
Abstract
Background
Colonoscopy has a great impact on diagnosis and management of the diseases of the colon. In general it's a safe and accurate procedure. No evaluation has been done of any endoscopic practices in a country where the practice of medicine is totally private.
Objectives
Prospective audit of technical success and complication rates of both therapeutic and diagnostic colonoscopy.
Setting
One endoscopy unit of a Lebanese university hospital.
Patients and design
407 consecutive colonoscopies were evaluated over a 6-month period. Data were recorded for age and sex of the patients, indication of the colonoscopy, presence of comorbidities, patients risk stratification, administrated dose of anesthetic drugs. Data concerning the procedure itself were also monitored.
Intervention
Completion rate as well as complications reported during or post colonoscopy. All patients were called back by phone 48 hours and 1 month later to identify any related post-procedural complication.
Results
407 patients underwent colonoscopy. All patients were sedated with midazolam, propofol and fentanyl. The overall caecal intubation rate was 99.99%. 70 snare polypectomies and 29 cold forceps excision were performed as well as 5 coagulations with Argon Plasma Coagulation. The most important post-procedural complication was chemical colitis in 2 cases.
Limitations
Patients and endoscopists satisfaction was not evaluated. It's an audit of a single tertiary French affiliated hospital. It does not necessarily reflect what's really happening on a national level.
Conclusion
This audit enabled us to change some of our practices; i.e. rinsing method of endoscopes. It stimulated the team to keep a high performance level without neglecting the risk of potential complications.
Introduction
Progress in endoscopic technology has advanced the practice of medicine as it relates to the gastrointestinal tract. Scientists and clinicians have acquired unprecedented access to the gastrointestinal lumen and colonoscopy became the second most frequently performed procedure in U.S. ambulatory care. Direct examination of the mucosal surface provides great information and endoscopic treatment have now supplanted many open surgical procedures. Ongoing technical improvements and innovations continue to extend potential endoscopic therapies. In order to evaluate a procedure, we need to verify the quality of the service by tracking the outcomes, according to quality indicators: conditions of the procedure, diagnostic and therapeutic success, and patient evolution and satisfaction.1,2 Properly performed, colonoscopy is generally safe, accurate, and well tolerated by most patients. However, it is incumbent on endoscopists to evaluate their practices and seek to make improvements wherever possible. The aim of our study was to conduct a prospective audit concerning the diagnostic yield, technical success and complication rates of both therapeutic and diagnostic colonoscopy in the endoscopy unit of Hotel-Dieu de France University hospital in Lebanon over a 6-month period.
Patients and Methods
Patients
The cohort was composed of patients undergoing colonoscopy at Hotel-Dieu de France from February 1st to July 31st 2006. All colonoscopies were included, diagnostic and therapeutic, in hospital and on ambulatory basis. No patients were excluded.
For each patient, the physician had to fill a form concerning the patient's age and sex, the date and the indication of the colonoscopy, the presence of a past history of abdominal surgery, the presence of comorbidities including diabetes, renal failure, heart disease or pulmonary pathology, the ASA score, and the doses of anesthetic drugs received. The form also included data concerning the endo-scopic act itself. The duration of the colonoscopy and the limit attended in the colon, the adequacy of colon preparation, the finding and the eventual therapeutic act where monitored as well as the complications reported during or strictly post procedure.
All patients were contacted by phone 48 hours and 1 month after the colonoscopy to assess for adverse events.
Preparation
A low-fiber diet was started 3 days before the examination because we think it ameliorates the quality of preparation. 3 A polyethylene glycol electrolyte solution was used for bowel preparation. Patients had 4 liters ingested the night before the colonoscopy, and they stopped oral intake starting midnight.
The adequacy of bowel preparation was graded at the end of the procedure, as “good” (mucosa well seen throughout), “fair” (liquid contents, examination adequate), or “poor” (solid contents, examination compromised).
Sedation
All patients were seen by the anesthesiologists at least 24 hours before colonoscopy in accordance with the guidelines of the American society of anesthesiologists for ambulatory anesthesia and surgery 4 . All colonoscopies were done under general anesthesia. The sedation protocol followed by the anesthesiologists in our unit consisted of the association of midazolam 1 to 3 mg, propofol given by bolus of 20 mg every two minutes according to the depth of the sedation needed, and alfentanyl in doses of 250 to 700 μg. The doses varied with the patient's age, weight and the presence of comor-bidities. The sedation was maintained by ventilation with natrium protoxyde and oxygen.
After the procedure, the patients were surveyed until complete consciousness and oxygen saturation above 95%. The patients who underwent a therapeutic act during colonoscopy were admitted to the hospital for at least 24 hours for surveillance.
Endoscopes
The colonoscopies were done with a Pentax EC 3840 (Pentax, Tokyo, Japan), and two Olympus Exera CFQ 145L, CFQ 160ZL (Olympus, Tokyo, Japan) colonoscopes.
The endoscopes were manually cleaned. The 4 steps of cleaning included an external cleaning and brushing of all the endoscope channels with an antibacterial detergent then disinfection with glutaraldehyde (Sekucid®). All instruments were rinsed thereafter with drinking-quality water internally and externally to remove all traces of disinfectant and finally dried externally and by flushing each channel with air.
Statistical analysis
Study database management and all statistical analyses were performed with the SPSS (v.10). Descriptive analysis included the calculation of rates for count data and means and standard deviations for continuous data; statistical comparisons for count data were based on chi-square procedures; comparisons for continuous data were based on t tests. Significant results were considered when p was less than 0.05
Results
Patients’ clinical characteristics
Patients’ characteristics.

Indications of colonoscopy.

Technical modalities
Variation of mean doses of anesthetic drugs according to patients’ context.

Seuil p < 0.05.
Mean duration of colonoscopy according to patients’ context.

Seuil p < 0.05.
The overall caecal intubation rate reached 99.25% with an ileal intubation rate of 62.15% knowing that the ileal intubation was not systematically attempted.
Diagnostic and therapeutic yield
Endoscopic findings of the colonoscopies.
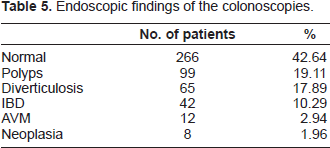
As to the therapy procedures, 70 snare polyp-ectomies were done, 17 of whichusing the muco-sectomy technique, 29 cold foceps excision and 5 Argon Plasma coagulations.
Morbidity
During the procedure, 25 (6.1%) complications were recorded: 18 vomiting which resolved spontaneously without the need for any treatment, two cases of oversedation and desaturation (a drop in the hemoglobin oxygen saturation of more than 4% or to less than 90%) which resolved after stopping the nitrogen protoxyde and increasing the oxygen output, one case of non severe premature ventricular arrhythmia and one atrial fibrillation that resolved spontaneously and three episodes of hypertension treated with I.V. nicardipine (Loxen®). All of these complications were thus treated on the spot without any need for hospitalization.
Post-procedural complications at 48 hours call.

Two patients presented to the emergency room, 24 hours after the colonoscopy, complaining of abdominal pain, fever and bloody diarrhea. Investigations showed no perforation, but the rectosigmoidoscopy found congestive, erosive mucosa, that was normal on the initial exam consistent with chemical colitis. They were treated on ambulatory basis with antibiotics and follow up was unremarkable after 48 hours. All the other events were mentioned when the patients where phoned back and did not necessitate any treatment.
2 (0.49%) patients reported slight bleeding 10 days after snare and forceps polypectomy which resolved spontaneously on the one month call.
Discussion
The aim of our study was to evaluate the quality of our endoscopy practice and to reevaluate the protocols we are following. We thus conducted this audit by recording all medical and technical details, the rate of complete colonoscopies, and all the short and long term complications, by controlling all the colonoscopies done over a six month period. We analyzed the results according to three quality indicators: the diagnostic yield, the rate of completion, and the rate of complications.
The team includes gastro-enterologists, anesthesiologists and nurses. Everyone has a specific and important role, and can influence the quality of care offered by the team. Four hundred and seven colonoscopies were recorded, without any
patient selection. All the patients who had done a colonoscopy during the study period were included. Were excluded only the colonoscopies done by the pediatric team.
Among our symptomatic patients (84%), 36.6% had significant pathological findings. This result matches with the diagnostic yield of colonoscopy stated in the literature (15%-45%). Among patients examined for screening (2.9%), 16.7% had pathological findings; whereas in the literature, they report a higher rate of screening colonoscopies (11%). The low rate of screening colonoscopies in our unit reflects the lack of a screening policy for colorectal cancer, not only in out unit but on a national basis.
All the colonoscopies were done under general anesthesia, with the presence of an anesthesiologist. We routinely provide sedation and analgesia in our unit. This is not the case in all the endoscopy units of our small country. Several studies had already demonstrated the influence of routine sedation and analgesia on patient satisfaction and on the effectiveness of colonoscopy. 1 This routine sedation and analgesia increases the cost of our endoscopic act by 110 american dollars (27% of the total cost). We intend to conduct in the near future a comparative study between routine sedation and “on demand” sedation hoping to reduce the cost of the colonoscopy while keeping the same level of performance, in a country with serious financial problems.
Effective colonoscopists should be able to intubate the cecum in ≥90% of all cases and in ≥95% of cases when the indication is screening in a healthy adult.2,5,6,7 We had a high completion rate in our series, 99.25% of the colonoscopies, compared to that reported in the literature which varies between 79% and 97%. This is probably due to the high rate of good preparation (61.17%), the general anesthesia, and the technical skills of the operators. Although it is not a good indicator of the sensitivity of the colonoscopy, it contributes besides other factors such as retrieval time and good preparation, to increase the sensitivity rate.
The complications reported after the colonoscopies were mostly minor ones, due to the general anesthesia (nausea, vomiting, dizziness).8,9,10,11 Abdominal pain, known to be due to the insufflation of carbon dioxide during theprocedure is a frequent complication after colonoscopy. Diarrhea in the first 48 hours after the procedure is a frequent complication and is due to the remaining preparation solution in the gut. 12
The rate of perforation stated in the literature is 0.03% to 0.8% for diagnostic colonoscopies and 0.073% to 3% for therapeutical colonoscopies.13,14,15,16 Bleeding occurs in 0.008% to 1% of diagnostic colonoscopies and 1.6% to 2.1% of therapeutical colonoscopies.17,18,19 No perforation and no significant bleeding were reported over our 407 colonoscopies.
The two chemical colitis we reported were due to glutaraldehyde, the solution we use to clean the endoscopes. This complication is stated in the literature, it is due to insufficient rinsing of the endoscope after glutaraldehyde. 20 This complication lead us to change our cleaning method, we are using an irrigating pump instead of manually rinsing the colonoscope. We also prolonged the rinsing time to six minutes after consulting the hygiene responsible in the hospital.
This audit, the first to be conducted in our country, allowed us to evaluate our endoscopic practices and enabled us to change some of them. The high rate of technical success and the safety of the procedure encouraged us to start to establish a screening policy for colorectal cancer at the level of the Lebanese society of gastroenterology. It also stimulated the team to evaluate other quality indicators such as retrieval time, appropriateness of indication, sensitivity of the endoscopic exam and others to define areas for continuous quality improvement supporting the recommendation from professional societies.