
Abstract
Systemic lupus erythematosus (SLE) and related disorders are chronic inflammatory diseases characterized by abnormalities and, in some cases, even complete failure of immune responses as the underlying pathology. Although almost all connective tissue diseases and related disorders can be complicated by various neuropsychiatric syndromes, SLE is a typical connective tissue disease that can cause neurological and psychiatric syndromes. In this review, neuropsychiatric syndromes complicating connective tissue diseases, especially SLE are outlined, and pathological and other conditions that should be considered in the differential diagnosis are also discussed.
Introduction
Connective tissue diseases and related disorders are chronic inflammatory diseases characterized by abnormalities and, in some cases, even complete failure of immune responses as the underlying pathology. Originally, connective tissue diseases represented a group of disorders in which connective tissues, such as the joints, skin, muscle, and blood vessels, were the primary site of inflammation. Because infiltration of immune, inflammatory, and other cells may also cause inflammation and abnormal immune responses in neuron, nearly all connective tissue diseases and related disorders can be complicated by various neuropsychiatric syndromes. Systemic lupus erythematosus (SLE) is a typical connective tissue disease that can cause neurological and psychiatric syndromes. In this review, neuropsychiatric syndromes complicating connective tissue diseases, especially SLE (neuropsychiatric SLE [NPSLE]) are outlined, and pathological and other conditions that should be considered in the differential diagnosis are also discussed.
Pathology of NPSLE
NPSLE is etiologically classified as an angiopathy with syndromes ranging from those based on vascular inflammation, including necrotizing vasculitis, to those caused by the onset of vascular occlusion with thrombosis, based on antiphospholipid antibody syndrome (APS).1,2 However, according to anatomical, pathological, and other findings, necrotizing vasculitis cannot be necessarily proven to exist in the central nervous system (CNS) in many cases, but neuroimaging consistent with microvascular infarction are observed relatively often.3–5 Furthermore, there are also cases in which enhanced vascular permeability is suspected based on abnormal immune and inflammatory responses in the brain parenchyma. Focal syndromes are thought to more likely result from vascular lesions, whereas diffuse manifestations are more likely related to autoantibody- or cytokine-mediated impairment of neuronal function. Recent reports have clearly showed that N-methyl-D-aspartate (NMDA) receptor NR2 subunit on neuronal cells (anti-NR2 antibody) are associated with diffuse NPSLE, and cerebrospinal fluid (CSF) anti-NR2 is elevated in diffuse NPSLE when compared with that in focal NPSLE or in non-SLE controls.6,7 Furthermore, it was shown that IgG anti-NR2 antibodies stimulate the activation of endothelial cells, which may have a crucial role in the pathogenesis of NPSLE. 8 In addition, several cytokines would play a crucial role, in part, in the development of lupus-related neuropsychiatric syndrome, because certain repertoires of cytokines/chemokines are detectable in the CNS of NPSLE patients during active disease. In particular, the involvement of interleukin (IL)-6, interferon (IFN), IL-1, and tumor necrosis factor (TNF); certain antiinflammatory cytokines, including IL-10; and a number of chemokines such as fractalkine (CX3CL1), IP-10 (CXCL10), and MCP-1 (CCL2) in the pathogenesis of NPSLE have been extensively investigated.9–15 Schematic overview of the development of NPSLE is presented in Figure 1.

Schematic overview of the development of NPSLE. Either ischemia or activation/depression of neuronal cells may be a crucial component for NPSLE. The direct and indirect effects of several cytokines and chemokines on the CNS have been emphasized as possible contributors.
Classification of Neuropsychiatric syndromes
Neuropsychiatric syndromes in CNS
SLE is a typical autoimmune disease that can cause neurological and psychiatric syndromes. Because SLE can be complicated by almost all neuropsychiatric disorders, accurate classification and diagnosis are essential. In 1999, the American College of Rheumatology (ACR) issued new classification criteria for neuropsychiatric syndromes observed in SLE (Table 1), with reference to the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders. 16 Thus, the term NPSLE has been used in recent years. As described later, neuropsychiatric syndromes in SLE include those resulting from treatment, in other words, syndromes of steroid psychosis, and are also affected by infection, arteriosclerotic lesions. Thus, making an accurate differential diagnosis with exclusion of relevant disorders that might mimic SLE or have overlapping features is both fundamental and important. Myelopathy is also classified as a CNS disease in the NPSLE classification. 16 When syndromes, such as paraplegia, quadriplegia, sensory disturbance, and bladder and rectal disturbance, are observed during the course of SLE, transverse myelitis should be suspected. Moreover, myeloid angiopathy resulting from hypercoagulable tendencies, seen in APS and other conditions, is rare and also important as a cause of these symptoms. Myeloid angiopathy should be differentiated from multiple sclerosis and spinal lesions.
Prevalence of neuropsychiatric syndromes.

Neurologic syndromes in peripheral nervous system
Asymmetrical neurological syndromes, such as numbness and paresthesia mainly derived from mononeuritis multiplex, are observed. They reflect a disorder caused by ischemia of nervous tissue due to vasculitis, as typified by vasculitic syndromes including polyarteritis nodosa (PAN), antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis, and granulomatous angiitis. Moreover, peripheral neuropathy can also occur in Sjögren's syndrome (SS) regardless of the presence or absence of vasculitis.
Diagnosis of NPSLE
Because neuropsychiatric syndromes and syndromes complicating SLE are diverse, as indicated in Table 1, diagnosing NPSLE (CNS lupus) in actual clinical practice can be challenging. In other words, because headache, anxiety, mild depressive state, cognitive impairment, and other syndromes are commonly observed in association with aging, certain social circumstances, even without SLE. In addition, these neuropsychiatric symptoms may be influenced by infection, toxic metabolic condition, and drug-induced psychosis, especially induced by steroids, as described later. Therefore, it is often problematic to diagnose these syndromes as psychiatric features of SLE. Based on the new NPSLE classification criteria of the ACR, the recent reported incidences of each syndrome are shown in Table 1.17–20 Although these rates diverge slightly because of the differences in the sizes of facilities, regions, and methods of collecting cases (ie, a prospective study versus a retrospective study), the incidences of headache, mood disorder, cognitive impairment, and other syndromes are high in all reports. Moreover, in a study following 520 patients with SLE, Appenzeller et al reported that the incidence of NPSLE was 11.3%. 21 In patients with NPSLE, the complication rate at the time of onset was 3.7%, and an association with disease activity was noted. Moreover, patients who developed NPSLE during the follow-up period accounted for 7.7%. The disease onset was associated with positivity for antiphospholipid antibodies but not with either renal impairment or skin manifestations. 21
When a diagnosis is actually made in patients developing neuropsychiatric syndromes of some type during the course of SLE, it is important to assess the presence or absence of SLE activity, treatment state, and presence or absence of systemic complications. 22 In addition to routine immunological and serological tests, a CSF test, imaging studies (eg, computed tomography, magnetic resonance imaging [MRI], and single photon-emission computed tomography), and electroencephalography should be performed. The CSF test and brain MRI especially are essential for diagnosis because they allow the exclusion of local lesions, such as CNS infection and cerebrovascular disorder. 23 Moreover, it is common for SLE activity levels to not correspond with the onset and severity of CNS syndromes. This makes the diagnosis more difficult. Although antiribosome P antibody has been indicated to be also associated with the presence or activity of NPSLE,24–26 the results of a recent international meta-analysis of 1537 patients with SLE performed by Karassa et al found no strong association of this antibody with either the pathological condition or types of neuropsychiatric syndromes. 27 Taken together, it is crucial to accurately make a differential diagnosis of NPSLE using the serological and CSF examination and imaging studies as well as medical examination of neuropsychiatric syndromes, since the pathophysiology of NPSLE was very complicated and shows a wide diversity of clinical symptoms.
Important Differential Diagnosis: Steroid Psychosis
When psychiatric syndromes appear during the course of SLE, it is also often difficult to determine whether the syndromes are caused by SLE itself (NPSLE) or induced by steroids (steroid psychosis). In general, steroid psychosis is a psychiatric syndrome that newly appears after steroids are initiated or doses are increased in patients with SLE. When psychiatric syndromes are alleviated by reducing the steroid dose, steroid psychosis is confirmed. This form of psychosis manifests a few days after the initiation of steroid therapy in some patients and after a few weeks in others. Although there is no syndrome specific to this condition, many patients have mood disorders, such as manic or depressive states. 28
Chau and Mok, who analyzed 92 patients with SLE, reported that the incidence of steroid psychosis was 5%. 29 This rate is similar to that in patients receiving steroids for the treatment of not only SLE but also other conditions (5%). 30 In the previously described report on the follow-up and analysis of 520 patients with SLE, Appenzeller et al also reported that steroid psychosis was observed in 5.4% of their patients (28/520). 21 All 28 patients with SLE complicated by steroid psychosis were in the active disease stage, and their steroid doses at the time of steroid psychosis onset were high, ranging from 0.75 to 1 mg/kg body weight per day. Moreover, in all the patients, syndromes were alleviated in ∼13 days (median) after reducing the steroid dose. Interestingly, the statistical analysis revealed that hypoalbuminemia was significantly associated with the onset of steroid psychosis. Nishimura et al reported that IL-6 levels in the CSF are not elevated in most SLE patients with steroid psychosis and that IL-6 levels are useful for making the differential diagnosis. 31
Connective Tissue Diseases other than Sle Exhibiting Neuropsychiatric Syndromes
Although SLE and steroid psychosis are typical of diseases associated with neuropsychiatric syndromes, many other connective tissue disorders and related conditions produce disease-specific or nonspecific neurological syndromes.
Mixed connective tissue disease
Mixed connective tissue disease (MCTD) is a combination of certain features of SLE, myositis, and scleroderma and is characterized by positivity for other antibodies as well as anti-U1 ribonucleoprotein antibody. Although the development of serious CNS syndromes is rare, this disease may be complicated by trigeminal nerve disorder and aseptic meningitis.32,33 However, there are some interesting reports regarding NP syndromes in MCTD. According to a study on cognitive impairment in patients with SLE or MCTD using a combination of several types of cognitive function tests recommended by the ACR, cognitive impairment is apparently milder in patients with MCTD than in those with NPSLE. 34 Moreover, it has been demonstrated that, while 11 of 20 patients with MCTD had some CNS syndromes, 10 of 11 MCTD patients were found to meet the classification criteria for SLE in a follow-up study. 35 Thus, it is assumed that the concurrent development of CNS syndromes is rare in patients with genuine MCTD as described in many previous reports.
Rheumatoid arthritis
Common neurological syndromes that may appear in patients with rheumatoid arthritis (RA) or that can complicate RA are spinal cord disorders and peripheral neuropathy. Spinal lesions in RA lead to the development of spinal cord disorders or radicular syndromes because of atlantoaxial subluxation or deformity. 36 Moreover, strangulated neuropathy due to joint deformity and inflammation of the joints or thecal tissues is also common. In rheumatoid vasculitis due to concurrent vasculitis, mononeuropathy multiplex develops as with other types of vasculitis.
Regarding associations with therapeutic agents, peripheral neuropathies, such as Guillain–Barre syndrome 37 and chronic inflammatory polyradiculoneuritis, have been reported during administration of TNF inhibitors, which are biological agents. 38 When peripheral neuropathy develops concurrently during the stable stage of RA activity or inflammation, drug-induced conditions must also be considered.
Sjögren's syndrome
It is also common for SS to be complicated by many organ-specific or nonspecific autoimmune diseases. Neuropathy, at a relatively high incidence, is of the sensory type not accompanied by dyskinesia, and ganglionopathy is also pathologically observed in addition to vasculitis.39,40 Moreover, CNS lesions, such as those of the localized (eg, motor nerve paralysis and ataxia) and diffuse (eg, encephalopathy and dementia) types, are also observed in at least 20% of patients. Because the syndromes and natural history of these lesions are very similar in some patients, the differential diagnosis needs to focus on whether patients have SS alone or SS complicated by other diseases.41,42 In SS, memory disturbance has also been documented. In a report examining memory retention (Wechsler Memory Scale and Tactual Performance Test) in 66 patients with primary SS and controls matched for age and sex, memory disturbance was significantly more frequent in patients with primary SS. 43 Interestingly, this report describes the hippocampi as being significantly smaller when diagnosed with brain MRI in patients with SS, and their syndromes were found to be associated with the presence of anti-NR2 antibody in the CSF. 43 Although neuropsychiatric syndromes such as depression, anxiety, and mild cognitive dysfunction and also complaints of fatigue and myalgia have been seen in patients with SS, the etiology and course of these syndromes including depression, anxiety, and cognitive impairment have not been fully elucidated. The influence of fibromyalgia in some patients with SS is recognized, because similar syndromes seen in SS are frequently reported by patients with fibromyalgia and the association of SS and fibromyalgia has been observed.44,45
Behçet's disease
Behçet's disease (BD) is a systemic inflammatory disease characterized by recurrent oral aphthous ulcers, genital ulcers, skin manifestations, such as erythema nodosum and folliculitis-like eruption, and ocular manifestations typified by iridocyclitis and uveitis. 46 In ∼10% of BD cases, a specific CNS lesion (neuro-BD) may develop. 47 It more frequently occurs in males and patients positive for human leukocyte antigen (HLA)-B51. 48 According to pathological conditions, BD (CNS involvement) is classified into lesions showing inflammatory changes of the brain parenchyma (especially the brainstem and basal nuclei; 66%), lesions resulting from vasculitis and superior sagittal sinus thrombosis at a rather low frequency (29%), and other lesions.46,47 Neuro-BD is broadly divided into acute and chronic progressive types. The acute type occurs relatively acutely and causes headache and other meningitis-like syndromes, as well as cranial neuropathy, hemiplegia, and convulsion, while the chronic progressive type produces neuropsychiatric syndromes such as cognitive impairment, dementia, and ataxia, which gradually progresses, is resistant to treatment, and even causes deterioration of personality.49,50 Brain MRI reveals abnormal signal intensity in the cerebral white matter, basal nuclei, and brainstem (mesencephalon and pons) on T2-weighted images. In the chronic progressive type especially, atrophy of the brainstem is observed significantly more often than in other forms. 50 Moreover, because cyclosporine A, which may be administered to treat refractory pathological conditions such as the ocular manifestations, may cause CNS syndromes of the acute type, caution is necessary when diagnosing and managing this disorder. 51
Systemic vasculitis
In cases with almost (of most) systemic vasculitis, basically excluding primary angiitis of the CNS (PACNS) as described in the following section, peripheral neurological syndromes (mononeuritis multiplex) are common and can even be the initial syndromes.
Primary angiitis of the CNS
PACNS is a rare angiitis affecting mainly CNS blood vessels and was formerly referred to as granulomatous angiitis of the CNS.52,53 Because lesions of other systemic diseases, especially systemic vasculitis, SLE, lymphoma, and intracerebral infection, affect CNS blood vessels, as described later, differential diagnosis is important. According to a report summarizing five cases with PACNS diagnosed by biopsy of the brain parenchyma, the patients presented with headache and motor neuron disorders, as well as convulsion-like syndromes and impaired consciousness. 54 MRI revealed abnormal signal intensity on T2-weighted images in all cases. A brain tissue biopsy including the pia mater frequently reveals segmental granulomatous angiitis, and necrotizing vasculitis is detectable in some cases.53,55
Giant cell arteritis
Giant cell arteritis (GCA) is a form of vasculitis that involves the carotid arteries and their relatively large arterial branches, especially the temporal arteries. 56 As to the affected arteries, lesions are likely to develop in the ophthalmic artery, which is described later, posterior ciliary artery, vertebral artery, aorta, and so on, in addition to the temporal arteries, whereas the internal carotid artery and intracranial arteries are rarely affected by these lesions. With this form of angiitis, a painful pulsatile node (representing a damaged blood vessel) is palpable in the temporal area. Pathologically, the internal elastic lamina of the arterial wall undergoes destruction, and a granuloma containing multinucleated giant cells thereby forms. In ∼25% of cases, GCA may be complicated by visual impairment due to ischemia of the ophthalmic artery or its arterial branch and requires intensive care. Moreover, transient ischemic attack, cerebral infarction, and other neurological syndromes occur at frequencies that vary among reports (range: 2.5%–25%). 57 As for psychiatric syndromes, depressive state, psychosis, dementia, and various other syndromes have been clinically recognized.
Polyarteritis nodosa
PAN is a disease that causes necrotizing vasculitis in medium- to small-sized arteries throughout the body and produces various syndromes. 58 Necrotizing vasculitis, which is the main feature of the PAN lesion, is characterized by various degrees of fibrinoid degeneration and necrosis. Pagnoux et al, who retrospectively analyzed 348 patients diagnosed as having PAN during or after 1963, reported that 79% presented with concurrent neurological syndromes, of which mononeuropathy multiplex was the most common. 59 The incidence of CNS disorders in PAN cases is often reported to be 4%–8%.59,60 Infarction of the CNS in PAN cases is speculated to result from arteriolar occlusion caused by necrotizing vasculitis. Furthermore, hemorrhage is assumed to be attributable to rupture or tearing of a cerebral aneurysm associated with vasculitis. IL-6 levels in the CSF are also reportedly increased during the active stage of CNS lesions in patients with PAN. 61
ANCA-associated vasculitis
ANCA-associated vasculitis (AAV) is classified into microscopic polyangiitis (MPA), granulomatosis with polyangiitis (GPA; previously referred to as Wegener granulomatosis [WG]), and eosinophilic granulomatosis with polyangiitis (EGPA; previously referred to as allergic granulomatosis with polyangiitis or Churg-Strauss syndrome). 62 These types of vasculitis are likely to have systemic syndromes because mainly arterioles and capillaries are affected. As for neurological syndromes, peripheral neuropathy, especially mononeuropathy multiplex that produces numbness, motor paralysis, and other syndromes, develops. 63 In a recent report from a multicenter cohort of patients with EGPA, ANCA-positive patients exhibited more severe disease with mononeuritis as well as renal involvement. 64
Conversely, when mononeuropathy multiplex is observed in patients with systemic inflammatory conditions (eg, fever and high C-reactive protein level), systemic vasculitis typified by AAV should be considered. CNS lesions are characterized differently according to each of these disease types.
The rates of GPA complicated by CNS lesions vary among reports, ranging from 11% to 50%.65–67 Moreover, in an analysis of 324 patients with WG (GPA), the observed CNS syndromes included cranial nerve paralysis (6.5%), eye movement disorders (4.9%), cerebrovascular disease (4%), and convulsive seizure (3.1%). 68 Because WG mainly affects small blood vessels, abnormalities are difficult to detect even with intracranial angiography. However, abnormal MRI findings are often seen in the brainstem and cerebral hemisphere white matter. 69 The pathogenic mechanism underlying neurological syndromes is presumably direct invasion of granulomatous lesions or vasculitis. However, because there are also reports describing patients with concurrent diffuse or localized thickening of the dura mater (hypertrophic pachymeningitis [HP]), which is described later, 70 there are patients positive for myeloperoxidase or proteinase 3-ANCA with HP accompanied by upper respiratory lesions or granulomatous formation, overlapping pathologies may well exist in these patients.
In MPA, unlike GPA, the rate of concurrent CNS lesions has long been regarded as being relatively low. However, neither disorder is as rare as formerly assumed. It is assumed that the incidence of such complications might be affected by the differences in the mechanisms affecting psychiatric and neurological disorders, in other words, the size and distribution of invading blood vessels. Thus, even in MPA, it is not rare for patients to concurrently develop CNS syndromes or CNS vasculitis, and the brain also needs to be examined. In EGPA, CNS complications are basically rare but do manifest as eosinophilic vasculitis of the cerebral blood vessels in 6%–7% of patients.71,72 The major CNS syndromes are due to cerebral vascular insufficiency resulting from vasculitis (eg, cerebral infarction, impaired consciousness, and convulsion). Furthermore, spinal cord disorders due to eosinophilic vasculitis are rare but have also been reported. 73
Hypertrophic pachymeningitis
HP is an inflammatory lesion of the intracranial or intraspinal dura mater that leads to various cranial nerve disorders, cerebellar syndromes, myelopathy, and other conditions because of marked thickening of the dura mater. While HP is divided into idiopathic and secondary types, an important causative disorder of secondary HP is the vasculitis typified by GPA (WG). 70 At present, the diagnosis is not relatively difficult to make because of recent advances in MRI technology. The common clinical syndromes include headache, cranial nerve paralysis, cerebellar ataxia, and convulsion. Chronic and daily headaches (migraines in many cases) are common. Cranial nerve paralysis involves several nerves, while paralysis of cranial nerves II, V, VI, VII, VIII, and XII is especially common. MRI depicts the lesions as hypointense or isointense signal areas on T1-weighted images and generally as hyperintense signal areas on T2-weighted images, while gadolinium-enhanced MRI shows marked enhancement (linear or nodular enhancement) on T1-weighted images. 74
Related Important Pathological Conditions during Treatment and Follow-up of Connective Tissue Diseases
Thrombotic thrombocytopenic purpura
Thrombotic thrombocytopenic purpura (TTP) is a disease included in the concept of thrombotic microangiopathy (TMA) along with hemolytic uremic syndrome (HUS) and other diseases. TTP is a serious pathological condition in which thrombus formation due to platelet aggregation frequently occurs mainly in microvessels, leading to ischemia of important organs. 75 The occurrence of this disease is associated with decreased activity of a disintegrin-like and metalloproteinase with thrombospondin type 1 motifs 13 (ADAMTS13), an enzyme that cleaves ultrahigh-molecular-weight von Willebrand factor polymers and controls their molecular weight. 76 In TTP complicating autoimmune diseases such as SLE, most of the cases has decreased ADAMTS13 levels. 77 Furthermore, the case showing diminished ADAMTS13 activity in patients with adult-onset Still's disease was reported. 78 In addition to thrombosis, the clinical syndromes include fever, hemolytic anemia, renal dysfunction, and psychiatric manifestations. The neuropsychiatric syndromes include impaired consciousness (cloudiness and confusion), mood changes, personality changes, and headaches, which are characteristically often reversible and fluctuate during the day depending on the degree of vascular insufficiency. In cases with SLE complicated by APS (especially the fulminant type), systemic thrombosis may occur, while psychiatric manifestations, renal dysfunction, hemolytic anemia, and other syndromes may appear as features of the SLE itself. Thus, whether these syndromes are attributable to SLE alone or concurrent TTP is a significant clinical issue in some patients. However, because psychiatric syndromes of TTP are clinically characterized by variability or daily fluctuation, it is assumed that TTP can be differentiated from NPSLE and other diseases. In addition to treatment of the primary disease, it is important to perform plasmapheresis in the early stage.
Progressive multifocal leukoencephalopathy
Progressive multifocal leukoencephalopathy (PML) is a disease in which multiple demyelination of the CNS, especially the white matter, is caused by late-onset infection with the Jakob–Creutzfeldt (JC) virus, a DNA virus. While the majority of affected patients have acquired immunodeficiency syndrome, PML occasionally occurs in patients with a similar immunodeficient condition. According to an analysis of 34 patients with connective tissue diseases who developed PML, the PML was caused by administration of rituximab (anti-cluster of differentiation [CD] 20 antibody) to patients with SLE or RA, and caution is thus required when administering such biological agents. 79 Furthermore, a search of a database listing >2 million patients with autoimmune diseases (ie, RA, psoriasis, pediatric inflammatory arthritis, inflammatory bowel disease, and ankylosing spondylitis) across the United States identified 53 patients who had developed PML. Although many patients were infected with the human immunodeficiency virus or had malignant tumors as underlying diseases, nine patients had received rituximab or other biological agents before the onset. 80 This report describes the incidence of PML as 0.2 per 100,000 patients with autoimmune diseases. The virus asymptomatically infects the host in childhood, and then remains latent. When immunosuppressive therapy is administered, the virus is reactivated and becomes detectable. Then, it specifically infects oligodendrocytes in the CNS, leading to irreversible progression of demyelination of the nerve tissue. The syndromes that appear to reflect the demyelination site are hemiplegia, visual disturbance, aphasia, and cognitive impairment. MRI shows many hypointense areas on T1-weighted images and hyperintense areas on T2-weighted and fluid-attenuated inversion recovery images in the subcortical white matter. Although antiviral agents and other drugs are administered for treatment, the prognosis remains poor. Early detection and early treatment are crucial. Whenever patients treated with immunosuppressive, biological, or other agents develop CNS syndromes of any type, it is important to suspect the concurrent development of this disease.
Conclusions
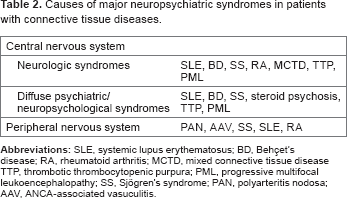
Neuropsychiatric syndromes observed in patients with connective tissue diseases and related disorders are diverse, and many cases have no characteristic syndrome specific to one of these diseases. The major neuropsychiatric syndromes and the possible causative diseases are summarized in Table 2. As seen in NPSLE, there are also diseases in which the presence of neuropsychiatric syndromes is an important diagnostic criterion for the primary disease. Thus, accurate assessment is required to differentiate whether the syndromes are associated with the disease itself, pathological conditions attributable to infection, aging, and the like, or are neuropsychiatric syndromes caused by therapeutic agents. Furthermore, because there are also pathological conditions that can greatly affect both prognosis and quality of life, early diagnosis and therapeutic interventions are always important.
Causes of major neuropsychiatric syndromes in patients with connective tissue diseases.
Author Contributions
Conceived and designed the experiments: TK, AM, NO. Analyzed the data: TK. Wrote the first draft of the manuscript: TK. Contributed to the writing of the manuscript: TK. Agree with manuscript results and conclusions: TK, AM, NO. Jointly developed the structure and arguments for the paper: TK, AM, NO. Made critical revisions and approved final version: TK, AM, NO. All authors reviewed and approved of the final manuscript.