
Abstract
Background
The incidence of microscopic colitis (MC) is increasing, but its etiology remains unknown. Case reports and limited controlled data suggest that commonly prescribed drugs may be triggers. The aim of this study was to evaluate the prevalence of selected medication use [Proton pump inhibitors (PPIs), HMG-CoA reductase inhibitors (statins), and Selective serotonin reuptake inhibitors (SSRIs)] in patients with MC compared to ‘random controls’ and ‘diarrhea controls.'
Methods
All patients were selected from primary care practices of a university health system during 2002 to 2007. Patients with biopsy proven lymphocytic or collagenous colitis were identified as cases. Diarrhea controls consisted of a 10:1 random sample of patients with chronic diarrhea and normal colon biopsies. Ten random controls were matched to each case on sex and index date (date of biopsy proven diagnosis). Drugs prescribed within the year prior to the index date were collected from the electronic medical record system.
Results
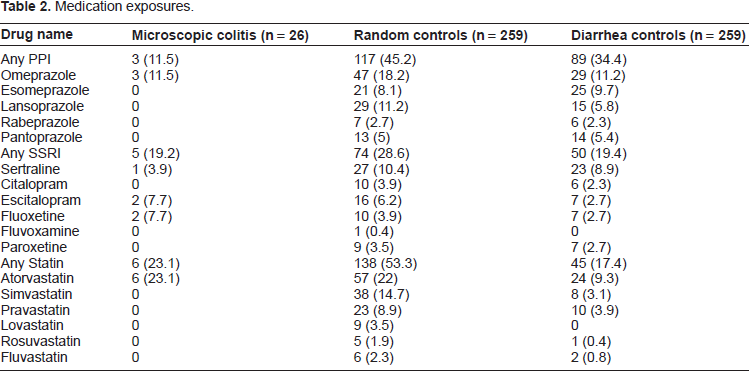
26 cases (median age 68.9 yrs), 259 random, and 259 diarrhea controls were identified. The adjusted ORs for PPI, SSRI, and statin prescription within 12 months of diagnosis of MC between cases and diarrhea controls were 0.28 (0.07-1.07), 0.87 (0.28-2.64), 1.12 (0.34-3.71) respectively. Use of PPI and statins was less common in MC patients than in random controls (P < 0.05 for both comparisons).
Conclusions
While prior data suggest that PPIs, statins, and SSRIs may be etiologically related to MC, our study found no increased association with these drugs.
Keywords
Background
Microscopic colitis describes a group of chronic inflammatory bowel disorders characterized predominantly by chronic diarrhea in patients with a grossly normal or near-normal colonoscopy. Most commonly, patients present with chronic nonbloody diarrhea accompanied by weight loss and/or abdominal pain. There are 2 specific subtypes of microscopic colitis, collagenous colitis and lymphocytic colitis, which are indistinguishable clinically but have classic histopathologic features. Both subtypes are pathologically characterized by a marked increase in intraepithelial lymphocytes with expansion of the lamina propria with acute and chronic inflammatory cells but preserved crypt architecture. 1 Collagenous colitis is further characterized by the presence of a thickened subepithelial collagen band. 1
The annual incidence of microscopic colitis is approximately 10/100,000 in North America with a prevalence of about 0.2%. 2 Previous epidemiological studies observed a female predominance (2:1) with a peak incidence at approximately age 60 years. 3 It appears to be more prevalent among the Caucasian race and has a possible association with other autoimmune diseases such as celiac disease.3,4 The clinical nature of microscopic colitis is generally considered benign, however, patients often have a spontaneously relapsing and remitting course similar to other inflammatory colitides.1,3
While the disorder has been well-recognized for the last 30 years, the underlying etiology remains unknown. Commonly held theories propose that environmental factors such as an infection, toxin, or drugs induce an abnormal immune activation to luminal antigens which then leads to inflammation of the colonic mucosa. 1 Since diarrhea is a common side-effect of many medications and patients in later decades of life are more likely to initiate new medications and in general, take more medications, drug consumption has been postulated as a contributing factor in the development of microscopic colitis. 5 Nonsteroidal anti-inflammatory drugs (NSAIDs), proton pump inhibitors (PPIs), HMG-CoA reductase inhibitors (statins), and selective serotonin reuptake inhibitors (SSRIs) have all been proposed to be linked to microscopic colitis on the basis of uncontrolled case reports or case series. 6 8 However, the majority of data regarding these associations are descriptive and uncontrolled. In contrast, a recent controlled study reported that while SSRIs, NSAIDs, beta-blockers, bisphosphonates, and statins were prescribed more commonly among patients with lymphocytic or collagenous colitis than among a control sample of patients undergoing cataract surgery, when medication use in lymphocytic and collagenous colitis patients were compared to patients with chronic diarrhea, only the use of sertraline was significantly more common among patients with microscopic colitis. 9 These findings support the notion that perhaps drug-induced chronic diarrhea or greater exposure to colonoscopy with biopsy among patients receiving these medications may lead to an increase in the diagnosis of microscopic colitis rather than these medications being a causative or triggering factor in its development. Our main objective was to further test the hypothesis that commonly used drugs such as PPIs, SSRIs, and statins were associated with the diagnosis of microscopic colitis.
Methods
We performed a case-control study within the University of Pennsylvania Health System. All subjects were required to have received care from practices using the Health System's EPIC electronic medical record. We identified cases from patients with a new pathologic diagnosis of lymphocytic or collagenous colitis from colonic specimens submitted to the Pathology Department of the Hospital of the University of Pennsylvania between the years 2002-2007. All specimens were obtained from colonoscopies of patients performed for the indication of diarrhea and over 80% of the specimens were reviewed by one of 3 expert gastrointestinal pathologists at our institution. From this list of patients, we included only those patients who had at least 1 outpatient primary care visit listed in the EPIC electronic medical record system prior to the date of the colonoscopy in order to have a uniform method for obtaining medication data.
We selected two control groups. The diarrhea control group was composed of patients who underwent colonoscopy for an indication of chronic diarrhea and in whom random biopsies were obtained. The indications for colonoscopy were obtained from the endoscopy report. From this list, we again included only those patients who had at least 1 outpatient primary care visit in EPIC prior to the date of the colonoscopy. Using a computerized randomization scheme, we selected 10:1 unmatched ratio of control subjects with biopsy-normal diarrhea for each case subject. The second control group, the random control group, was composed of patients cared for by primary care physicians in the same health system. Ten controls were randomly selected to match to each case by year of birth and having a primary care office visit listed in EPIC within 1 month of the pathologic diagnosis date of microscopic colitis.
We excluded both case and control subjects who were less than 18 years of age, with a concomitant diagnosis of Crohn's disease, ulcerative colitis, or indeterminate colitis.
Exposure data were extracted directly from the EPIC database for incorporation into analytic datasets for this study. We looked at 3 exposure time periods for medication use: within 12 months of index date, 6 months, and 3 months. The EPIC electronic medical record system is utilized by the majority of primary care and specialty practices within the University of Pennsylvania health system and contains information regarding patient-related clinic notes, phone calls, orders, laboratory and radiology data, diagnoses, and records of the majority of prescriptions written for each patient. Medication prescriptions and refills are written through EPIC by each prescriber. During each visit, the prescriber is prompted to review the history, medication and allergy list and the practitioner/prescriber can update the list manually to provide a historically accurate record of medication exposure (defined as ≥ medication listed in EPIC during the time of interest) and diagnoses at time of each visit. Diagnoses, such as diabetes mellitus and hypertension, are identified through the International Classification of Diseases (ICD-9) codes. As of 2007, EPIC contained information on approximately 80,000 patients seen within the health system primary care practices.
BMI was calculated using the weights and heights of the cases and controls at the primary care office visit just prior to the index date or matched date of analysis. BMI was then listed into categories based on the standard cutoffs for normal (BMI < 25), overweight (BMI 25-29), and obese (BMI ≥ 30). If only weight was reported, we imputed BMI using previously reported methods. 10 We collected demographic characteristics, pertinent diagnoses, and medications listed in the year prior to the index date or matched date for all patients. Pathology and endoscopy reports were also collected from EPIC and the university pathology database for manual review.
Statistical Analysis
The primary exposure variable was use of the medications of interest within 12 months of the index date (the date that the case subject was diagnosed with microscopic colitis). Medication exposure was considered to end either on the last day of supply or the end date which was documented in EPIC of the prescribed medication. Demographic characteristics were compared using t-tests and Chi-squared tests as appropriate. In our primary analysis, exposure to medication was defined as medication listed in EPIC within the year prior to the index date. Conditional logistic regression analysis was performed to assess whether the odds of exposure to the medications of interest was greater in the cases than in the matched random controls. Unconditional logistic regression analysis was performed to compare exposures among cases to that among the diarrhea (normal biopsy) controls. ORs and 95% confidence intervals were reported to demonstrate the strength of our associations and the surety with which they are estimated. For both comparisons, a step-down logistic regression was used and potential confounders were included in the final model if their inclusion changed the unadjusted odds ratio by at least 10%. To assess for potential bias related to our definition of exposure, sensitivity analyses were also performed using the following alternative definitions for medication exposure that required evidence of exposure within 6 months and within 3 months prior to the index date (date of colonoscopy with biopsy).
The finding of MC is rare and given finding only 25 cases which met our criteria over 7 years, it was felt that additional surveillance for this disease to potentially increase our sample size would only have provided a few more incident cases and not enough to significantly increase our power. Thus, given a case sample size of 25 cases, a case:control ratio of 1:10 for each control group and exposure to medication in the control group of 0.30, we estimated that we would have 60% power to detect an OR of 2.5 and an 80% power to detect an odds ratio (OR) of 3.2 or greater.
Results
Demographic characteristics.

P-value between cases and diarrhea controls.
P-value between cases and random controls.
P-value between diarrhea and random controls.
The diarrhea controls were younger (P < 0.01) than the case group but there was no significant difference in the median weights, BMIs or the prevalence of co-morbidities.
Drug use
Medication exposures.
Cases versus random controls
Association of medication exposure in microscopic colitis vs. random controls.

Cases versus diarrhea controls
Association of medication exposure in microscopic colitis vs. diarrhea controls.

Discussion
Commonly prescribed medications have been proposed as contributing to the etiology of microscopic colitis. In this study, we did not observe an increased risk of microscopic colitis in association with the use of PPIs, SSRIs or statins. In fact, use of these medications tended to be less common empirically among patients with microscopic colitis than among those in either of the control groups. These data argue against an etiologic role for these medications in the pathogenesis of microscopic colitis.
The incidence of microscopic colitis has increased dramatically over the last 30 years and is most common in middle-aged female patients. Increased detection has been implicated as a significant contributor to this rising number since diagnosis of microscopic colitis is inherently tied to the performance of colonoscopies and suspicion index for obtaining random biopsies. Similarities in the secular trends of the diagnosis of microscopic colitis and the use of medications to treat acid suppression, hypercholesterolemia, and depression/anxiety disorders contributes to the hypothesis that these medications may play a role in the etiology of microscopic colitis and for the rising incidence of microscopic colitis in the last 20 years. 2 The majority of literature examining this hypothesis have been reported in the form of case series, in some cases having reported improvement with drug withdrawal and recurrence with re-challenge supporting the supposed etiologic role of the medications.11,12
In a recent systematic review, Pardi et al used a scoring system for measuring the likelihood of drug causality on the basis of the degree of evidence in the literature. Based on their scoring system and review of the literature, 17 drugs were determined to be ‘high’ in terms of likelihood of causality which included some of the most frequently prescribed medications, namely PPIs, SSRIs, and statins. 13 However, even in their analysis, most of the data were from uncontrolled observations. Our results do not support Pardi's hypothesis regarding PPIs, SSRIs and statins. We are aware of one prior analytic study of similar design to ours and that study also failed to show an association between medication exposure and microscopic colitis when compared to patients with chronic diarrhea. 9 Although both studies were relatively small, the consistent finding of a lack of association in the two studies makes it increasingly unlikely that microscopic colitis is caused by these common medication exposures.
Arguing against a causal association between these common medication exposures and microscopic colitis is the lack of a common mechanistic pathway or limited number of pathways. In contrast, the proposed mechanisms by which certain medications may contribute to the development of microscopic colitis are diverse. Proton pump inhibitors may induce an inflammatory response by altering the bacterial flora of the GI tract and subsequently, the composition of fecal stream. Lansoprazole, in particular, may potentially exert differential inhibition of colonic proton pumps through binding to cysteine 321 which is separate from the other proton pump inhibitors in its class and may partially why diarrhea and microscopic colitis have been more frequently associated with lansoprazole compared to other PPIs.8,14 SSRIs may modulate intestinal function through neurohormonal mechanisms involving increased intestinal release of serotonin.15,16 The association of statins with colitis has been proposed to be related to an ischemic pathophysiology.17,18 While these commonly prescribed medications potentially have direct or indirect effects on the colonic mucosa, there is no clearly identified unifying mechanism by which they may induce microscopic colitis which argues against their direct involvement in the pathophysiology of this disorder.
There were several limitations to our study. First, our small sample case size limited our statistical power. However, as noted above, the consistency of our results with the prior study addressing this question helps to rule-out a type 2 error. Furthermore, most of our observed odds ratios were less than unity, further arguing against a positive association.
We did not evaluate the association of microscopic colitis in specific members of medication classes because of the small number of case subjects. It is possible that only a specific type of medication in the class is associated with microscopic colitis. Some reports have proposed that lansoprazole, simvastatin, and sertraline may be more likely to be associated with microscopic colitis than the other medications in the corresponding classes.9,13 Of course, were it the case that only these select medications within the broader classes contribute to the etiology of microscopic colitis, one would again expect similarity between these unique medications. The absence of such argues against the medication induced hypothesis.
As with most studies, there is a potential for misclassification bias. First, the accuracy of the medication list is limited by the physicians’ ability to review the medication list at each patient visit to assure it is the most updated list. We sought to assess this by comparing the correlation between medications recalled by the patient using a random selection of 80 patients in the case and diarrhea control group at the time of colonoscopy. We compared the hand-written list of medications from the pre-procedure form with the list of medications in the electronic database listed in the clinic visit just prior to the colonoscopy. The agreement was fair to modest as assessed by the kappa statistic [0.4 for PPIs (P = 0.0003), 0.3 for statins (P = 0.01), and 0.50 for SSRIs (P = 0.0001)]. Of course, some of the inaccuracy in agreement could be incomplete patient recall of their medications at the time of colonoscopy.
It is well recognized that the act of prescribing a medication to a patient does not guarantee compliance with the medication. The time period between ingestion of a potential causal agent to the development of microscopic colitis is not known and, in addition, there is often a delay in the diagnosis. There is a possibility that a medication prescribed more than 12 months prior to the diagnosis was not captured thus biasing our results towards the null. However, there is little reason to believe that such bias would shift an odds ratio for a positive association to that of an inverse association as observed in our study. Thus, it seems unlikely that any bias resulting from medication use misclassification has obscured a true association of these medications with microscopic colitis.
We also considered the possible difference in definition of chronic diarrhea for the cases and diarrhea controls. Random biopsies performed at the time of colonoscopy assure that the diarrhea was significant enough for the gastroenterologist to consider a diagnosis of microscopic colitis. Furthermore, for the majority of diarrhea controls and cases, the descriptive indication listed on the pathology form for obtaining colonic biopsies included ‘rule-out microscopic colitis’ when the specimens were sent to pathology. In addition, we examined the characteristics of the diarrhea which were provided by the primary care physician or gastroenterologist just prior to the colonoscopy for this indication. While this information was not uniformly reported in the electronic medical record, we were able to determine that the length of time which patients reported diarrheal symptoms prior to colonoscopy for the cases was slightly shorter (7 months) compared to the diarrhea controls (10 months) but the frequency and associated symptoms diarrhea were similar (3-5 times a day and only a small minority were associated with abdominal cramping and/or weight loss).
It must be noted that we did indeed find a significant decreased association for PPI use and MC compared to random controls which we cannot adequately explain. However, while we also saw a decreased association, this was not significantly seen in comparison to the diarrhea controls. The only other controlled study by Fernandes-Banares 9 similarly did not find a significant association with these commonly prescribed medication classes when comparing their case group to their diarrhea control group, however, their ORs were increased as opposed to decreased. In addition, unlike the results of their study, our study found that microscopic colitis cases patient were less likely to take these commonly prescribed medications. We cannot adequately explain these findings other than considering the possibility of non-random selection of control patients. Therefore, we assessed the representativeness of our random control group by comparing these patients to control subjects selected through random digit dialing within the Greater Philadelphia region for a prior study. 20 The prevalence of co-morbidities and medication use were different between the two cohorts. Our random control sample, had a significantly different proportion of patients with a history of GERD (32% of controls in our study vs. 43%, P < 0.01), diabetes (34% of controls in our study vs. 10%, P < 0.01) and hypertension (70.2% of controls in our study vs. 32.8% respectively, P < 0.01). The random control groups selected for this study from EPIC also had a greater proportion of patients who were prescribed PPIs and SSRIs (45% vs. 11% for PPI use and 29% vs. 10.4% for SSRI use, P < 0.01). Because of these differences, we then measured the association of PPI use and SSRI use with microscopic colitis substituting our control group with the control group in the study by Lewis et al and found that the unadjusted ORs were close to the null for PPIs and not statistically significant for either PPIs or SSRIs [OR 1.5 (0.20-3.53) for PPI use and OR 2.0 (0.59-5.65) for SSRI use]. Of course, any possible association of SSRIs with random controls but not with diarrhea controls could result from detection bias due to medication induced diarrhea other than microscopic colitis rather than from a causal association. 9 For this reason, we and Fernandes-Banares 9 have emphasized the importance of examining associations among patients with chronic diarrhea to support a causal association.
In conclusion, the results of this study argue against the hypothesis that PPIs, SSRIs, and statins may induce the development of microscopic colitis. Because single center studies on this etiology of microscopic colitis are limited by small sample sizes, larger multi-center studies are needed. In addition, alternative etiologic theories should be explored since the available controlled data do not support a strong role for medications in the etiology of these diseases.
Footnotes
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.