
Abstract
This study describes knee alignment and active knee range of motion (ROM) in a community-based group of 78-year old adults (n = 143) who did not have radiographic evidence of knee osteoarthritis in either knee (KL < 2). Although knee malalignment is a risk factor for knee osteoarthritis, most women and men had either valgus or varus alignments. Notably, no men were valgus in both knees. Women with both knees valgus had significantly greater body mass index (
Introduction
Osteoarthritis (OA), the most common form of arthritis, affects approximately 27 million American adults 1 and is the 4th leading cause of non-fatal disability in adults worldwide. 2 Knee OA, the most common form of osteoarthritis, affects an estimated 250 million people worldwide and can severely limit mobility. 3
Despite of the prevalence of knee OA, not everyone is affected. As individuals enter their 70s, the incidence and progression of knee OA reaches a plateau and starts to decline.4,5 There are few studies of elderly unaffected individuals. A broader understanding of the elderly without knee OA may lead to the identification of possible protective factors for knee OA, a better understanding of OA incidence and progression, and a reduction in the overall incidence and severity of knee osteoarthritis.
In addition to age, gender, and body mass index (BMI), two other risk factors often associated with knee OA are knee malalignment6,7 and decreased knee range of motion (ROM).8,9 Knee malalignment (varus or ‘bowlegged’ and valgus or ‘knock kneed’) affects knee joint loading and can increase the risk of cartilage damage and the risk for development and progression of knee OA. 10 Information supporting a relationship between adult knee alignment and the development of knee OA is limited. 11 Brouwer et al. 6 reported an association in older adults between varus (OR = 1.54) and valgus (OR = 2.06) alignments and increased risk of incident radiographic knee osteoarthritis. Sharma et al. 10 reported an increased risk of incident radiographic knee OA with varus (OR = 1.49), but not valgus (OR = 0.87) alignment. Felson et al. 12 reported an adjusted odds ratio (OR) of 2.5 between valgus (>3.1°) knees and the risk of incident knee OA in older adults (50–79 years). In contrast, Hunter et al. 7 found no association between varus or valgus knee alignment and incident knee OA in 52–55 year-old participants, suggesting that the presence of malalignment in healthy knees is likely not sufficient to initiate the OA disease process.
Obesity and knee malalignment are recognized as important risk factors for the development of knee OA.
13
Niu et al.
14
reported a significantly increased risk for incident radiographic knee OA for obese (BMI ≥ 25 and <35) and very obese (BMI ≥ 35) adults (50–79 years) regardless of baseline knee alignment. Brouwer et al.
6
reported a statistically significant increased risk for incident radiographic knee OA in obese adults with varus alignment (
Reduced knee range of motion is often present in individuals with knee OA. Liikavainio et al.
15
compared knee range of motion (flexion and extension) in two groups of 51- to 67-year old men with and without knee OA. They reported significantly reduced (
Few studies have specifically described knee alignment or range of motion in men or women over the age of 75 and fewer have described those without knee osteoarthritis. This study provides information on knee alignment and knee range of motion by gender in 78-year-old participants without radiographic knee osteoarthritis. We considered radiographic and physical exam determinations of adult knee alignment in combination with recalled childhood knee alignment, as well as BMI in conjunction with radiographic knee alignment and knee ROM.
Methods
Study Participants
This study examined knee alignment and knee range of motion for 143 participants who were 78 years old and did not have radiographic signs of knee OA. The study group participants were selected from the Clearwater Osteoarthritis Study (COS), a community-based longitudinal study of 3700+ participants age 40 and older, conducted by the Arthritis Research Institute of America in the Clearwater, Florida area from 1988–2009.
Data collected from COS participants every two years included demographic, personal attributes, health history, lifestyle, physical exam, and radiographic exam information. More detailed information on the COS is documented in other publications.17–20
The COS was conducted in accordance with ethical standards of the COS Institutional Review Board, (US Dept. of Health and Human Services IORG #0005812) and following the guidelines of the Helsinki Declaration. Informed consent was obtained from the COS study participants at each visit they completed.
For this study, we used selection criteria that would yield a sample of at least 100 COS participants for statistical evaluation. The COS participants in this sample were 78 (±1 year) of age and had no radiographic evidence of OA in either knee (KL < 2).
Definition of Radiographic Knee OA
All COS participants had weight-bearing anterior-posterior (AP) knee x-rays taken by a licensed x-ray technician using standard plain-film exposure techniques at each visit. A board-certified radiologist who had no knowledge of participant's symptoms or physical characteristics graded each radiograph for presence and severity of radiographic knee OA. 20 The x-rays were scored based on the Kellgren and Lawrence (KL) knee OA criteria as described by the Atlas of Standard Radiographs of Arthritis. 21 This ordinal system grades joints on a scale of 0–4: 0 = none or absent, 1 = questionable osteophytes and no joint space narrowing, 2 = definite osteophytes with possible joint space narrowing, 3 = definite joint space narrowing with moderate multiple osteophytes and some sclerosis, and 4 = severe joint space narrowing with cysts, osteophytes and sclerosis present. Each knee received a single KL score for the lateral and medial compartments of the tibio-femoral joint together. Absence of radiographic knee OA was determined by a KL score of < 2 in both knees. This is consistent with the primary definition of radiographic knee OA (KL ≥ 2) used in most research.22,23
Knee Alignment
Knee alignment for each study participant at age 78 years (±1 year) was determined using three different methods, including from radiographs, during the physical exam, and from the participant's medical history form. For each participant, the alignment for each knee, based on the angle between the tibia and femur, was designated as straight, varus, or valgus. For x-ray assessment, a board-certified radiologist reviewed the films to determine the alignment for each knee based on visualizing the angle between the tibia and femur, as well as visible rotation. Long-leg radiographs were considered for the longitudinal COS. However, knee-segment only films were chosen because the additional pelvic radiation exposure of bilateral full limb x-rays was deemed unacceptable by the Institutional Review Board and the additional expense of the specialized equipment and supplies were prohibitive. This was not considered an issue for this specific investigation, as both Kraus et al.
24
and Hinman
25
found significant positive correlations between long-leg and knee-segment-only radiographs when assessing knee alignment (r = 0.65,
Knee Range of Motion
For each knee, ROM was measured in degrees using a goniometer during the visit nearest age 78 (±1 year) physical examination. Extension is the number of degrees away from straight (0 degrees). Flexion is the outer angle of the flexed leg from fully extended (0 degrees) to fully flexed.
BMI
BMI was based on the height and weight measurements obtained during the visit closest to age 78 (±1 year) using the following standard formula: BMI = weight (in pounds) × 703/height 2 (in inches). 26 BMI at age 25 was based on the self-reported weight and height responses provided on the medical history form during the initial visit “What did you weigh at 25?” and “What was your height in stocking feet at age 25?”
Statistical Analysis
We described participant characteristics, physical examination and x-ray examination results, and self-report responses to the COS questionnaire. The level of significance for the analysis of variance and the post-hoc tests was set at
Differences between gender and between side of body (left or right) in knee alignment and knee range of motion were evaluated using appropriate t-tests and the 95% confidence intervals for the mean difference. Chi-square goodness of fit tests were used to examine equal proportions on binomial variables indicating similar alignment in both knees and five binomial tests of proportions indicating a specific alignment combination for both knees compared to all other remaining combinations (eg, straight and valgus compared with all other alignments).
Data analyses for this study was conducted using SAS software, Version 9.3 (SAS Institute, Cary, NC, USA).
US population means for different age, race, and gender categories for BMI were provided for contextual reference from the National Health and Nutrition Examination Surveys (NHANES). 27 For the 78-year-old age group, the NHANES IV, 1999–2002 data from the 75+-year-old age group were used. For the 25-year-old age group, the 1960–1962 National Health Examination Survey (NHES) I, data from the 20–29-year-old group were used. The selected race categories for comparison to this study's all Caucasian participants were all races and non-Hispanic white.
Results
Study Population
General demographic characteristics of this group of COS participants without radiographic knee OA are presented in Table 1. These data can be used to compare other study groups with and without radiographic knee OA. All COS participants were Caucasian (100%) and most were female (72.0%) which is higher than the United States (US) Census 2000 population estimate of 59% women for the age group 75–79-years-old. 28
Demographics of COS a participants absent knee OA b at age 78 years.
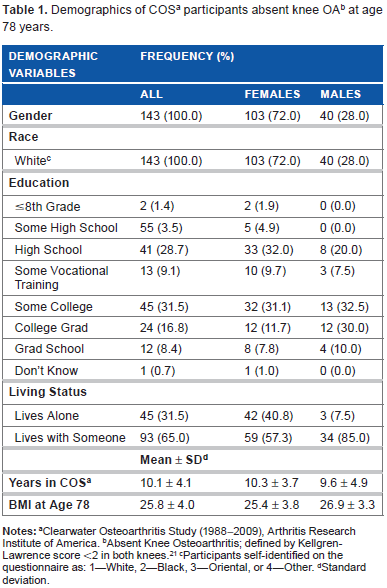
Clearwater Osteoarthritis Study (1988–2009), Arthritis Research Institute of America.
Absent Knee Osteoarthritis; defined by Kellgren-Lawrence score <2 in both knees. 21
Participants self-identified on the questionnaire as: 1–-White, 2–-Black, 3–-Oriental, or 4–-Other.
Standard deviation.
The education levels in this group of COS participants without radiographic knee OA were similar to the US Census 2000 population estimates for individuals over 65-years-old: 28.6% graduated from high school, 15.5% graduated from college, and 8.9% had at least some graduate level education. 28
Overall, 65.0% of this group of COS participants lived with at least one other person, which was higher than the US Census 2000 population estimate of 53% for individuals over 65-years-old. The proportion of male COS participants who lived with another person (85%) was higher than the 75% reported in the 2000 US Census report. 29
The BMI values for this group of COS participants without radiographic knee OA are at the cusp between the WHO categories of “normal” (18.5 to < 25) and “overweight” (25 to < 30). 26 The BMI values for this group of men and women are similar to the National Health and Nutritional Examination Survey (NHANES) 1999–2002 values by gender for ages 75 and older (all races); for women 26.8 (SE = 0.4) and for men 26.8 (SE = 0.2). 27
Knee Alignment
Based on x-ray exams, 81.8% of the participants had both knees classified with the same alignment: both straight (11.2%), both valgus (21.7%), and both varus (49.0%). However, the distribution of both knees valgus and both knees varus in women and men was markedly different. For both knees valgus, 30.1% of women had valgus knees, whereas no men (0%) had valgus knees. The percentage of men with both knees varus (77.5%) is more than double the percentage of women (37.9%) with both knees varus. The remaining participants (18.2%) had knees classified with different right and left knee alignments. More women (19.5%) had different knee alignments than men (15.0%). Overall, based on x-ray exams, most participants (88.6%) had at least one knee valgus or one knee varus (Table 2).
Distribution of knee alignment among COS a participants absent knee OA b at age 78 years based on X-rays, physical exams, and childhood recollections.

Clearwater Osteoarthritis Study (1988–2009), Arthritis Research Institute of America.
Absent Knee Osteoarthritis; defined by Kellgren-Lawrence score <2 in both knees. 21
Knee alignment/X-ray Exam: Board-certified radiologist used weight-bearing, anterior to posterior, bilateral knee x-rays to classify each knee as straight, valgus, or varus.
Knee alignment/Physical Exam: Examiner visually assessed and classified each knee as straight, valgus, or varus.
Knee alignment/Childhood Recollection: Participant recalled whether in childhood legs were straight, knock kneed (valgus), bowlegged (varus), or don't know.
Knees Same alignment: both knees straight, both knees valgus, or both knees varus.
Knees Different alignment: left and right knees have different alignments.
Based on physical exams, 93.7% of the participants had both knees classified with the same alignment: both straight (51.7%), both valgus (17.5%), and both varus (24.5%). Only 6.3% of the participants had knees classified with different right and left knee alignments. Similar to the findings based on x-ray exams, more women had knees classified with different knee alignments (6.8%) than men (5.0%). However, based on physical exams, fewer than half of the participants (48.3%) had at least one knee valgus or one knee varus.
Based on childhood recollections, 97.1% of the participants self-classified with same knee alignment: both straight, knock kneed (both valgus), or bowlegged (both varus). In contrast to the findings based on x-ray and physical exams, most (85.0%) participants self-classified with both knees straight. In women, 6.9% recalled valgus and 6.9% recalled varus alignment. None of the men recalled valgus alignment, which is consistent with findings from the x-ray exams. Only 7.7% of the men recalled varus alignment in childhood, which is markedly lower than findings using the x-ray exam (77.5%) or the physical exam (35.0%) knee alignment assessment method.
Comparison of Knee Alignment Determination Methods Based on Participants with Same Knee Alignment
Most COS participants without radiographic knee OA had both knees with the same alignment, regardless of knee alignment determination method. Therefore, we performed all subsequent analyses on participants with same knee alignments for both knees.
Comparison of X-Ray Exam with Physical Exam Methods
We compared the knee alignment for COS participants absent radiographic knee OA among the subgroups with same knee alignments for each assessment method (Fig. 1) and by individual participant (data not shown). Knee alignment classification is not consistent between these two subjective methods used in this study, which included x-ray exam and physical exam.
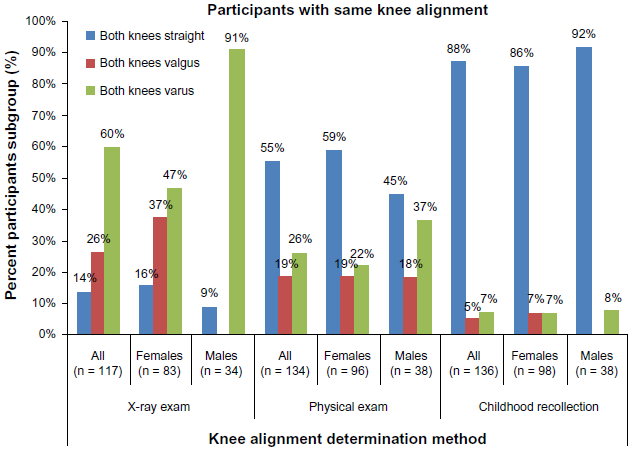
Percent distribution of individuals among COS subgroups with same knee alignment absent radiographic knee OA at age 78 years grouped by method of knee alignment determination: X-ray exam, physical exam, and childhood recollection.
More women (59%) and men (45%) were classified with both knees straight based on physical exams than based on x-ray exams (16% and 9%, respectively). Fewer women (19%) were classified with both knees valgus based on physical exams than based on x-ray exams (37%). More men (18%) were classified with both knees valgus based on physical exams than based on x-ray exams (0%). Fewer women (22%) and men (37%) were classified with both knees varus based on physical exams than based on x-ray exams (47% and 91%, respectively).
Similarly, when comparing the two knee alignment classification methods for individual participants, the alignment classification was not consistent. For example, of the women classified with both knees straight based on physical exams, most were classified either with both knees valgus (34.1%) or with both knees varus (46.8%) based on x-ray exams; only 19.1% were classified with both knees straight based on physical and x-ray exams. Of the men classified with both knees straight based on physical exams, all (100%) were classified with both knees varus based on x-ray exams; none (0%) were classified with both knees straight or both knees valgus.
The standard method for determining and reporting knee alignment in the OA literature is based on x-ray exams. Therefore, we use knee alignments determined from knee x-ray exams in the remaining analyses.
Comparison of Childhood Recollection with X-Ray Exam Methods
We compared knee alignment based on recollection and x-rays. Of the women who recalled having straight knees during childhood, 42.6% had both knees classified as valgus and 44.3% had both knees classified as varus based on x-ray exams at age 78; the remaining 13.1% had both knees classified as straight. Of the men who recalled having both knees straight during childhood, 89.7% had both knees classified as varus at age 78 based on x-ray exams. No men had both knees classified as valgus at age 78 based on x-ray exams.
Knee Alignment and BMI
Comparison of Knee Alignments with Bmi at Age 78
Based on analysis of variance, there was a statistically significant difference in BMI at age 78 among the three alignment categories determined by x-ray for women (

Distribution of BMI and change in BMI among COS subgroups with same knee alignment based on x-ray assessment for female and male COS participants absent radiographic knee OA at age 78 years. (A) BMI for females in the valgus group was significantly greater than the varus group (
Comparison of Knee Alignments with BMI Change over Time
BMI change over time represents an approximate 55-year interval between young adult (age 25) and 78 year-old elderly adults. There was generally a 5-unit BMI increase from young adult to elderly adult in women and men for all knee alignment categories. For women, there was a statistically significant difference in BMI change among the three alignment categories (
Knee Range of Motion
Overall, the COS male and female participants without radiographic knee OA at age 78 had good knee range of motion. There was no statistically significant difference between men and women for knee extension or knee flexion (Table 3).
Knee range of motion among COS a participants absent knee OA b at age 78 years.

Clearwater Osteoarthritis Study (1988–2009), Arthritis Research Institute of America.
Absent Knee Osteoarthritis; defined by Kellgren-Lawrence score <2 in both knees. 21
Standard deviation.
Knee range of motion determined during physical exam. Flexion is the outer angle of the flexed leg from fully extended (0 degrees) to fully flexed (approaches 140 degrees). Extension is number of degrees away from full extension (0 degrees).
In men, left knee flexion was statistically significantly greater than right knee flexion (
Knee Range of Motion and BMI at Age 78
Using Pearson correlation analyses, there were no statistically significant correlations between knee ROM parameters and BMI for women or for men.
Knee Range of Motion and Knee Alignment
Male and female participants with both knees straight showed better knee extension (closer to 0°) and better knee flexion (approaching 140°) than participants with both knees varus or both knees valgus (Fig. 3 and Table 4).

Distribution of knee range of motion among COS subgroups with same knee alignment based on x-ray assessment for female and male COS participants absent radiographic knee OA at age 78 years. Only four graphs are presented because right knee and left knee data were similar. (A) Right knee extension in females was significantly closer to full extension in the straight group when compared to either the valgus (
Analysis of knee alignment and knee range of motion among COS a participants absent knee OA b at age 78 years.

Clearwater Osteoarthritis Study (1988–2009), Arthritis Research Institute of America.
Absent knee osteoarthritis; defined by Kellgren-Lawrence score <2 in both knees. 21
Standard deviation.
Knee alignment determined by radiologist from standing anterior to posterior bilateral knee x-rays: 3 categories assessed – both knees straight, both valgus, or both varus.
Knee range of motion measured in degrees. Extension is number of degrees away from straight (0 degrees). Flexion is the outer angle of the flexed leg from fully extended (0 degrees) to fully flexed (approaches 140 degrees).
t-test (Tukey-Kramer adjustment for multiple comparisons).
Women with both knees valgus showed statistically significantly reduced function in right and left knee extension and in right and left knee flexion than women with both knees straight; no men had both knees valgus. In general, both women and men with both knees varus showed statistically significantly reduced right and left knee extension and right and left knee flexion than individuals with both knees straight (Fig. 3 and Table 4).
Discussion
In this study, we examined knee alignment and knee range of motion characteristics by gender in a population of 78-year-old men and women without radiographic knee OA. We also compared radiographic and physical exam definitions of knee alignment and radiographic knee alignment at age 78 to recalled childhood knee alignment. Associations among radiographic alignment groups and BMI classes, ROM and BMI classes, and knee alignment and knee range of motion were considered. Although these men and women had two or more OA risk factors (female gender, older age, increased BMI, and knee malalignment), they did not have radiographic knee OA. This study documents the complex relationships among knee OA risk factors in elderly adults without radiographic knee OA.
Study Population
In The Cos Study Group, Nearly 75% Of The Participants Were Women. This Gender Distribution May Have Resulted From A Sampling Effect, An Age Effect (In The General Population There Are More Older Women Than Older Men), A Gender Difference In Non-Occurrence Of Radiographic Knee Oa At Age 78, Or A Combination Of All Three. 28 General Population Prevalence Rates Calculated Specifically For Absence Of Radiographic Knee Oa By Gender Were Not Available In The Scientific Literature. 5
Knee Alignment
Varus knee malalignment is a risk factor for knee OA development and progression.6,10 However, most participants (60%) in our group of 78-year old men and women had varus knee alignment (determined from x-rays) and did not have radiographic knee OA. Normal musculoskeletal developmental changes can occur, resulting in varus and valgus alignments in healthy individuals. Nicolella et al.
30
described a study by Bellemans of healthy 20–27 year olds with ‘constitutional’ varus alignment in men (32%) and women (17%). Laxafoss and colleagues
31
reported statistically significant correlations between increasing age and increasing angular change toward valgus alignment men and women without knee OA (
Gender-Related Differences
In this study, we identified gender differences in the frequency distribution of knee alignment categories in 78-year-old participants. The frequency of women with both knees valgus based on x-ray assessment was 22%, which is similar to the 20% reported by Laxafoss for the Copenhagen Osteoarthritis Study 70–79 year age group without knee OA. 31 However, no men (0%) had both knees valgus, unlike the 20% Laxafoss reported for men. In our study, the frequency of participants with both knees varus was similar between genders: 27% for women and 22% for men (Table 2). Our proportions are markedly greater than the findings in Laxafoss study: 8% for men and 8% for women in the 70–79 year age group. In our study, the frequency of straight knees was markedly lower (women 16% and men 9%) than the 72% reported for women and men in the Laxafoss study (Sample size for the 70–79 year age group not reported in the Laxafoss study). Study participants in both the COS and the Laxafoss paper appeared to share the commonalities of being primarily urban and Caucasian, selected for the respective studies independent of OA status. Similar knee radiographic views and assessments were conducted. The variations in alignment characteristics of the older participants without knee OA may be related to lifestyle and/or genetic differences based on the different countries and world regions of origin.
Childhood Alignment-Related Differences
In our study, based on childhood recall, 88% of participants had straight knees, 5% had valgus knees, and 7% had varus knees. Schouten and colleagues 32 reported an increased risk of incident knee OA in individuals who recalled valgus (knock knees) or varus (bow legs) alignment during childhood. McWilliams 33 reported older participants (age range 55–75 years) recalled straight alignments in 95% of participants without knee OA and in 85% of participants with knee OA, which is similar to the 88% reported by our 78-year old no radiographic knee OA study participants.
Knee alignments commonly change during an individual's lifetime from childhood to adulthood. Based on clinical examinations, Cahuzac and colleagues found that male and female children between the ages of 10–13 years have similar valgus knee alignments; however, by age 16 years, male children have more varus alignment than female children (
Comparison of Physical Exam Andx-Ray Exam Methods
Although full limb radiographs are considered the most accurate method for classifying knee alignment, antero-posterior (AP) knee x-rays and physical exams are the most frequently used methods in clinical settings 25 and were the two methods used in our study. Only 1/3 of the participants were found to have the same knee alignment based on the physical exams and the AP x-ray exam methods. Most participants (66%) were classified into different knee alignment categories (straight, varus, valgus) when the results from physical exams were compared to AP knee x-ray exams.
Kraus et al.
24
compared assessment of knee alignments using a goniometer in a physical exam with both full-limb and the knee-segment-only x-rays (to simulate AP knee films) from 57 participants with symptomatic knee OA. They found a statistically significant positive correlation (r = 0.70,
Knee Alignment and BMI
Obesity and knee malalignment, particularly varus alignment, are recognized as important risk factors for the development and progression of knee OA.6,13,36 In our study, 78-year old women and men were borderline normal-obese (mean BMI = 25.8). Women with valgus alignment had significantly greater BMIs (
Knee ROM
Reduced knee function is often present in individuals with knee OA. 37 However, the relationship between knee function and OA development is unclear. 30 In our study of older participants without knee OA, there were no statistically significant differences between knee flexion and extension based on gender or BMI. However, there were statistically significant differences based on knee alignment. Women with valgus or varus knee alignments showed a statistically significant decreased range of motion in knee extension and flexion than women with straight knees. Males with varus alignment had statistically significant decreased range of motion in knee extension and flexion. These functional reductions may be related to the biomechanical aspects of knee malalignment or vice versa; the reduced range of motion may have contributed to malalignment. Information about lifestage knee range of motion in conjunction with knee alignment would be helpful.
Study Limitations
This study is limited by its descriptive nature. It does not include an appropriate comparison group of 78-year-old men and women with radiographic knee OA for calculating relative risks. Knee alignment classifications were not based on full weight-bearing long limb radiographs. There was no measurement of knee alignment angles, so it is not possible to assess the severity of malalignment or easily compare our findings with other malalignment studies. Results may not be generalizable due to participant selection methods with resulting racial uniformity and gender disparity.
Conclusion
Although knee malalignment is a risk factor for knee OA, most 78-year-old women and men without radiographic knee osteoarthritis showed either valgus or varus alignments; only a small proportion had straight knees. Women with both knees valgus had significantly greater BMI (
Author Contributions
Conceived and designed the experiments: LF, ES. Analysed the data: ES, NO Wrote the first draft of the manuscript: DL. Contributed to the writing of the manuscript: DL, LF, NC, ES. Agree with manuscript results and conclusions: LF, DL, ES, NC. Jointly developed the structure and arguments for the paper: DL, LF. Made critical revisions and approved final version: LF, DL, ES, NC. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.
Footnotes
Acknowledgements
Thank you to the ARIA volunteers and staff who have provided the support necessary to collect, record, and analyze the Clearwater Osteoarthritis Study data.