
Abstract
Background
Food hypersensitivity is a prevalent condition with poorly characterized underlying mechanisms. In the present pilot study we investigated effects of seal oil and soy oil on meal-induced symptoms and gastric accommodation in patients with subjective food hypersensitivity (FH). Single dose experiment: On three consecutive days, 10 mL of seal oil, soy oil, or saline were randomly administered into the duodenum of 10 patients with subjective FH and 10 healthy volunteers through a nasoduodenal feeding tube 10-20 minutes before the ingestion of a test meal. Short-term treatment study: 24 patients with subjective FH were randomly allocated to 10 days’ treatment with either 10 mL of seal or soy oil, self-administrated through an indwelling nasoduodenal feeding tube, 3 times daily. In both experiments meal-induced abdominal symptoms and gastric accommodation were measured by visual analogue scales and external ultrasound respectively.
Results
Symptoms and gastric accommodation were not significantly influenced by single doses of seal or soy oil. When given daily for 10 days, seal oil, but not soy oil, reduced total symptom scores significantly (P = 0.03). The symptomatic improvement was not associated with improvements in gastric accommodation.
Conclusion
Daily administration of seal oil may benefit patients with subjective FH. The beneficial effect of seal oil in patients with subjective FH can not be ascribed to improved gastric accommodation.
Background
Food hypersensitivity (FH) is a prevalent condition. In the general population, the prevalence is estimated around 25%, whereas in patients with functional gastrointestinal disorders, the prevalence is at least 50% (O'Leary and Shanahan, 2002; Asero et al. 2007). The diagnosis of FH is based on the patients’ self-attribution of their symptoms to adverse reactions to food (Arslan et al. 2004b; Zar et al. 2002), thus including both allergic (IgE-mediated or non-IgE-mediated food allergy) and non-allergic reactions (non-allergic food hypersensitivity) (Johansson et al. 2001). The condition is associated with a high prevalence of psychiatric symptoms, poor quality of life and several (extraintestinal) subjective health complaints (Arslan et al. 2004b; Lind et al. 2005). Self-reported FH, which after relevant clinical examinations remains without any recognised organic or immunological explanation, is in this paper denoted subjective FH, as previously described (Arslan et al. 2004b).
Most patients with FH have symptoms of irritable bowel syndrome (IBS) (Arslan et al. 2004b), which are known to be associated with heightened perception of visceral stimuli (visceral hypersensitivity) (Aziz, 2006). Although psychological factors are strongly implicated (Aziz, 2006), the symptoms may be exacerbated and even reproduced by the administration of lipids (Feinle et al. 2001; Simren et al. 2007), meat soup (Hjelland et al. 2004), lactulose (Morken et al. 2007) and exogenous prostaglandin (Rask-Madsen and Bukhave, 1979). How psychological factors and food or food ingredients interact and evoke IBS-like symptoms in these patients are the subject of much speculation (Akiho et al. 2007).
Long chain polyunsaturated fatty acids (LCPUFA) have a range of different effects in the human body. When administered into the duodenum, they are known to affect various stomach motor functions (Feinle et al. 2001). Thus, in a recent study we showed that duodenal infusion of fat based on soy oil, relaxed the stiff proximal stomach and improved gastric accommodation to a test meal in patients with functional dyspepsia (Lunding et al. 2006). Clinically more important might be the effects of long-term administration of LCPUFA on metabolic and inflammatory conditions (Gil, 2002). Although a long-term administration strategy is normally applied, we found that short-term (10 days') duodenal administration of seal oil markedly attenuated joint pains in patients with inflammatory bowel disease (IBD) (Bjørkkjaer et al. 2004).
Seal oil shares many of the characteristics of fish oils, e.g. relatively high content of long chain n-3 PUFA (i.e. 20 ≥ carbon atoms long). In vegetable oils n-3 PUFA are present as α-linolenic acid (ALA; 18:3n-3), though the amount differs between oils. The main fatty acid in many vegetable oils is the n-6 PUFA linoleic acid (LA; 18:2n-6). ALA and LA are both essential fatty acids and precursors for the endogenously synthesised LCPUFA eicos-apentaenoic acid (EPA; 20:5n-3) and arachidonic acid (AA; 20:4n-6), respectively. However, the capacity in humans to convert ALA to EPA, and especially DHA, is limited (Burdge et al. 2007). The n-3 PUFA in fish oil are mainly located in sn-2 position of the triacylglycerol (TAG) molecule, while almost exclusively in sn-1 or sn-3 position in TAG from seal oil (Brockerhoff et al. 1968; Yoshida et al. 1996). The impact of the positional distribution of FA on the backbone of the TAG from marine oils, on absorption, incorporation and utilization is not clear (Osaki et al. 2005). However, the different fatty acid profiles of marine oils and vegetable oils may have important implications for the amount and type of free fatty acids released by pancreatic lipase in the gut, and by lipoprotein lipase throughout circulation, and thus provides different precursors for further metabolism.
The present pilot study includes one single dose experiment and one short-term treatment study. The single dose experiment was performed to test whether single doses of seal oil or soy oil administered into the duodenum would differentially influence the response to a subsequent meal. The short-term treatment study was executed to characterize potential treatment effects of the oils in patients with food hypersensitivity. In an attempt to elucidate a possible mechanism of action, gastric accommodation in response to the meal was measured using non-invasive external ultrasonography.
Materials and Methods
Patients
Patients with various unexplained abdominal symptoms including dyspepsia, pain, bloating, nausea, vomiting and disturbed bowel habits were included in the study provided they self-attributed their complaints to food intolerance (here denoted self-reported FH). The clinical examination included a detailed medical history, physical examination, and routine laboratory tests in addition to skin-prick test (SPT), serum total-and food-specific IgE, and double-blind placebo-controlled food-challenge (DBPCFC). Patients with clear IgE-mediated food allergy and pregnant or lactating women were excluded. Gastroscopy including biopsies from the stomach and the duodenum was performed to exclude peptic ulcer, Helicobacter pylori infection and coeliac disease. An oral lactose tolerance test analysing blood glucose response was performed to exclude lactose malabsorption. Intestinal permeability and calprotectin in gut lavage fluid were examined to exclude IBD (Arslan et al. 2004a).
Single dose experiment
Ten female patients (range 28-82 years, mean age 49 years) with subjective FH. The response of the patients was compared to that of 10 healthy volunteers (4 females and 6 males, range 23-56 years, mean age 31 years).
Short-term treatment study
Twenty-four patients (22 females and 2 males, range 24-80 years, mean age 43 years) with subjective FH were randomly allocated to short-term treatment with either seal oil (n = 12; 11 females and 1 male, mean age 45 years) or soy oil (n = 12; 11 females and 1 male, mean age 41 years).
Experimental oils
The refined seal oil (Rieber Skinn A/S, Bergen, Norway) was from harp seal (Phagophilus groenlandicus), as specified previously (Madland et al. 2006). The soy oil was commercially available, produced by Mills DA (Oslo, Norway). In the single dose experiment, 10 mL seal oil or soy oil or saline solution was given per day (for 3 days). Thus the participants received about 0.8 g of EPA, 0.4 g docosapentaenoic acid (DPA), and 0.9 g of docosahexaenoic acid (DHA) from the seal oil per day. From the 10 mL of soy oil, the participants received about 5.0 g LA.
In the short-term treatment study, the participants self-administered 10 mL seal or soy oil three times daily for 10 days, resulting in a daily intake of approximately 2.4 g EPA, 1.1 g DPA and 2.6 g DHA, i.e. 6.1 g of n-3 LCPUFA from seal oil or 15.0 g n-6 LA from soy oil per day. In both experiments, the participants were blinded regarding the administered solutions and there were no taste or smell or known side effects that could identify the specific treatment.
Meal induced symptoms
As in several prior studies (Gilja et al. 2007) we applied a commercial meat soup (Toro® clear meat soup, Rieber and Son A/S, Bergen, Norway) for symptom provocation and evaluation of gastric accommodation. At each experiment, the subjects drank during 4 min 500 mL of the soup containing 1.8 g protein, 0.9 g bovine fat, 1.1 g carbohydrate and 0.2 g non-soluble seasoning (20 kcal totally). Beforehand, the soup was boiled and then cooled to 37 °C. In previous studies this soup meal induced fed state motility with approximately 3 antral contractions per min in over 85% of patients and controls (Gilja et al. 1995).
The participants were asked to score the meal-induced symptoms on a 100 millimetre visual analogue scale (VAS), where zero denotes absence of symptoms and 100 denotes excruciating symptoms. This Norwegian version of VAS has previously been validated in terms of reliability, validity and sensitivity (NRRK).
Ultrasonography
Two-dimensional (2D) ultrasound images were obtained using a sector scanner (System Five, GE Vingmed Ultrasound, Horten, Norway) with a 4.4-5.0 MHz curvilinear transducer. The participants were scanned while sitting in a wooden chair, leaning slightly backwards with an angle of 120° between the thighs and the spine. Using the method of Gilja et al., three different ultrasonographic measures were applied at each recording time: proximal gastric area, frontal diameter and antral area (Gilja et al. 1995; Gilja et al. 2007). The measures were traced twice and the average result recorded. All sonographic examinations and measurements were performed by one of the authors (G.A.L).
Experimental Procedure
Single dose experiment
In random order, each participant was examined on three consecutive afternoons after fasting from breakfast. By aid of fluoroscopy and a stylet, a thin nasoduodenal tube (Freka® Feeding Tube, Fresenius Kabi, GmbH, Germany) was positioned with its tip to the mid duodenum. The participants kept the tube inserted during the entire trial period. The study design is schematically outlined in Figure 1A. The administrations of oils or saline were performed slowly to prevent arousal of symptoms from -10 to 0 minutes, and the soup meal was ingested 10 minutes thereafter during 4 minutes. The abdominal symptoms (epigastric pain, nausea and fullness) were recorded at -10 and 0 minutes, and postprandially, at 14 and 24 minutes. The ultrasound scannings were performed at the same intervals.

Study design. Acute experiment
Short-term treatment study
Patients were randomly allocated to short-term duodenal treatment with either seal oil (n = 12) or soy oil (n = 12). 10 mL seal or soy oil was self-administered through the indwelling nasoduodenal tube (described above) before meals, 3 times daily for 10 days. Before and after 10 days oil administration, they ingested the test meal of 500 mL during 4 minutes, and abdominal symptoms (epigastric pain, nausea, fullness, satiety and discomfort) were recorded at 0 and 4 minutes, and postprandially, at 14 and 24 minutes (Fig. 1B). Ultrasound scanning was performed at the same intervals.
Statistical analysis
Data were analysed and displayed using GraphPad Prism 5 (GraphPad Software Inc, San Diego, U.S.A). Results are presented as mean with standard error of the mean (SEM) both as time-curves and as area under the time-curves (area between curve and zero, AUC). Each symptom score was examined separately, but because analysis of individual symptoms did not provide any additional information, only the sum of the scores are presented. In the single dose experiment, the three groups were primarily compared by ANOVA. Differences were otherwise evaluated by paired and unpaired Student t-tests. P-values < 0.05 were regarded statistically significant.
Ethical approval
The protocol was approved by the Regional committee for human research ethics, Norway. All participants gave written informed consent.
Results
Most patients claimed intolerance to one or two food items, wheat flour and cow's milk being the food items most often reported intolerance to. All patients had negative biopsy results for Helicobacter pylori and coeliac disease and none of them had indication of lactose malabsorption. One patient in the single dose experiment and one in the short term treatment study had positive DBP-CFC for wheat flour and for egg, respectively. However, both patients had negative SPT and negative food-specific IgE towards the same food items. Hence, these two patients had non-IgE-mediated food allergy or non-allergic food hypersensitivity.
Single-dose experiment
Meal-induced symptoms
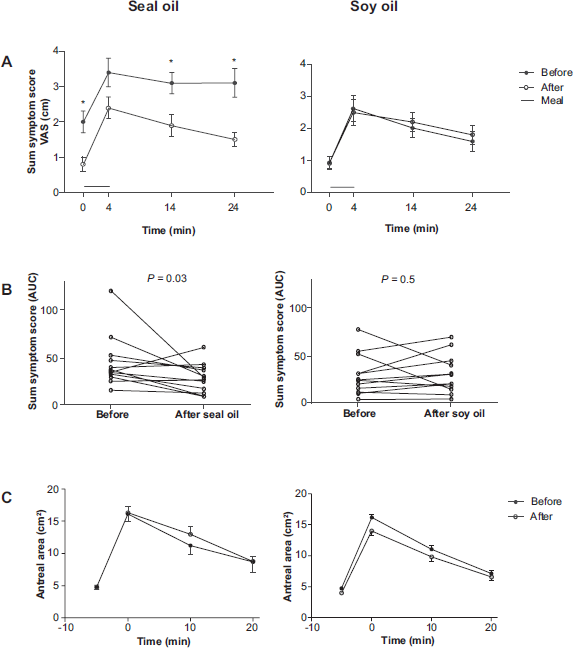
As compared with saline, duodenal administration of seal oil or soy oil from -10 to 0 min before the meal did not significantly influence the symptoms induced by the subsequent meal. The data obtained with saline, soy oil and seal oil administration where therefore pooled and significant differences in sum symptom score were observed between patient group and control group both before and after administration of the meat soup meal (Fig. 2A).

Sum symptom score
Ultrasonography
As compared with saline, duodenal administration of seal oil or soy oil 10-20 min before the meal, did not significantly influence the widths of antral areas after the test meal. Thus the data were pooled, and a significantly wider postprandial antral area was observed in the patient group compared with the control group shortly after finishing the soup meal (P = 0.02) (Fig. 2B).
Short-term treatment study
Meal-induced symptoms
As compared with pre-treatment, 10 days’ administration of seal oil significantly reduced sum symptom scores both before (i.e. at start of the meal) and after meal ingestion (Fig. 3A shows symptom profiles and Fig. 3B area under the curve). Administration of soy oil had no effect on symptoms (Figs. 3A-B).
Sum symptom score (
Ultrasonography
The ultrasonographic measures showed no significant effects on the size of the antral area of the stomach of either seal oil or soy oil administration (Fig. 3C). Neither was there any significant effect of the two treatments on the measures of the proximal stomach (results not shown).
Discussion
As compared with healthy volunteers, patients with subjective FH reported more symptoms in response to the ingestion of 500 mL meat soup and showed more antral distension immediately following the meal. This indication of impaired gastric accommodation is consistent with prior findings in patients with functional dyspepsia (Hausken et al. 1993). Most of our patients had irritable bowel syndrome (approximately 80%) and some few functional dyspepsia according to Rome criteria (Park and Camilleri, 2006). Visceral hypersensitivity is common among such patients, and the discomfort experienced in response to the ingestion of a dilute meat soup indicates indeed that visceral hypersensitivity is typical also for patients with self-reported FH and that the patients’ subjective FH might be less specific for particular food items than that often self-reported.
Single doses of seal oil or soy oil administered into the duodenum did not significantly influence symptoms or gastric accommodation induced by our test meal. However, 10 days’ treatment with seal oil significantly improved abdominal symptoms, both baseline symptoms at start of meal ingestion and symptoms evoked by the meal, without any noticeable effect on gastric accommodation. Similarly administered soy oil had no effect on either symptoms or gastric accommodation.
Because duodenal administration of LCPUFA is supposed to relax the proximal stomach and improve gastric accommodation to meals, we anticipated that symptom improvement in response to seal oil administration would be associated with improvements in gastric accommodation. No such improvements in either proximal or distal (antral) gastric accommodation were seen. Hence, altered gastric accommodation can hardly explain the beneficial symptomatic effect of seal oil.
More likely the beneficial symptomatic effect of seal oil in patients with FH is a consequence of cyclooxygenase (COX) inhibition, a documented effect of long chain n-3 PUFAs (Cleland et al. 2006). Indeed, up-regulated intestinal COX activity has been reported in a mouse model of post-infectious IBS (Collins, 2007) and possibly also in patients with FH (Buisseret et al. 1978; Flatz and Lie, 1982; Peuhkuri et al. 1999). Buisseret et al. (Buisseret et al. 1978) observed a marked rise in the blood and stool concentrations of prostaglandin E2 and F2-α after the ingestion of incompatible food in humans with FH, and Jones et al. concluded that prostaglandin production is an important factor in the pathogenesis of food intolerance in IBS (Jones et al. 1982). Even carbohydrate malabsortion may up-regulate prostaglandin production although neither acetylsalicylic acid nor ibuprofen treatment was able to relieve symptoms induced by ingestion of lactose or lactulose (Flatz and Lie, 1982; Peuhkuri et al. 1999).
Our group of patients with subjective FH had indications of visceral hypersensitivity, a condition in which inflammation may be involved as seen after induction of colitis in animal models (Zhou et al. 2008). Changes in intestinal lymphocytes, eosinophils and mast cells are previously reported in functional gastrointestinal disorders (Rothenberg and Cohen, 2007; Phillips et al. 1979; Park and Camilleri, 2006). In the present study duodenal biopsies were taken mainly to exclude coeliac disease and gut lavage calprotectin was examined to exclude colitis. Long chain n-3 PUFAs have shown inconsistent (MacLean et al. 2005), but indeed some beneficial effects on intestinal inflammation (Belluzzi et al. 1996; Brunborg et al. 2008). Moreover, we have previously reported reduced leucotriene B4 and prostaglandin E2 levels in blood following treatment with seal oil (Brunborg et al. 2008). Long chain PUFAs in seal oil could thus ameliorate symptoms through an anti-inflammatory property.
Seal oil (and the more widely used fish oil) is rich in the natural COX inhibitor EPA, which competes with AA for the same COX enzymes. Also, the EPA-derived prostaglandins and leukotrienes are less pro-inflammatory than those formed from AA. Soy oil, on the other hand, is rich in the n-6 PUFA LA, the precursor of AA, which is metabolised to pro-inflammatory prostaglandins and leukotrienes. We applied a relatively high dose of seal oil, 10 mL three times daily. This high amount of oil was well tolerated with no adverse effects and the mode of administration secured near perfect compliance (according to patients’ verbal reports). The dose corresponds to approximately 5.4 g of n-3 PUFAs a day, which is double the dose required for anti-inflammatory effect (2.7 g of n-3 LCPUFA a day) (Cleland et al. 2006). When administered orally, anti-inflammatory effects of n-3 PUFAs (as fish oil) are usually seen only after 2-3 months of treatment (Cleland et al. 2006). However, in a recent study, using the same mode of administration as here, it was observed a similarly rapid effect of seal oil administration, namely a profound reduction of IBD-related joint pain after 10 days’ treatment (Bjørkkjær et al. 2004). Because n-3, but not n-6, fatty acids are able to inhibit inducible COX activity, we speculate that the reported effect of seal oil on joint pains could be an effect of COX inhibition (Cleland et al. 2006).
Supporting a role of prostaglandins in FH are previous observations that oral administration of a prostaglandin analogue, misoprostol, aggravates functional gastrointestinal complaints (Hausken et al. 1990) while administration of non-steroid anti-inflammatory drugs (NSAIDs), which inhibits the action of COX and thus prostaglandin synthesis, prevents diarrhoea in patients with IBS (Bukhave and Rask-Madsen, 1981). Prostaglandins not only induce increased intestinal transit and diarrhoea, but also affect nociception and visceral sensitivity (Lessof et al. 1983).
The potential usefulness of NSAIDs in patients with FH and IBS is seriously hampered by side-effects (Spiller et al. 2000; Marshall et al. 2004), which include aggravation of mucosal damage and increased intestinal permeability (Aabakken, 1992). As a consequence, these drugs may deteriorate rather than improve important aspects of the pathophysiology of IBS. In addition comes the associated increased risk for cardiovascular events, which are seen especially with the new COX-2 selective NSAIDs (Cleland et al. 2006). In fact, marine oils abundant in EPA may constitute natural COX inhibitors, free of adverse side effects in addition to being cardioprotective (Cleland et al. 2006).
In spite of random allocation to the two treatment arms, baseline symptom scores were somewhat higher in the seal oil group than in the soy oil group (P = 0.01). We cannot exclude a possible influence of this odd result of randomization on the observed differences in effect of treatment. However our small pilot study suggests a beneficial effect of seal oil administration in patients with FH. The encouraging result clearly warrants further studies, both on possible up-regulation of intestinal prostaglandin synthesis in FH and its possible treatment with naturally occurring modifiers of prostaglandin synthesis.
Competing Interests
The author(s) declare that they have no competing interests.
Authors’ Contributions
KG contributed to the design of the study, coordinated and participated in the data collection, statistical analysis and drafted the manuscript. RL contributed to the coordination and practical execution of the study. GAL contributed to design the study, collected data and helped with interpretation of data. AB and LF conceived of the study and designed the study, and, together with TB, helped draft the manuscript.