
Abstract
The frequency of anemia, iron deficiency, and the long-term need for IV iron following Roux-en-y gastric bypass (RYGB) surgery has not been well characterized. Three-hundred and nineteen out of 904 consecutive subjects who underwent RYGB at Penn State Hershey Medical Center from 1999 to 2006 met the inclusion criteria for a preoperative complete blood count (CBC) and at least one CBC >6 months following surgery. Cumulative incidence of anemia 7 years post procedure was 58%. Menstruation status and presence of preoperative anemia were predictive of anemia by univariate analysis and multivariable Cox regression (
Introduction
Weight loss surgery is an effective and durable treatment for clinically severe obesity and its associated conditions. Bariatric surgery not only promotes weight loss but also significantly reduces cardiac-related death, myocardial infarction, and stroke. 1 Approximately 220,000 Americans had some form of bariatric surgery in 2008, with the Roux-en-Y gastric bypass (RYGB) procedure accounting for the vast majority. 2 Postoperative anemia has been reported in approximately one-fourth to one-half of the patients within 6 months to 4 years following surgery.3–9 Despite its proven benefits, several nutritional deficiencies may be seen after gastric bypass. These include iron, calcium, the fat-soluble vitamins A, D, E, and K, vitamin C, copper, selenium, and zinc10–16 However, by far the most common of these is iron deficiency. Women, especially those who are menstruating, appear to be at higher risk for developing iron deficiency,5,8,17 and oral iron supplementation is inconsistent in preventing anemia.13–19 Moreover, data beyond 4-5 years are sparce, and the long-term need for intravenous (IV) iron replacement has not been well characterized.
Since iron deficiency anemia may take years to develop, we sought to determine the long-term incidence of anemia, iron deficiency, and the prevalence of IV iron infusions five or more years after RYGB surgery.
Methods
Patient Selection and Variables Assessed
In accordance with the principles of the Declaration of Helsinki, and following the approval of the Penn State College of Medicine Institutional Review Board, 904 subjects were identified from our prospective bariatric surgery database as having undergone RYGB surgery at Hershey Medical Center from 1999 to 2006. Electronic medical records (EMRs) were assessed on all subjects for iron supplementation, pre- and postoperative complete blood counts (CBCs), ferritin levels, menstruation status at time of surgery, and length of the Roux limb. Women were considered to be menopausal if their age was >50 years at the time of surgery. Subjects were considered eligible for inclusion if a preoperative CBC and at least one postoperative CBC at >6 months from the time of surgery were available. Anemia was defined as a hemoglobin <12 g/dL for women and <14 g/dL for men. Iron deficiency was defined as a ferritin level <10 μg/L. Subjects were evaluated for development of anemia and iron deficiency. IV iron therapy was given at the discretion of the hematology consultant for patients with symptomatic iron deficiency anemia who were intolerant or refractory to oral iron supplements. Subjects were censored from future analysis once they became anemic. EMR data were censored as of May 12, 2012.
Routine Surgical and Postoperative Protocol
RYGB was performed with reconstruction, as depicted in Figure 1.
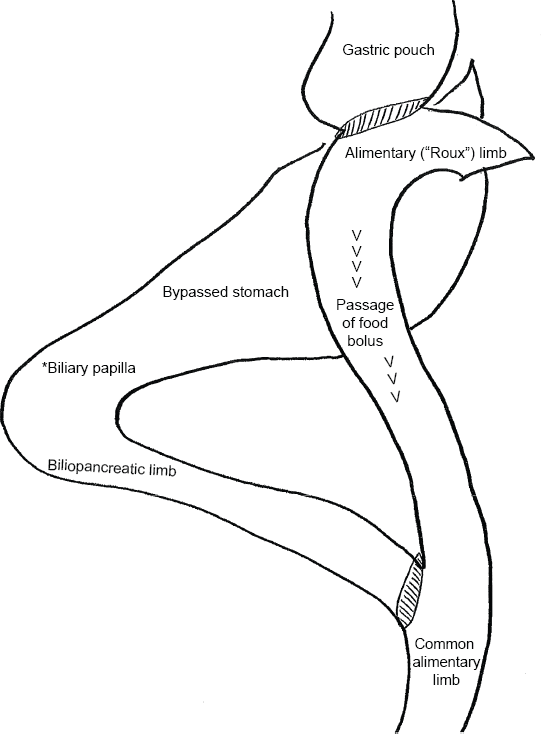
Depiction of anatomic rearrangement of Roux-en-Y gastric bypass, demonstrating that the entire duodenum is excluded from the absorption of nutrients.
The conventional Roux limb was between 100 and 150 cm and the pancreatobiliary limb between 40 and 50 cm. All patients were instructed to take one of the more absorbable forms of oral iron, such as funarate/gluconate, 28 mg at bedtime, preferably with vitamin C 500 mg, and not within 2 hours of calcium supplements, in addition to calcium, vitamin D, a multivitamin containing vitamin A, and vitamin B12 supplements. Patients were informed that these vitamin and mineral supplements would be required lifelong. Follow-up visits were routinely scheduled at 1 month with the dietician, at 3 months with the surgeon and dietician, at 9 months with the dietician, and at 12 months and then annually for 5 years with the surgeon. At 1 month, patients were given an information sheet to be given to their primary physician requesting CBCs along with routine laboratory monitoring quarterly for the first year and annually thereafter.
Statistics
Univariate analyses using Chi-squared test and Student's
Results
Three-hundred and nineteen subjects met the inclusion criteria of a preoperative CBC and at least one postoperative CBC >6 months from the time of surgery recorded in the EMR.
Mean age at surgery was 45 years (range 18-67 years). Two-hundred and sixty-nine (84%) were women and 50 (16%) were men. One-hundred and forty-eight (55%) of the women were menstruating at the time of surgery. The median follow-up time of the 319 subjects was 56 months with an interquartile range 31-71 months (minimum 5.9 months, maximum 90.4 months). Subjects who did not meet the inclusion criteria had similar distributions in age, sex, weight, and body mass index (BMI), except for a higher (73%) proportion of women menstruating at the time of surgery. Preoperative hemoglobin levels were observed for 62% of the subjects who did not meet the inclusion criteria, with a mean (standard deviation) of 13.6 (1.3) g/dL compared to 13.4 (1.2) for the subjects who met the inclusion criteria.
One-hundred and twenty-two of the 319 subjects developed anemia. Thirty-six of the 122 (30%) had ferritin levels recorded. Twenty-two (61%) of the 36 subjects tested, representing 18% of the 122 subjects with anemia, were found to be iron deficient using a standard cut-off of 10 ng/mL. Fourteen (64%) of the 22 subjects with iron deficiency anemia were women of menstrual age. For patients who developed anemia, the average postoperative hemoglobin concentration measured at >6 months postoperatively was 12.6 (1.1) g/dL in men and 10.7 (1.1) g/dL in women.
Time to event analysis showed that the risk of developing anemia by 7 years post procedure was 58% (Fig. 2).

Kaplan-Meier (KM) cumulative event rate of anemia-free subjects of the study cohort. The number of subjects at risk at each 20-month time interval is indicated at the bottom of the graph. The cumulative rate of anemia is 100% minus the KM estimate.
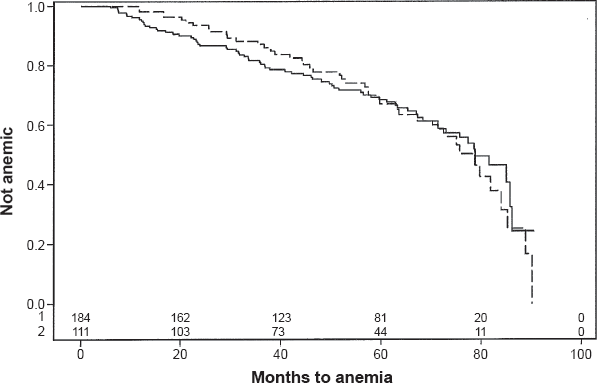
Among the women menstruating at the time of surgery, 62% developed postoperative anemia by 7 years post procedure (Fig. 3).
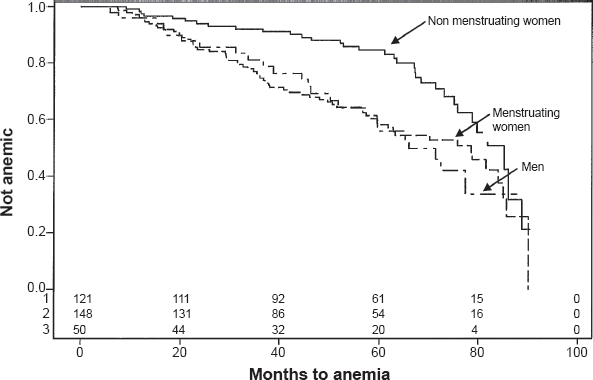
Kaplan-Meier cumulative event rate of anemia-free subjects by sex and menstruation status at the time of surgery. Nonmenstruating women —; menstruating women men––; Log-rank
The risk of postoperative anemia was significantly higher in the women who menstruated at the time of surgery compared to those who did not (
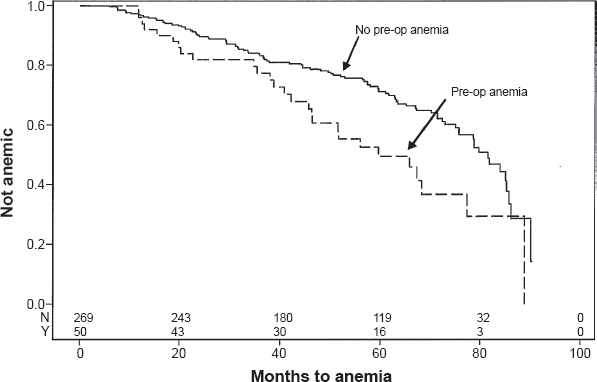
Kaplan-Meier cumulative event rate of anemia-free subjects by preoperative anemia status. Preop anemia no—; yes—; Log-rank
One-hundred and seventy-five (55%) subjects received supplemental oral iron after surgery. However, postoperative iron replacement did not reduce the overall rate of anemia (Fig. 5).
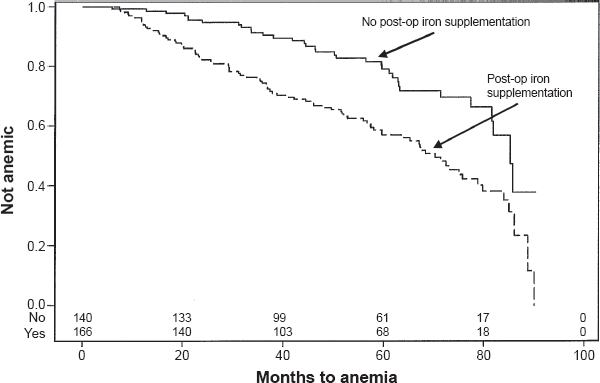
Kaplan-Meier cumulative event rate of anemia-free subjects by supplemental iron status after surgery. Iron post op no—; yes—; Log-rank
Longer Roux limbs seemed to be associated with the development of anemia at years 1-4, but the overall difference in the whole study period did not reach statistical significance (Fig. 6).
Kaplan-Meier cumulative event rate of amemia-free subjects by length of Roux limb. Long loop —; Short loop —; Log-rank
Twenty-seven subjects representing 8.5% of our study cohort and 22% of our anemic subjects with intolerance or refractoriness to oral iron received IV iron sucrose or low molecular weight iron dextran for iron deficiency anemia with a hemoglobin of <10 g/dL 1-111 months postoperatively (mean 51, median 52 months) (Fig. 7).
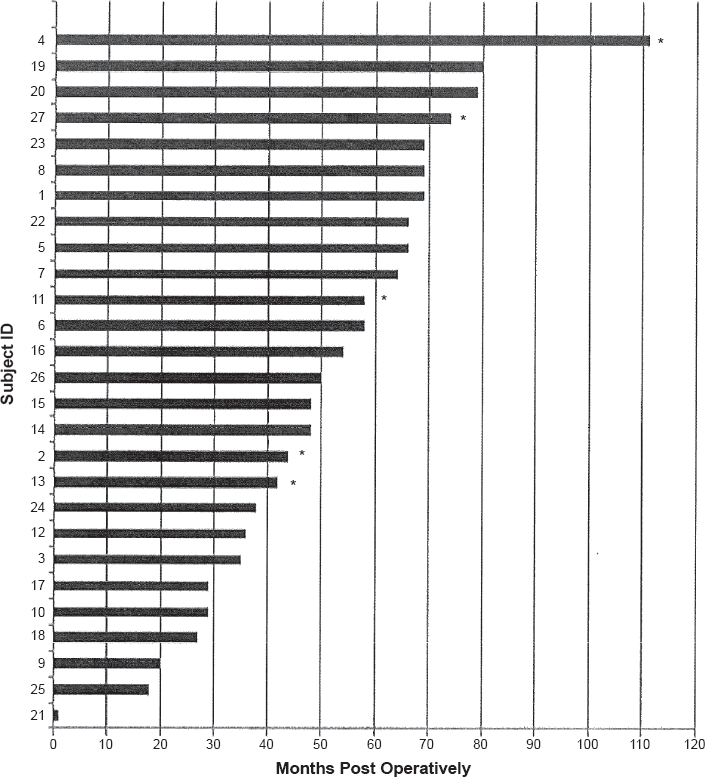
Time to IV iron replacement after surgery.
The usual doses for each event were 1 g of iron sucrose given over three infusions, or a single infusion of 1 g of iron dextran. Five of the 27 received infusions on two or more separate occasions. Twenty-four were women, of whom 18 (75%) were under 51 years of age. Ten of the 27 also received red cell transfusions more than 1 year postoperatively (mean 59 months, median 50 months), and two additional women received red cell transufsions but no IV iron 2 and 3 years postoperatively (data not shown). Thirteen of the 27 subjects had hemoglobin values recorded before and after receiving intravenous iron (Table 1). All but one had a hemoglobin rise of >2 g/dL within 4-6 weeks following the infusion. The average pre-infusion hemoglobin was 9.1 g/dL and the average post-infusion hemoglobin for the those not receiving red cell transfusions was 12.4 g/dL.
Thirteen patients with pre and post-hemoglobin (Hgb) values within 1-6 months after IV iron.

Three subjects also received packed red cells for iron deficiency anemia.
Menstruation status and presence of preoperative anemia were predictive of postoperative anemia in the univariate analysis (Table 2,
Univariate and multivariable analysis of predictors of anemia occurring up to 7 years after RYGB surgery in a cohort of 319 patients.

Discussion
Mammalian iron absorption requires the transfer of iron across both the apical and basolateral membranes of enterocytes. This takes place preferentially in the duodenum and occurs in both nonheme and heme forms. Nonheme iron enters the cell through the divalent metal transporter DMT-1 and is transferred across the basolateral membrane to the circulation by ferroportin. Heme binds to its receptor HCP-1 and is absorbed directly into the duodenal enterocyte by a process that is not well understood.20,21 However, there is a gradient for nonheme iron absorption throughout the small intestine, at least in animals.22–24
RYGB is a procedure in which the distal stomach, duodenum, and proximal jejunum are bypassed, precluding exposure of the food bolus to these sites in the postoperative biliopancre-atic limb. Food bolus exposure to the normal gastric acid gradient along the foregut is also altered. Therefore, exclusion of the duodenum from alimentary flow and pH alterations along mucosa with absorptive potential are both implicated in the development of iron deficiency anemia after RYGB. Perioperative blood loss is unlikely to contribute significantly because the reported rate of bleeding requiring transfusion during or immediately after RYGP is on the order of only 1%-4%. 25
Our study is in agreement with previous reports that iron deficiency and iron deficiency anemia are significant complications following RYGB. Reported rates of iron deficiency range from 15% to 60% and of iron deficiency anemia from 10% to 52% in retrospective studies.11–15 However, only three of these studies have follow-ups of 4 years or more,4,9,11 and the true incidence of iron deficiency and iron deficiency anemia is difficult to ascertain. In a prospective study by Ruz et al of 51 individuals, the percentage of anemic subjects changed from 1.5% at the beginning of the study to 38.8% at 18 months. 3 In a larger prospective study by Avinoah et al of a random group of 200 patients undergoing bariatric surgery, mean values of hemoglobin and iron showed a gradual and significant decrease 6-8 years after surgery; 26 however, the actual values were not reported.
Our study of 319 subjects showed a cumulative incidence of anemia of 58% by 7 years post procedure. This is one of only three studies8,9,17 to systematically report long-term results beyond 5 years. The main findings were that the rate of development of anemia in individual subjects continued to increase over at least 7 years, and that 8.5% of all 319 subjects and 22% of 122 anemic subjects received IV iron replacement with good response at an average of 4 years postoperatively.
Eighteen percent of our anemic subjects were confirmed to have iron deficiency, consistent with published literature. However, this is likely a gross underestimate, since only one-third had ferritin levels available for review, and of these, 61% had iron deficiency. Furthermore, serum ferritin alone may not be the optimal way to define iron deficiency, as it is an acute phase reactant that is generally higher in obese people, presumably secondary to underlying chronic inflammation. 27 In this setting, our threshold of 10 μg/L may have been too low. Previous studies have assessed serum iron and total iron binding capacity (TIBC), but these also are poor markers for iron deficiency because serum iron is influenced by iron absorption from meals, infection, inflammation, and diurnal variation, and TIBC is affected by malnutrition, inflammation, chronic infection, and cancer. A ferritin level of <10 ng/mL is very specific for iron deficiency, but in older patients or those with inflammatory states one cannot rule out iron deficiency until the ferritin level is >100 ng/mL. 28 Guyatt et al found that the likelihood ratio for iron deficiency was positive up to a ferritin level of 40 ng/mL in the absence of inflammation and up to 70 ng/mL in the presence of inflammation. 29 Had we raised the serum ferritin threshold to 40 ng/mL, we would have increased our percentage of anemic patients with iron deficiency from 18% to 21%. Had we raised it to 70 ng/mL, 29 (24%) of our anemic patients would have been classified as being iron deficient. Although raising the ferritin cutoff may improve the rate of detection of iron deficiency, an accurate assessment of iron deficiency in the setting of chronic inflammation awaits the development of a reliable test to measure hepcidin levels.
Rates of anemia and iron deficiency were highest in menstruating women, 62% of whom became anemic by 7 years postoperatively. This is greatly increased from the 12% incidence of iron deficiency in women of childbearing age in the National Health and Nutrition Examination Survey, 30 and the 13% incidence of anemia in women of reproductive age in the WHO survey. 31 Iron supplementation did not appear to correct the development of anemia over time. Suprisingly, the rate of anemia in men was similar to that in menstruating women. This may have been affected by the small sample size or the higher rate of preoperative anemia in the men.
The length of the Roux limb was associated with development of anemia at post-surgical yearly intervals 1-4, but lost significance by year 5 and was not significant in the multivariate analysis. Mechanistically, this early association could be due to greater malabsorption of nutrients in patients with longer limbs, with subsequent adaption of enterocytes facilitating iron absorption over time.
A gradient for nonheme iron absorption throughout the small intestine has been demonstrated in animals.22–24 Such an adaptive mechanism could explain why some patients absorb enough food and supplemental iron post gastric bypass surgery to prevent the development of anemia in the absence of other causes such as menstrual blood loss, occult gastrointestinal bleeding, or a deficiency of other micronutrients, which were not examined in this study.
The significant association of preoperative anemia with postoperative anemia is not unexpected, given that preexisting conditions other than the role of adipose tissue leading to low hemoglobin concentrations preoperatively would be unlikely to change with gastric bypass. The fact that oral iron after surgery did not correct the anemia is not surprising, since oral iron is excluded from the biliopancreatic limb encompassing the excluded stomach, duodenum, and proximal jejunum. A recent report has shown that iron absorption from a single oral dose of ferrous sulfate is reduced by more than 60% after RYGB. 32
Published data identifying patients receiving IV iron supplementation following RYGB are limited. In one study, anemia was corrected in most of 23 patients who received iron dextran post RYGB for refractory iron deficiency anemia, with an 85% probability of remaining in an iron-replete state at 1 year. 33 In another study, intravenous iron was required in 6.7%. 17 In an earlier retrospective analysis of 42 bariatric surgery patients who received IV iron, premenopausal women required earlier replacement. 34 This represented approximately 4% of the patients who underwent all forms of bariatric surgery at the parent institution during the study period.
Clearly, there is a range of iron deficiency that is moderate and does not require IV iron. However, a seminal observation in our study was that 27 subjects, representing 8.5% of our study cohort and 22% of anemic subjects, received IV iron infusions a mean of 44 months and a median of 32 months after surgery. The vast majority of these (90%) were women, of whom 75% were premenopausal. Increases of >2 g/dL of hemoglobin within 6 months following IV iron infusions were observed in a subset of all but 1 of 13 subjects with data pre and post infusion. For this group, the average hemoglobin rose from 9.1 to 12.4 g/dL, confirming the efficacy of IV iron replacement in subjects previously unresponsive or intolerant to oral iron supplements.
Although currently approved IV iron preparations have been shown to have an excellent safety profile in multiple studies comprising thousands of subjects with iron deficiency anemia, all iron products can cause hypersensitivity or other reactions, some of which are severe. 35 This small but potentially avoidable risk, plus the inconvenience and cost of repeated iron infusions, can have a major impact on quality of life. This outcome needs further characterization in prospective studies.
Our study has limitations due to incomplete data. Only 35% met our inclusion criteria on review of the EMR because the others had no follow-up CBC recorded 6 months or longer after surgery. This low response rate may indicate a self-selection bias, with subjects more likely to return for follow-up if they were symptomatic from anemia or otherwise ill, thereby increasing the prevalence of anemia in our study population. However, those who were excluded had similar distributions of age, gender, weight, and BMI, except for a higher proportion of menstruating women, which would argue strongly against a self-selection bias. Additionally, only 30% of anemic subjects had ferritin levels recorded. However, our overall rates of anemia, iron deficiency, and iron deficiency anemia were consistent with the published literature. Other limitations include lack of data regarding compliance and the coexistence of other micronutrient deficiencies such as B12 and folate deficiency, which have been shown to be substantial following RYGB.
Despite a clearly articulated schedule requesting follow-up visits and CBCs at least annually for 5 years following RYGB, the lack of data for review in this single-institution study highlights the fragmented care received by this patient population. Other bariatric surgery centers have had similar experiences. The reported 5-year follow up rate of 1359 eligible patients in the International Bariatric Surgery Registry was only 5.1%, 36 and the 5-year follow-up at major bariatric centers is as low as 14% (oral communication from Matthew Hutter, MD, Massachusetts General Hospital). When taken in this context, our 35% follow-up rate at 7 years is commendable. Clearly, a better system for long-term follow-up is needed to detect anemia from deficiencies of iron and other nutrients, which may take years to develop.
Credentialing of bariatric centers of excellence includes recommended rates of annual follow-up that are difficult to achieve. Traditionally, credentialed bariatric centers of excellence have been required to demonstrate a plan for at least 5-year follow-up of patients undergoing weight loss surgery. While a plan may in fact be in place, follow-up of patients, particularly in countries without national health insurance, is generally poor. Patient mobility, changes in providers, loss of health insurance, cost of care, cost of supplements, lack of uniformity of electronic health records, and innumerable other factors limit patient follow-up. More definitive guidelines, closer collaboration with primary care providers, and improved methods of tracking are needed to increase our understanding of the long-term consequences and to improve outcomes following RYGB. This is particularly true given the rise in popularity of bariatric surgery for the control of obesity and obesity-related comorbid conditions.
In summary, we have shown a 58% cumulative incidence of anemia by 7 years post RYGB. Iron deficiency anemia was demonstrated in 18% of a subset with ferritin levels available for review. Importantly, 8.5%, two-thirds of whom were women of menstrual age ≤50 years, and 22% of all subjects with anemia required IV iron supplementation a mean of 47 months postoperatively because of unresponsiveness or intolerance to oral iron. Well-designed prospective studies are needed to determine the magnitude of this under recognized longterm risk for the development of iron deficiency anemia after RYGB and to better define those at increased risk for needing IV iron infusions. Additionally, translational studies to elucidate factors controlling iron uptake by the remaining alimentary surface are needed to identify adaptive mechanisms that may reduce the risk for development of iron deficiency following RYGB surgery.
Author Contributions
Conceived and designed the experiments: AK and EE. Analyzed the data: DM and LK. Wrote the first draft of the manuscript: AK. Contributed to the writing of the manuscript: AK, KD, CD, AR, LK and EE. Agree with manuscript results and conclusions: AK, KD, CD, AR, DM, LK and EE. Jointly developed the structure and arguments for the paper: AK, KD, CD, AR and EE. Made critical revisions and approved final version: KD, CD and EE. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
The authors gratefully acknowledge the assistance of Gail Long, Michelle Moore, and Linda Nelson in the collection of data and the preparation of the manuscript.