
Abstract
Background
Increased speed and resolution of ultrasound have made it a first-line modality for the abdominal examination. During the last 5 years trans-abdominal ultrasonography has been used increasingly, for assessment of patients with small bowel (SB) diseases. Around 350 such examinations are performed annually in the diagnostic imaging department at Azhar University Hospital. Hence, the aim is to determine if the ultrafast three-dimensional ultrasound (U3D US) is potent for optimal examination of SB diseases.
Patients and Methods
Tap-water intake has been used to distend the SB. All patients have been examined in supine position. The U3D US data of 198 patients with SB diseases were assessed. The proximal and distal SB image quality along with the evaluation of bowel distention, motility and lesions were reported.
Results
Image quality was good in all examinations. Adequate demonstration of the proximal and distal SB was obtained in all of U3D US examinations. The inclusive diagnostic accuracy of U3D US was precise in 92.3%. Proximal SB was, however, less frequently involved, particularly in patients below the age of 30 years (
Conclusion
The diagnostic accuracy of U3D US enterography is valuable for detecting SB lesions. This modality is widely available, inexpensive and easy technique, can be used as an initial investigation in the evaluation of patients with SB disorders.
Introduction
The advent of endoscopy has increased the diagnostic possibilities of small bowel (SB) disorders. Wireless capsule video-endoscopy is the most recent method, which may allow for excellent visualization of the SB mucosa and any luminal abnormalities, but it does not clearly localize the area of the SB where lesions are identified or demonstrate beyond the mucosal surface; therefore its specificity is lower than other methods. 1 3 In addition, there is a possibility of capsule retention where SB strictures are present. 4
Due to the variable sensitivity of barium follow-through (23%-80%) for the detection of SB lesions, 5 much research has been directed toward the potential of cross-sectional imaging modalities for the diagnosis and evaluation of SB diseases, as with these techniques the bowel lumen, the bowel wall and the extra-intestinal abdomen including the visceral fat, the lymph nodes and the vascular structures feeding and draining the bowel can be visualized. 5 7
Minordi et al reported that Multi Detector Computed Tomography (MDCT) enteroclysis has been shown to be superior to small-bowel barium examinations, conventional CT, and complementary to capsule endoscopy in the elective investigation of small-bowel disease. 8 However, the growing awareness of the risks of ionizing radiation exposure has prompted the exploration by Magnetic Resonance Enteroclysis (MRE) useful in assessing the quality and quantity of bowel. Advantages of MRE imaging include a lack of ionizing radiation and the ability to provide dynamic information regarding bowel distention and motility. 9 The main value of enteral MDCT and MRI is that they permit detection of jejuna lesions that have escaped detection with conventional two-dimensional ultrasound (2D US) imaging. 8 10 The reason is frequently because the surface visualization of ultrasound image contains many speckles, so that the interesting image parts and minute details of ultrasound anatomy are not definite. 10 12
The recent advances of dynamic interactive speckle subtraction accompanying the introduction of three-dimensional ultrasound (3D US) have provided good quality display for proper tissue characterization and subsequently visualization of subtle lesions. 13 16
During the last 5 years ultrafast three-dimensional ultrasonography (U3D US) has been increasingly used for assessment of patients with bowel disease. Almost about 350 such examinations are performed annually in the diagnostic imaging department at Azhar University Hospital which is also the site for the management of bowel diseases.
The aim of this prospective study was thus to assess the quality of U3D US imaging in SB diseases and to confirm whether imaging of patients with this modality can provide a quality adjunct diagnosis.
To our knowledge, no previous studies addressing the ultrafast 3-dimensional ultrasound (U3D US) on the small bowel or explaining the small bowel U3D US's display techniques have been published before.
Patients and Methods
The study protocol, including review 17 of the ultrasound normal figures for the SB, was approved by the local research ethics committee, who deemed that patient consent was not required for this study as both conventional and 3-dimensional ultrasound are considered to be standard examination methods.
We prospectively evaluated 189 patients; 102 male patients aged 17-72 years (mean age, 44.5 years) and 87 female patients aged 20-74 years (mean age, 40.3 years). All subjects were patients of Azhar University Hospital, Cairo, Egypt, which is also the site for the management of bowel diseases. All patients had undergone the necessary laboratory investigations. The clinical indication for U3D US test was mainly to assess reasons for recurrent episodes of abdominal pain with illness (
U3D US preparation
All patients drank tap-water for 15 minutes just prior to their U3D US test; 1200-1500 mL of pure tap-water was usually required for each to distend the SB, which varied depending on the patient's tolerance. There was no need for medications to reduce SB peristalsis or prolong SB distension. Patients were also asked to report any discomfort that they experienced after the procedure such as vomiting, diarrhea, or abdominal pain.
U3D US techniques
Patients were imaged in the supine position using a 3-dimensional ultrasound system (Accuvix V20, Medison, South Korea) with a volume probe (V 4-8 MHz, 75 frames/second). Routine conventional 2D US was primarily obtained to ensure adequate SB distention. Patients were asked to drink more water if the small bowel was not adequately distended. Visual division of the abdominal field into 4 quadrants centered on the umbilicus was well-thought-out. Real-time 4 scan-volumes were then acquired dynamically, one volume for each quadrant, without breath-holding to cover the entire abdomen. Additional volume or more were occasionally required when targeting any lesion was essential. The time of U3D US examination varied from 5 to 15 minutes (mean 10 minutes), depending upon how many additional volumes were required.
Image analysis
Each real time U3D US volume was reviewed twice: first to confirm proper volume acquisition, distensibility of the SB loops, motility and lesion detection. The U3D US volumes were then archived at a workstation (Sonoview_Pro 1.5.1).
After the patient left the examination room, the stored volumes were displayed and analyzed by a committee of well-trained specialists at least of 5 years’ experience, so as to evaluate U3D US modality, specifically for the presence of SB wall thickening, panoramic viewing of the mucosal aspect, and SB masses. Surface rendering was routinely viewed in sagittal, coronal, transverse and oblique contiguous images. Then, the multislice extended capability (XI MR) was performed to obtain very thin (0.5 mm) contiguous slices targeting the SB lesion at any overlap point.
The laboratory data for all patients (
Statistical analyses
Were performed with the commercially available software (SPSS 19.0 for Windows). All
Results
We used the previously reported ultrasound parameters for normal personnel presented in the report of Sporea et al 17 ; calibers = less than 3.0 and 2.0 cm for the jejunum and ileum, respectively and the normal wall thickness = less than 3.0 mm.
Data from 189 U3D US examinations of patients with SB disorders and their corresponding laboratory, enteroscopy and/or surgical data and their histologic findings were finally disclosed and scheduled. No significant difference was found in male to female sex (
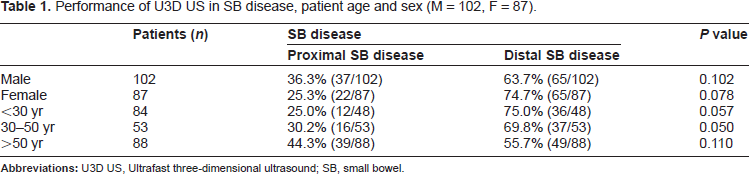
Tap-water intake was well tolerated in all the 189 patients in whom the examination was completed successfully, with good distention of the proximal and distal SB and good image quality (Fig. 1). No patient experienced side effects at the examination.
U3D UD showing the normal appearance of the small bowel; (
Performance of U3D US in SB disease, patient age and sex (M = 102, F = 87).
U3D US imaging findings and accuracy on 189 patients with small bowel disorders.

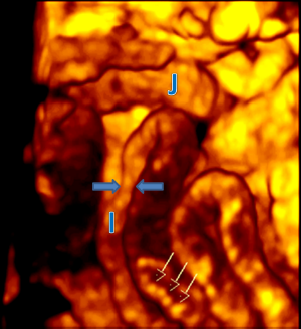
U3D US revealed thickening of the SB wall and broadening of the mucosal pattern as the main diagnostic criteria for enteritis. No significant variance could be noted differentiating infectious enteritis from irritable bowel, either in SB motility or wall changes. However, for typhoid enteritis, surface oval-shaped bright patches were noted and well thought-out to be characteristics (Fig. 2). In case of intestinal tuberculosis, stenotic segments were considered discerning, and mostly seen involving the ileum than the jejunum (Fig. 3).
U3D US coronal cut-section image of a 37-year-old female patient with known inflammatory bowel disease (typhoid). ( U3D US surface rendered image of a 17-year-old male patient with known intestinal tuberculosis. Image shows severe inflammation of the small bowel with dotty bright tiny (transversely aligned) spots involving the SB mucosal aspect (arrows), likely representing ulcers. Stenotic segments are noted (opposed arrows). The process is involving the ileum (I) more than the jejunum (J).
Crohn's disease in the present study was scheduled distinctly, as its pathogenesis is not yet known and has dissimilar diagnostic criteria. In CD, the U3D US enterography was able to demonstrate the thickened wall of the terminal ileum in all cases of this category, with central string-sign and marginal jagging representing infiltration of perivisceral fat (Fig. 4). However, one of them showed U3D US of early signs of abscess formation on coronal multislice sequence.
A 34-year female patient with intermittent abdominal pain and cramps. (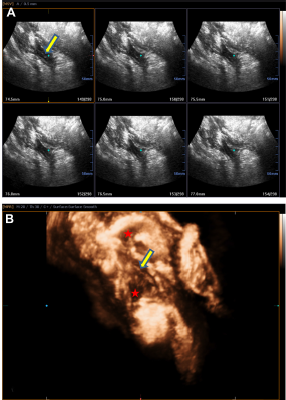
From a total of 4 SB mass lesions, all of them were confirmed at surgery. U3D US enterography helped us to identify luminal and the extraluminal patterns in 3 out of them (Fig. 5). However, the missed case with SB mass lesion showed partial SB obstruction and the location could be suggested at the level of the proximal ileum, which proved adenoma at surgery. The diameters of the neoplasms in the three cases of SB adenocarcinoma ranged from 19 to 43 mm (mean diameter, 26.7 mm). The extraluminal disease in these patients was liver metastasis in two patients and enlarged mesenteric lymph nodes in one.
U3D US images of ileal adenocarcinoma in 70-year-old man with unexplained loss of weight, abdominal pain and cramps. (
In the 7 patients who underwent surgery, there was perfect concordance with the findings detected at U3D US; demonstrated high-grade partial SB obstruction in one patient with SB adenocarcinoma inducing jejuno-jejunal intussusception (Fig. 6) and low grade partial small-bowel obstruction in six patients; three were due to mass lesion and the remaining three instances were due to CD.
38-year-old male with complaints of vomiting, abdominal distension and pain. U3D US-enterography to evaluate the small bowel revealed: (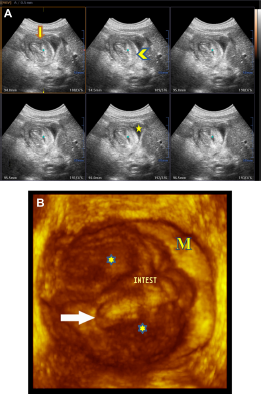
Discussion
Precise evaluation of SB lesions is difficult because of its curved course and overlapping folds. Currently, two major techniques are used: MDCT and MRI for the necessity to reveal the luminal, mural and extraluminal profile as well. 11
On the other hand, several reports mentioned that the role of sonography in the evaluation of SB neoplasms is similar to that of CT scan and comparable to MRI with oral contrast material administration. They mentioned that ultrasound is frequently performed early in the diagnostic work-up, which may lead to accurate recognition, localization and even staging of disease with the opportunity for directing appropriate further investigation, including sonography—guided aspiration biopsy. 18 21
In the present study, U3D US sequences yielded useful information in the evaluation of SB. The advantages of ultrafast volume acquisition and interactive speckle reduction are combined in this modality to overcome motion artifacts due to SB motility and enable the detection of intraluminal, mural, and extramural SB disorders along with motility information comparable to that gleaned at current cross-sectional imaging modalities.
Optimal distention of the SB has also been shown to facilitate for correct SB evaluation because collapsed SB loops can hide or mimic lesions or confusing thickened bowel wall in collapsed segments. This proved significant in accurate delineation of mural changes in patients with enteritis and CD, and also particularly proved important in the detection of the luminal, mural and extraenteric patterns of SB neoplasms in the early stage.
Results of the present study on U3D US compared to the previous reports on conventional 2D US,15,22–24 has been shown to be more sensitive in detecting mural changes of the SB, and more potent in the detection of mucosal surface abnormalities due to the better soft-tissue characterization. Besides, our results are almost parallel to that performed on MDCT 25 in the evaluation of SB neoplasms.
Moreover, the U3D US test can be performed several times, as it is a cost-effective, office-based technique, with no ionizing radiation exposure.
Our study had a number of limitations. First, most of our patients relieved on medical treatment after the U3D US assessments; and thus, for ethical reasons, it was difficult to do further invasive examinations in such patients in whom symptoms resolved with proper treatment. On the other hand, the remaining patients in our study with small bowel CD or neoplasms were presented with partial or complete intestinal obstruction, have been subjected to surgical interventions just after the U3D US test. Second, this was a single-center trial and its design is not reliable on the inter-observers’ variability and the disease prevalence or type in other populations. Nevertheless, our center covers a big population, hence, this attempt deemed feasible and more research is needed to establish the diagnostic effectiveness of this modality.
Conclusion
U3D US is widely available, inexpensive, and easy technique, can be used as an initial virtual enterography in the evaluation of patients with SB disorders.
Footnotes
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.