
Abstract
Objective
To estimate the prevalence of connective tissue diseases in patients presenting with fever of unknown origin (FUO).
Patients and Methods
In this study thirty patients diagnosed as FUO (Group 1), in 2008, were included in an observational study and diagnostic workup. Additionally, retrospective analysis of seventy patients’ files (Group 2), for patients who presented with prolonged unexplained pyrexia to the same hospital in the previous two years, was performed. Patients were subjected to: full clinical assessment including full history taking, thorough clinical examination, laboratory investigations including the basic investigations for patients with prolonged fever, complete blood count, erythrocytes sedimentation rate, urine analysis and culture, blood culture, sputum culture and plain chest X ray. Further diagnostic work up and/or procedures were requested according to the potential diagnostic clues (PDC) present in every patient.
Results
Out of 100 FUO patients, 50% were found to have infectious diseases, 24% were found to have connective tissue diseases, 8% miscellaneous causes and 7% neoplastic diseases (P < 0.05). In 11 patients no definite cause for FUO could be identified. Connective tissue patients were: eight systemic lupus patients (33.3%), five patients with familial mediterranean fever (20.8%), four patients with rheumatoid arthritis (16.6%), three patients (12.5%) with Still's disease and Rheumatic fever and one patient with Behçet syndrome/Crohn's disease (4.3%), (P < 0.05).
Conclusions
Despite the advanced technology, FUO remains a challenging medical problem. Infections were the most common cause of FUO in Egypt, confirming the trends found in other parts of the world. There was an increased prevalence of connective tissue patients presented with prolonged unexplained fever. A keen clinical eye, meticulous history taking and repeated physical examination remained the most important diagnostic tools in FUO patients.
Introduction
Fever is a frequent medical problem, it occurs as a response to noxious stimuli either infectious or non-infectious. It is usually associated with systemic upset symptoms. Fever of unknown origin (FUO) is a pattern of fever with temperature higher than 38.3 °C on several occasions over more than 3 weeks, in which the diagnosis remains uncertain after the initial diagnostic work up. 1 Temperature should be measured every three hours and recorded. By the end of the day a graph could be plotted. FUO always represents diagnostic and therapeutic challenges. 2 It can be the initial symptom of connective tissue disease, an expression of the disease flare or unusual infections. 3 Many patients who presented with FUO were found to have connective tissue diseases. The fever here is due to abnormal immune response in which antibodies are produced against the body's antigens. The well known example is in systemic lupus erythematosus (SLE). 4 Out of 11 juvenile SLE patients 10 (90.9%) have fulfilled the preliminary guidelines for macrophage activation syndrome, three of them with macrophage hemophagocytosis in bone marrow aspirate and hyperferritinemia. The hallmark of this syndrome is excessive activation and proliferation of T lymphocytes and macrophages that phagocytose erythrocytes, leukocytes and platelets with massive hypersecretion of proinflammatory cytokines. Clinically it is characterized by the occurrence of unexplained fever and cytopenia. However, specific infections, brucellosis, tuberculosis and hematological malignancy are the classical differential diagnosis. 3 Interleukin I (IL-1), IL-6 and other endogenous pyrogens like tumor necrosis factor α (TNF-α) have been shown to play a pivotal role in the pathogenesis of FUO. Familial mediterranean fever and Crohn's disease usually present with FUO. Muñoz et al, 5 report two patients with Crohn's disease who presented with fever of unknown origin, and mild intestinal symptoms. Kikuchi-Fujimoto disease is described as a recent cause of FUO, it is a histocytic necrotizing lymphadenitis that presented with lymphadenopathy and prolonged fever, elevated erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) levels, rarely bilateral pleural effusion, and interstitial lung disease, SLE and other causes of FUO are the differential diagnosis.6,7
Interestingly, Rovers et al 8 introduced a new imaging modality as a diagnostic tool in FUO cases using the fluorodeoxyglucose (FDG) positron emission tomography (PET). FDG -PET has advantages because the site of inflammation, malignancy or infection can be localized in FUO patients. Image fusion combining PET and computed tomography facilitates anatomical location of increased FDG-uptake and so, better localization for further investigations to achieve the final diagnosis. The utility of FDG-PET in patients with FUO is growing and it will probably become the preferred diagnostic procedure in FUO patients.
Aim of the Study
To estimate the prevalence of connective tissue diseases among patients presented with FUO to the internal medicine department, Ain Shams University hospital, Cairo, Egypt.
Patients and Methods
Study Population
This observational study included 30 patients (Group 1), who presented with prolonged unexplained fever and fulfilled the clinical criteria of FUO according to the Petersdorf and Beason criteria (1961). They were selected and followed up either from the referred patients, to the outpatients’ clinic, by prolonged unexplained fever, or from the inpatients in the internal medicine department, Ain Shams University hospital, Cairo, Egypt in 2008. In addition 70 patient's were followed up who presented with prolonged fever with provisional diagnosis FUO in the previous two years (2006–2008) in the same hospital (Group 2).
Patients were Subjected to the following Diagnostic Work Up
Full history taking, thorough and repeated physical examination with recording of any clinical data: rash, jaundice, fever pattern, arthritis, lymphadenopathy and abdominal tenderness, etc.
Laboratory Assessment
7 ml of venous blood was withdrawn from each patient, it was divided in two test tubes one on EDTA anticoagulant for complete blood count (CBC), ESR and the other half was allowed to clot and serum was separated and used to do: full blood chemistry, including complete liver and kidney function tests; blood urea serum creatinine, aspartate amino transaminase (AST), alanine aminotransaminase (ALT) serum ferritin, C-reactive protein (CRP), anti nuclear antibodies (ANA) by immunoflurescence (IF) on Hep-2 cell line and anti-double stranded (DNA) by IF on Crithedia lucilia. In addition, complete urine analysis, urine and blood cultures were undertaken. Plain chest X ray and pelvi-abdominal ultrasound (US) were also performed. Depending on the potential diagnostic clues (PDC) present in every patient further diagnostic workup and/or procedures were performed: ascetic fluid culture, lymph node biopsy or sputum smear by Zehil-Nelseen stain. Serological tests were done to detect the specific antibodies in the sera by ELISA; Widal test and Brucella agglutination test, for cases suspected to have Typhoid or Multa fever respectively. Echocardiography when bacterial endocarditis is suspected. Barium enema/colonoscopy were performed if inflammatory bowel disease (IBD) was suspected.
Statistical Methods
Statistical analysis was done using statistical program for social science (SPSS) version 12. Description of quantitative variables was done as mean ± SD. Unpaired t-test was used to compare two quantitative variables in parametric data (SD < 50% of mean) and description of qualitative variables as number and percentage. A chi square test was used to compare qualitative variables between groups. One way ANOVA test was used to compare more than two groups as regard quantitative variables in parametric data (SD < 25% of mean). P value: >0.05 is non-significant (NS), P <0.05 is significant (S), P < 0.001 is highly significant (HS).
Results
The final diagnosis of patients presented with FUO was recorded, after statistical analysis the results were presented in five tables and four figures. This study included two groups:
Chi square test, showed non-significant difference regarding the percentage of different disease categories between both groups, (P > 0.05) (Table 1). Hence, both groups could be treated as a single group (n = 100). In 11 patients no definite causes of fever could be identified however, most of them showed spontaneous recovery.
Disease categories in all patients presented with FUO (n = 100).
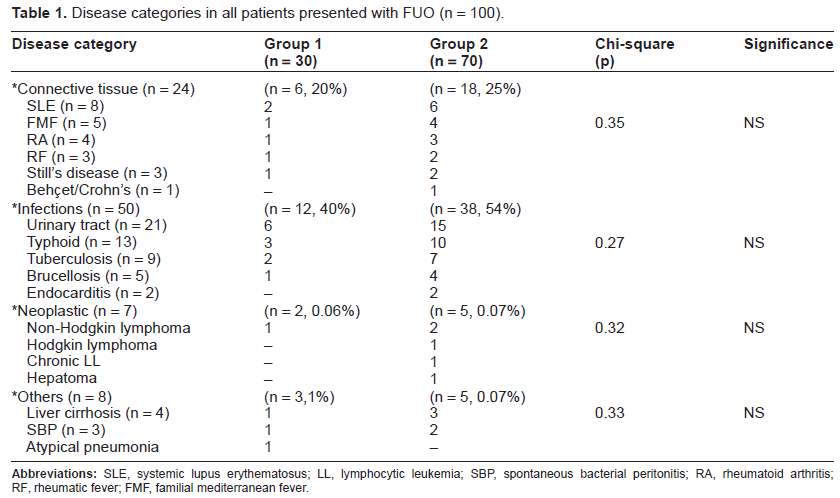
In all FUO patients (n = 100), 24% were found to have connective tissue diseases, 50% were found to have infectious diseases, 8% were found to have miscellaneous causes of FUO, 7% were found to have neoplastic diseases (Fig. 1). Chi-square test showed a statistically significant number of FUO patients having infectious diseases (P = 0.02). There was non-significant difference between both groups as regards the compared parameters (Table 2).

Pie chart represents the percentage of different disease categories presented with FUO.

Connective tissue patients presented with FUO in both groups.
Comparison between both groups of FUO patients by students t test.

There was a significantly higher percentage of patients who presented with intermittent fever patterns in the connective tissue group than in any other groups. Continuous fever pattern was significantly present in the infectious group. While, the unidentified pattern of fever was significantly encountered in the neoplastic group (Table 3 and Fig. 3).
Fever patterns in different disease categories of FUO patients.

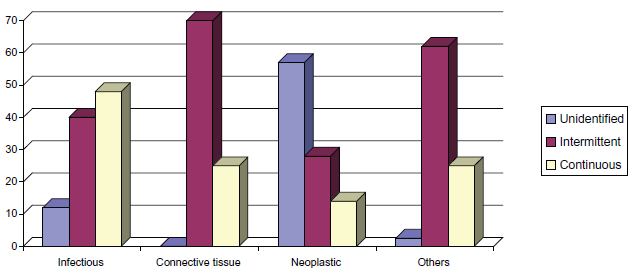
Fever patterns in different disease categories presented by FUO.
One way ANOVA test showed a statistically significant difference between different disease categories as regards these laboratory tests. Posthoc test was done to find the exact statistical significance between connective tissue group and other groups regarding test data (Table 4).
Comparison between different disease categories.

Out of the 24 CT patients (8,33.3%) were found to have SLE, (5, 20.8%) FMF, (4,16.6%) RA, (3,12.5%) for each of Still's disease and RF and (1,4%) was found to have Behçet/Crohn's disease. By Chi-square test (P < 0.05), (Fig. 4).

Pie chart for the percentage of CT patients presenting with FUO.
CT patients were generally found to have significantly higher ESR values than patients with infections, they were also found to have significantly lower CRP, C3 and TLC values than patients with infections and neoplasm respectively, (Table 5).
Posthoc test to find the statistical significance between CT group and other groups.

Discussion
Despite the recent advances in technology, FUO remains a diagnostic and therapeutic challenge even to expert physicians. In this study we were trying to find out the prevalence of connective tissue diseases in patients who presented with FUO. The diagnostic work up that best reaches the final diagnosis, step by step logistic approach, data collection and analysis, all were essential to reach the final diagnosis. Avoiding exhausting the patients with unnecessary investigations and invasive procedures should be always in mind.
In the present study the prevalence of patients presenting with FUO found to have connective tissue diseases was 24% (n = 6 ± 18). Collagen vascular diseases can manifest as FUO if the fever precedes the other more specific and localizing manifestations (arthritis, rash, nephritis, etc). We had eight patients with SLE who presented with FUO. SLE is a relatively common cause of FUO. 9 In this study; compared to patients with infectious fever, patients with SLE fever were more likely to have lower serum complement C3 level and a higher SLE disease activity index score. A prednisone dose of ≥45 mg daily was able to suppress SLE fever in our patients, usually within 2–3 days. In the present study the diagnosis of SLE patients was delayed due to lack of the specific diagnostic criteria as these patients were referred to our department from the fever hospitals after prolonged unexplained fever as a sole initial symptom. Familial mediterranean fever may present as FUO in patients of mediterranean descent, with recurrent febrile episodes at varying intervals associated with periodic abdominal pains is the commonest presentation due to peritonitis, pleurisy or arthralgias. 10 In this study we have 5 patients with FMF (20.8%) who presented with FUO. It was the diagnosis of exclusion as all of them were young females with long histories of recurrent abdominal pains and positive past history of appendectomy after which the periodic pains were still coming. Importantly, most of them denied any history of fever. They showed an excellent response to oral colchicine in a dose of 500 micrograms three times daily. Rheumatoid arthritis and systemic onset juvenile rheumatoid arthritis (JRA) [Still's disease] both may present with FUO. Still's disease is often difficult to diagnose; with a high spiking fever, non-pruritic rash that lasts less than 48 hours, myalgias, sore throat, high ESR and leukocytosis with mild elevation of liver enzymes all can lead the diagnosis towards infection thus the true diagnosis can be delayed. 11
In our study, the three patients with Still's disease (12.5%) were also referred undiagnosed from the fever hospital with, negative blood and urine cultures, negative ANA, DNA testing and Rheumatoid Factor (RF). No response of the fever to antibiotics in systemic onset JRA and adult onset still's disease lead to the diagnosis of exclusion. The four rheumatoid arthritis patients (16.6%) were presented mainly with systemic upset symptoms; prolonged fever and generalized body aches without localizing signs in the joints which was one of the presenting features in some RA patients. In agreement with the findings of Birch and Bhattacharya 12 our three patients with rheumatic fever, (12.5%) were found to have rheumatic carditis (however they were not complaining from any cardiac symptoms, it was diagnosed by ECG) and atypical fleeting arthralgias with limitation of movements in the affected joints rather than joints localizing signs. Crohn's disease is still the most common gastrointestinal cause of FUO. Diarrhea and other abdominal symptoms were lacking particularly in young adults. In the present study, we have one patient with Crohn's disease who presented with prolonged fever, anemia and weight loss. The diagnosis was delayed as the patient was already diagnosed as having Behçet's syndrome which was confirmed by endoscopy and biopsy.
In agreement with other studies,2,13,14 in the present study 50% of FUO patients were found to have infectious etiology; 21 patients (42%) were found to have complicated urinary tract infections [recurrent stones, congenital anomalies and uncontrolled diabetes], nine (18%) patients proved to have tuberculosis (TB), they were referred to the chest hospital, in five of them there was a history of old TB. This agrees with the reappearance of TB cases in other developing countries. They were found to have continuous fever pattern, toxemia and weight loss but the classical hemoptysis was absent. Typhoid fever was diagnosed in 13 patients (26%); 3 were found to have positive blood culture and 10 had positive titre by Widal test. The classical signs of typhoid (relative bradycardia in relation to fever and leukopenia) were not found in our typhoid patients. Five patients (1%) were found to have brucellosis. They were diagnosed by typical history, positive serology and a history of animal contact (all were butchers). Two patients (0.04%) were diagnosed as subacute infective endocarditis proved by echocardiography, one has prosthetic valve.
These were in agreement with the report of Edwin et al 13 , who examined 72 cases of FUO, they concluded that the three most frequent causes of FUO were; infections, neoplasm and connective tissue disorders. They added that the specific causes for FUO have varied through the years and in different locales. The three main classes have consistently been: tuberculosis, infective endocarditis, systemic lupus erythematosus and lymphomas/leukemia.
Ammari, 14 studied 52 patients with FUO in north Jordan reporting that infections were responsible for 26 cases (50%), malignancy for eight cases (15%), connective tissue disorders for six cases (12%) and others for 12 cases (23%). Infections remain the most common cause of FUO in Jordan, mainly tuberculosis, brucellosis and typhoid fever.
In the present study, the percentage of female patients who presented with FUO was significantly higher than males. The mean age was in the 3rd and 4th decades of life. This was different to the mean age in Edwin et al 13 which was in the 2nd and the 3rd decades of life. It is important to clarify that the percentage of connective tissue diseases in our cohort of FUO patients was 24% which was significantly higher than that of Ammari 14 (12%), or Edwin et al 13 (7%). While it was close to that found in the study of Salinas et al 15 in Mexico city (26%), they also reported that SLE is the main cause of FUO in the inflammatory non-infectious conditions.
Vander Schueren et al 16 had investigated 290 immunocompetent patients referred as FUO, in a unique report they found that the most prevalent diagnostic category was non-infectious inflammatory diseases (35.4%) of which (14%) were diagnosed as collagen vascular diseases: 5 SLE, 2 Takayasu's aortitis, 2 mixed connective tissue disease, one case each of ankylosing spondylitis, polyarthritis nodosa, sarcoidosis, granulomatous hepatitis and autoimmune hepatitis. They added that 98 FUO patients were discharged undiagnosed (33.8%) most of them were having episodic fever >38.3 °C. The fever remained obscure in 50 patients (47.6%) of 105 patients with episodic fever vs. 48 (25.9%) of 185 patients with continuous fever. Additionally, in eastern India Kejariwal et al 17 found that 11% of their 100 patients with FUO were due to collagen vascular diseases most of them were found to have SLE (5 cases).
In Saudi Arabia, Al-Qahtani 2 studied all admitted patients diagnosed as FUO between 1983–2008 (n = 273), she found that 41 patients (15%) were found to have different connective tissue diseases, 28 (68.3%) patients with SLE, 7 (17.1%) patients with mixed connective tissue, 4 (9.8%) with rheumatoid arthritis and 2 (4.9%) with polyarteritis nodosa. Additionally she reported 10 patients with sarcoidosis (55.5%), 2 patients with familial mediterranean fever and three patients with Crohn's disease (16.7%) but she didn't add them to the connective tissue group.
If they were added, the prevalence would be 56 cases (20%) which are close to our findings. Concurring with our results, she reported that infection is still the most common cause of FUO in Saudi Arabia (n = 106, 38.8%), neoplasm in 66 patients (24.2%), unidentified etiology in 42 patients (15.4%) tuberculosis and brucellosis ranked high among the infective causes; whiles lymphomas and leukemia in neoplasm, and SLE in the connective tissue group. In our study the intermittent fever pattern was significantly found in connective tissue patients, while patients with infections were found to have a continuous pattern of fever and those with neoplasia were found to have unidentified fever pattern. Indeed, it is difficult to have a meticulous fever chart for patients with FUO, as most of them were taking antipyretics on demand and having cold baths for their fever.
Connective tissue patients who presented with FUO were found to be of younger age group (28.04 ± 12.9) than FUO patients due to infection. They were found to have higher ESR values than patients due to infections except tuberculous patients, who were found to have significantly higher ESR values. FUO patients due to typhoid fever or tuberculosis were found to have an continuous fever pattern when compared to connective tissue patients who were mainly found to have an intermittent pattern. However, nowadays less importance is placed upon the pattern of fever as a diagnostic tool in FUO patients.
In Japan Goto et al 18 have described the characteristics and the outcomes for patients hospitalized with prolonged fever—not necessary fulfilling the FUO criteria—by reviewing the medical records in 226 consecutive patients, the majority of illnesses involved different infections (54%), non-infectious inflammatory diseases particularly adult onset Still's disease (n = 6), primary vasculitis syndromes (n = 5) and 3 cases of Behçet's disease were the leading cause of FUO (16/51, 31%).
Importantly, in patients with prolonged fever (who did not strictly meet the criteria in the definition of the classical FUO) there was a considerable number having critical illnesses. They concluded that strict use of the definition of FUO is thus unwarranted when managing patients with prolonged unexplained fever.
In Conclusion
FUO is still a challenging medical problem. Infections remain the most common cause in Egypt, confirming the trends found in other parts of the world, followed by connective tissue diseases and finally neoplasm. A keen clinical eye, meticulous history taking with repeated physical examinations and simple logistic laboratory tests are the most important diagnostic tools. Daily physical examination while the patient is hospitalized is essential. Pay special attention to rashes, new or changing cardiac murmurs, arthritis, abdominal tenderness or rigidity, lymph node enlargement and neurologic deficits. This was the cornerstone upon which the laboratory work up should be designed.
The increased prevalence of connective tissue diseases in patients presenting with FUO in Cairo, Egypt should be kept in mind and should raise the attention for early detection of the symptoms and signs of these diseases. Environmental pollutions, lifestyle modifications and other unidentified triggers may play a role in this increased prevalence.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.