
Abstract
Objective
Barriers to medical care may influence health status. It is unclear whether problems with access can predict clinical outcomes in lupus. This study aimed to determine whether care barriers are associated with increased disease activity and damage in a multi-center, multiethnic SLE cohort. We also compared concordance between care barriers as reported by the patient and lupus specialist.
Methods
Data from SLE patients in 12 Canadian centers collected at annual visits, including demographics, treatment, disease activity and damage were analyzed.
Results
654 patients were enrolled with ethnic groups being Caucasian [CC] (64%), Aboriginal [ABO] (9%), Asian [AS] (21%), and Black [BLK] (6%). 50.8% had at least one barrier to care including travel to a rheumatologist (32.0%), waiting to see a rheumatologist and cost of medications. Access to medication and costs were significantly associated with co-morbidity (p < 0.001, p = 0.04). There were significant associations between ethnicity and any physician perceived care barrier < p < 0.001), mostly in Aboriginal. Doctors identified half of patients who had access to medication problems (p = 0.003) and the relationship between doctors and patients identifying similar care barriers was weak (r = 0.09). A lower total household income significantly predicted the presence of any care barrier (p < 0.001).
Conclusions
Despite access to a lupus specialist many care barriers were identified, although we found few associations between care barriers and patient outcomes. The cost of medication was related to SLE disease activity; however, we cannot determine if this was cause or effect. Care barriers identified by lupus patients are significantly underestimated by physicians.
Keywords
Introduction
Access to healthcare is a social determinant of health and an important public health issue. Availability of subspecialty services can be a challenge due to physician shortages, wait times, clinic locations, and costs associated with medications or clinic visits. Systemic Lupus Erythematosus (SLE/lupus), a chronic multi-system autoimmune disease, requires ongoing assessment and treatment. While the importance of access to care and its health effects in SLE is not well defined in the literature, it has been hypothesized that barriers to rheumatology care may be associated with poorer health outcomes in SLE. 1 The benefits of specialty care have been well documented for rheumatoid arthritis (RA): when a rheumatologist was identified as the primary treating physician, patients reported improved functional status, number of painful joints, overall pain rating, and global assessment. 2 Measures of access to care have varied widely between studies in SLE. Early treatment and more frequent follow-up visits were hypothesized to contribute to improved survival in SLE. 3 A perceived difficulty in obtaining healthcare was more frequently reported by SLE patients who subsequently died (21.4%) compared to surviving patients (3.8%, p = 0.002) within the first five years of the LUMINA longitudinal study. 4 Non-adherence, which impacts medication use and follow-up visits, has been associated with higher rates of emergency room visits, hospitalizations and renal failure in lupus patients.5,6
Analyses of other access factors have provided inconsistent results. For example, Karlson et al. did not find that indicators of access (health insurance at diagnosis or distance to the physician's office), predicted SLE outcomes. 7 On the other hand, Ward examined lupus nephritis patients starting renal replacement therapy and found that private medical insurance correlated with later age of onset of end stage renal disease, arguing the difference may be mediated by better access or quality of care. 8
The influence of ethnicity on access to care in SLE has also been investigated. A review of Medicare claims in 3 U.S. states noted that elderly African American patients with SLE visited a rheumatologist less often than their Caucasian counterparts. 9 They surmised that if medical care by a rheumatologist improves SLE health status, improving subspecialty access in ethnic minorities could enhance patient outcomes.
Our study aimed to determine whether patient and physician identified care barriers are associated with increased disease activity and damage in a prospective, multi-center, multiethnic Canadian SLE cohort. Universal healthcare in Canada provides a unique setting for our investigation by minimizing effects of income on access. A related objective was to identify any differences in obstacles to care between ethnic groups. We also compared concordance between care barriers as reported by the patient and the specialist. Finally, we examined what factors (i.e. socioeconomic status (SES), ethnicity, activity and damage) were associated with care barriers.
Methods
Study Population and protocol
The 1000 Canadian Faces of Lupus is a prospective multi-center cohort study of patients with a clinical diagnosis of SLE (meeting the American College of Rheumatology [ACR] criteria). 10 The goal of the cohort is to establish a long-term national lupus cohort to research lupus in a Canadian context including the interaction of patient characteristics on the course and outcome of SLE. Recruitment began in July 2005 and included both incident and prevalent cases presenting at the 14 participating centers across Canada. Study visits, which occurred at cohort entry and on an annual basis, consisted of an interview, physical exam and laboratory tests. Both investigator and participants completed data forms.
Data collection covers the following areas: demographics, disease manifestations/activity, disease damage and co-morbidity, health related behaviors and health related quality of life (using the Short-Form 36 [SF36]). Demographic information includes age, gender, ethnicity, occupation, income, education, smoking and alcohol use. Data on disease manifestations include clinical (ACR criteria, disease onset/duration, other disease manifestations and medication use) and laboratory information (autoantibodies collected annually include antinuclear antibodies, antibodies to double-stranded DNA and extractable nuclear antigens, and antiphospholipid antibodies).
Disease activity was assessed by the SLAM-R (revised SLE activity measure) 11 and the SLEDAI-2K (SLE disease activity index 2K). 12 These indices score lupus manifestations within the major organ systems. Cumulative end organ damage was measured with the Systemic lupus international collaborating clinics/ACR damage index (SLICC). 13 The Charlson Index was used to measure co-morbidity; here 22 co-morbid conditions are assigned a score. A greater score means a more severe illness burden with increased one-year mortality. 14
Access to healthcare was investigated from both the patient and physician perspectives. Patients completed self-report questionnaires about community access (availability of local family doctor or nursing station) and physician access (regular family doctor/rheumatologist, travel distance/time). Patient care barriers were measured on 5 dimensions: cost of medications, access to medications (such as ability to obtain a prescription, and lack of government drug coverage for “off label” indications), travel to rheumatologist's office, waiting to see a rheumatologist, and cost of medical devices. Each dimension had three possible responses of 0 (no problem), 1 (a bit of a problem) and 2 (a significant problem).
Physician reported care barriers were also divided into 5 dimensions: language barrier, missed visits (due to weather/travel), clinic visit non-attendance (“no shows”), access to medications and non-adherence with medications. Barriers affecting patient care over the past year were rated by the physician on a similar three-point scale identical to the patient reported scale from 0 to 2.
Statistical analyses
Healthcare access variables that were identified to be a problem in >5% were included in subsequent analyses using SPSS Version 15 (SPSS Inc, Chicago, IL, U.S.A). The scores for each care barrier were recoded into binary variables (0 = no problem, 1 = a problem). As well, we created binary variables for any care barrier (patient and physician perceived), any patient perceived care barrier and any physician perceived care barrier. To investigate the differences in access between ethnic groups, Mantel-Henzel testing was performed. Using univariate analysis, we attempted to identify care barriers that were associated with SLE outcome (SLAM, SLEDAI, SLICC) within the multiethnic cohort and then within the Caucasian group only. Multivariate regression analysis was used to detect relationships between access variables and SLE activity/damage with models adjusting for age, income and ethnicity. Logistic regression modeling was done to determine whether ethnicity, SES (socioeconomic status) or damage was significantly related to any care barrier. Pearson correlations were used to determine if there was a relationship between patient and physician perceived care barriers. Linear regression models determined associations between care barriers and the Charlson Index, SLEDAI, SLAM and SLICC scores.
Results
One thousand five hundred and eight patients have been enrolled since July 2005 at 14 sites, but not all sites are currently completing the care barriers case report form. For 614/1508 patients from 2 sites, no information on care barriers was available. The majority of patients belonged to one of four ethnic groups: Aboriginal, Asian, Black or Caucasian. An additional 240 patients had missing data on ethnicity, or belonged to an ethnic group other than the 4 of interest, and were excluded from analysis. A total of 654 patients from 12 sites completed the healthcare barriers questionnaire including Caucasian (CC) (64%), Asian (AS) (21%), Aboriginal (ABO) (9%) and Black (BK) (6%). Baseline demographics of the cohort are presented in Table 1.
Baseline demographics of SLE patients who completed care barrier forms.
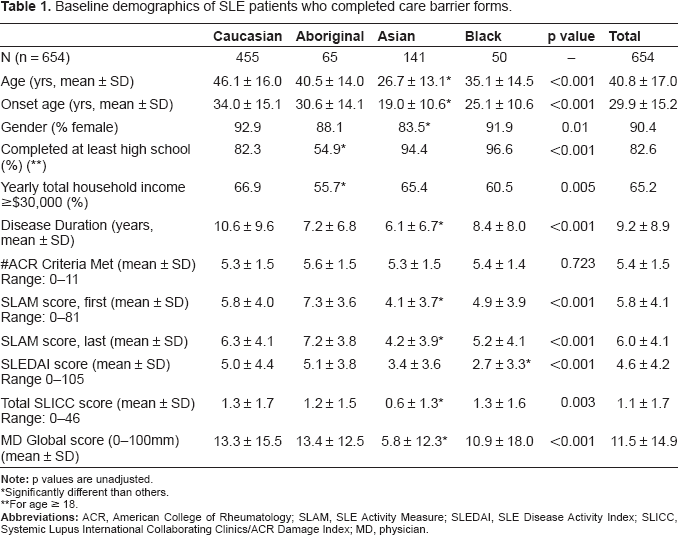
Significantly different than others.
For age ≥ 18.
We found that 88.5% of our cohort had access to a general practitioner (GP) in their community, 80.4% had a GP who they saw regularly, and 92.5% had a regular rheumatologist but 55.4% were traveling to another community to see their rheumatologist. These statistics did not differ much by ethnicity.
Table 2 demonstrates the presence of care barriers amongst a large percentage of our patients from both the patient and physician's point of view. Just over half (50.8%) of the patients perceived a care barrier despite ‘universal’ healthcare in Canada; 27.5% found cost of medication as a barrier to care, 19.6% reported waiting to see a rheumatologist as a barrier, 32% reported traveling to a rheumatologist's office as a barrier, 7.6% reported access to medication as a barrier and 8.6% reported cost of medical devices as a problem.
Percentage of SLE patients with care barriers.

We compared ethnic differences on three patient perceived care barriers: cost of medication, travel to a rheumatologist's office and waiting to see a rheumatologist, as well as on any care barrier and any physician or patient reported care barrier. We found a significant difference (p < 0.001) between ethnicities for any physician perceived care barrier where physicians reported barriers to care in 21% of their Aboriginal patients compared to only 2.6% of their Black patients. There were no ethnic differences in any other category (Table 3).
Percentage of SLE patients with care barriers by ethnicity.

Significantly different than others.
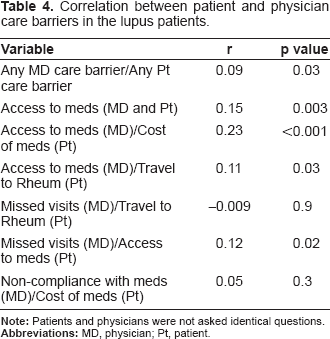
While 50.8% of our patients experienced one or more barriers to care, physicians reported a low frequency of barriers (only 9.8% of patients). Language was seen as a barrier by physicians for only 5.7% of patients, in spite of the high frequency of visible minority patients, but all patients enrolled in this study signed informed consent in either English or French, so language barriers would have been mostly removed from patients entering the study. Missed clinic visits (due to weather or travel disruptions) and non-attendance at clinic visits were reported as a physician perceived barrier in 2.5% and 4.2% of patients, respectively, while physicians reported difficulty in accessing medications for 4.4% of patients, as well as non-adherence with medications in 4.4% of patients. Overall, any patient and any physician perceived care barriers were significantly, but weakly, correlated (r = 0.09, p = 0.025), as were physician and patients’ perceptions of access to medication as a barrier (r = 0.25, p = 0.003) and physician perceived access to medication as a barrier and patient perceived cost of medications (r = 0.23, p < 0.0001). We did not find a significant correlation between physician perception of missed visits and patient perception of traveling to the rheumatologist, nor between non-adherence with medication from the physician's perspective with cost of medication as a care barrier from the patient's perspective. In general, the relationship between doctors and patients identifying most care barriers was not strong (Table 4).
Correlation between patient and physician care barriers in the lupus patients.
Ethnicity and damage were not associated with the presence of any care barrier (data not shown). Total yearly household income was inversely associated with the presence of any care barrier (B = –0.11; p < 0.001), while there was no strong association between education and the presence of any care barrier (data not shown).
In spite of the numerous barriers to care identified by both patients and physicians as described, however, we found few associations between barriers and patient outcomes. We observed that only patient perceived access to medication and cost of medical devices were significantly related to the Charlson Index, whereas physician perceived access to medications was associated with the SLEDAI score and cost of medications and physician perceived access to medication as barriers were associated with the SLAM score (p = 0.04 and 0.001 respectively) (Tables 5 and 6).
Care barriers associated with disease activity.

Statistically significant.
Care barriers associated with damage and co-morbidity.

Statistically significant.
Discussion
Our results show that barriers to care occur even in a publicly funded healthcare system. Our cohort is biased in favor of access as the patients have been referred to and are followed by a lupus specialist, they are seen regularly and they have agreed to enter a cohort study. However, notwithstanding that all study patients had equal hospital/physician access (tax funded universal healthcare) and were already followed by a rheumatologist by virtue of the study design, we found identifiable barriers. In addition, despite universal healthcare in Canada, most patients do not have their medications paid for by the government, nor does every patient have a private drug plan.
Despite a best case scenario for lupus patients to have few barriers, we found important barriers which were related to lupus activity and co-morbidity, but not damage as measured by the SLICC. SLE damage may not have an effect on current care barriers (but could be related to disease activity, severity and other morbidity in the past, which was not part of the scope of this study in patients with prevalent lupus). Patients with lower incomes (despite universal healthcare) still struggle more with the added costs of their disease, demonstrating the far reaching impact of chronic disease in patients’ lives.
Physician perception of barriers to care was significantly related to patient barriers, but there was still a discrepancy between physician and patient reporting of care barriers. Physicians may be unaware of some important barriers to care and this could impact health as demonstrated in our results where care barriers were related to lupus activity. Also, when discussing care barriers the perspective (patient or doctor) could alter the results.
Other studies have found non-adherence with medications or clinic attendance to result in increased damage and worse outcomes. 15 Similarly, difficulty accessing medications, due to unavailability through insurance or inability to afford the medications on the part of the patient, could certainly result in worse outcomes due to under-treatment. Certainly health insurance status has been associated with worse outcomes in other SLE studies.15–23 This analysis is limited in its conclusions because it is cross-sectional; we cannot comment on a cause and effect relationship between disease activity, outcomes and barriers to healthcare. Prospective data are being collected to look for barriers that are predictive of SLE outcomes.
In conclusion, care barriers occur in more than half of the lupus patients who have a specialist. The presence of at least one carrier barrier did not differ statistically by ethnicity (but was highest in Aboriginals and lowest in Asians within Canada). The lupus patients frequently identify barriers even in a system of universal healthcare and these barriers are often underestimated by their treating physicians. Barriers are higher in those with lower total household incomes.
Disclosure
The authors report no conflicts of interest.
Footnotes
Acknowledgments
We would like to thank The Arthritis Society, Lupus Canada, Ontario Lupus Association and Lupus Ontario for providing funding for this study. This study was funded by The Arthritis Society, Lupus Canada, Ontario Lupus Association and Lupus Ontario.