of our work was to compare noncontrast-enhanced PET/CT with ceCT in patients with localized DLBCL according to PET/CT findings, with the purpose of avoiding the performance of a ceCT.
Patients and Methods
Patients
This is a retrospective study of 28 patients (16 male) with a median age of 59 years, diagnosed of DLBCL between 2007 and 2011, in a localized stage according to PET/CT findings. The characteristics of the patients are detailed in Table 1. In agreement with the Cotswold modification of Ann Arbor classification, localized disease is defined as involvement of nodal territories in the same side of the diaphragm, or as a disease that is primarily originated in an extralymphatic organ, with or without regional nodal involvement (stages I—II). 4 Evaluation of our patients included an anamnesis, physical examination, hemogram, biochemistry, hepatic and renal parameters, lactate dehydrogenase (LDH), β2-microglobulin and viral serologies, chest X-ray, and bone marrow biopsy. All of them underwent a PET/CT without iodinated contrast (low dose) and a ceCT (high dose). Time interval between both tests was no longer than two weeks; during this time frame, none of the patients received any treatment. Patients with neck involvement on PET/CT who did not have a cervical ceCT of this area were excluded from the study. All the patients were subsequently controlled, either by PET/CT or clinically.
Patient characteristics.

Stage according to PET/CT findings and in agreement with the Cotswold classification.
Examination Protocol
PET/CT
All data were acquired in a hybrid tomograph Discovery ST (GE Healthcare), 60-120 minutes after the injection of 3.7 MBq/kg (0.1 mCi/kg) of 18 F-FDG. Patients fasted for at least six hours and were abundantly hydrated. In all of them, glucose level was tested immediately before radiotracer injection, to make sure that it was lower than 7.78 mmol/L.
Whole-body acquisition protocol included a CT scan (140 kV and 80 mA) and a PET (three minutes per field of view) in a two-dimensional mode for patients scanned before 2009 and in a three-dimensional mode afterward. CT images were used for attenuation correction and anatomical localization of PET findings.
Contrast-Enhanced CT
Thoracoabdominal studies were acquired in two multidetector CT units, one BrightSpeed and one LightSpeed VCT (GE Healthcare) of 16 and 64 detectors, respectively (140 kV and dose-modulated current with a maximum of 300 mA), after intravenous administration of 100-150 mL (according to each patient's weight) of a nonionic iodinated contrast agent at 4-4.5 mL/second.
Data Analysis
Images were independently evaluated by experienced specialists in nuclear medicine (PET/CT) and radiology (ceCT), identifying the number of nodal and extra-nodal involved localizations.
In PET/CT technique, positive lesions were considered as areas of focal or diffuse FDG uptake (higher than the background) in nonphysiologic localizations (including lymph nodes of less than 1 cm and normal size organs). The criteria to consider positive lesions on ceCT included lymph nodes over than 1 cm in the shorter axis, increased organ size, and/or abnormal contrast uptake.
Results
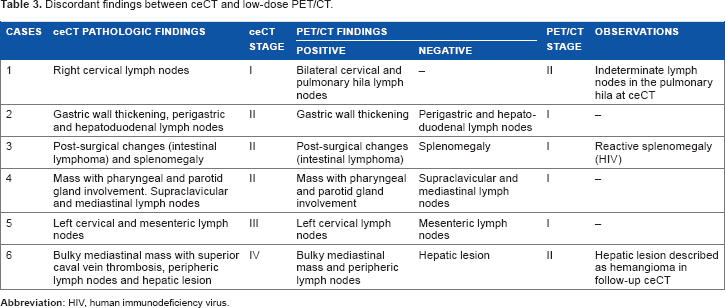
In the evaluation of nodal and extranodal localizations, PET/CT showed the involvement of 41 and 16 territories, and CT showed the involvement of 36 and 15 territories, respectively. The distribution of affected territories according to each technique is listed in Table 2. In view of PET/CT findings, 16 patients were considered as stage I (57%) and 12 as stage II (43%), while CT findings classified them as stage I in 13 cases (46.4%), stage II in 13 other patients (46.4%), and advanced disease (stages III and IV) in 2 of them (7.1%). Comparing both imaging techniques, 22 cases were concordant (79%) and 6 were discordant (21%); the latter are further detailed in Table 3. In three of these discordant patients, a change of stage also implied a change in the therapeutic approach (diminishing the number of chemotherapy cycles). All patients were treated with standard chemotherapy.
Distribution of nodal and extranodal involved territories according to PET/CT and ceCT.

Discordant findings between ceCT and low-dose PET/CT.
Discussion
For a long time, ceCT has been the most widely used imaging technique for the study of lymphomas; however, in the past few years, PET/CT has proved superior in initial staging, relapse, and response assessment of FDG-avid lymphomas, as pointed in the last Lugano classification.5–10 Nevertheless, PET/CT is usually performed with a low-dose CT and without iodinated contrast, mainly used for anatomic localization and attenuation correction. In this setting, the hybrid examination is often performed as complementary to ceCT. Could a low-dose PET/CT be enough for disease staging, consequently decreasing radiation dose to the patient? Different groups have already studied this topic,11–14 comparing sensitivity and specificity of a low-dose, noncontrast-enhanced PET/CT with a high-dose ceCT (coregistered with the PET acquisition or independently performed). These studies did not find any significant difference among two CT modalities regarding nodal or extranodal, even a low-dose PET/CT could detect more lesions.14–17 Another point of discussion and of interest for our group is finding out if a low-dose noncontrast-enhanced PET/CT for initial staging of patients with DLBCL localized disease (I-II) avoided high-dose ceCT. In this sense, Rodríguez-Vigil et al 11 published data comparing the results obtained with and without iodinated contrast in a PET/CT scanner and avoiding high-dose ceCT. They did not find any significant differences in the number of nodal and extranodal involved regions. However, Schaefer et al 12 included patients with both Hodgkin's disease and non-Hodgkin lymphomas in different stages, 30 of them in stage IV.
In our study, the unique selection of patients with localized disease was intended to limit the possibility of differences between both imaging techniques, studying patients with low tumor volume. In our opinion, discordant results increased including patients with advanced stages, as occurred in the previously cited works.11,12 In the current study, low-dose PET/CT detected more lesions than ceCT, nodal (41 vs. 36) and extranodal (16 vs. 15), similar to those mentioned in the literature for aggressive lymphomas.15–17 Differences observed in nodal involvement could be explained by the capacity of PET/CT to prove that involvement of infra lymph nodes lesser than 1 cm are not considered pathologic on the CT. 18 Regarding extranodal locations, differences could be explained due to the decision to include only localized stages, some of them with primary extranodal involvement (10 cases, 36%).
Analyzing particularly Ann Arbor stage of the disease, six patients (21%) were discordant between the two imaging procedures (Fig. 1). In one patient, PET/CT upstaged the disease and downstaged in five of them, changing the therapeutic management in three of them (11% of all patients), leading to a reduction of cycles of chemotherapy. In the study by Schaefer et al, 12 PET/CT changed the therapeutic approach in up to 16% of patients.

Sixty-two year-old woman diagnosed with DLBCL. ceCT showed pharyngeal involvement with extension to the right parotid gland, as well as supraclavicular and mediastinal lymph nodes of up to 11 mm (A, red arrow). PET/CT proved high hypermetabolism in the pharyngeal lesion (B), even if supraclavicular and mediastinal lymph nodes did not show increased uptake of 18 F-FDG (C, blue arrow). Due to the absence of pathologic metabolic activity, these lymph nodes were not considered as disease involvement, classifying the patient as stage I. According to ceCT findings, she would have been classified as stage II.
It is important to note some limitations of our study. For instance, we are aware of the retrospective nature of the study and the small number of patients. However, the population included is histologically homogeneous, and both imaging procedures were performed following proper standards and at appropriate time intervals.
Conclusion
Low-dose, noncontrast-enhanced PET/CT is a very good imaging technique for initial staging of DLBCL. Considering localized lymphomas, the current results demonstrate a better performance of PET/CT when compared with ceCT in detecting both nodal and extranodal lesions, précising the disease extension and allowing a better therapeutic approach. In this group of patients, an additional high-dose ceCT could be avoided.
Author Contributions
Conceived and designed the experiments: AS-L, MC-R, and SM. Analyzed the data: AS-L and MC-R. Wrote the first draft of the manuscript: AS-L and HP. Contributed to the writing of the manuscript: MC-R, JH-G, and SM. Agreed with manuscript results and conclusions: MC-R, SM, EG-B, and CG-C. Jointly developed the structure and arguments for the paper: AS-L, MC-R, and SM. Made critical revisions and approved the final version: AS-L, MC-R, SM, JH-G, HP, EG-B, and CG-C. All the authors reviewed and approved the final manuscript.