
Abstract
Introduction
Thrombocytosis is a common disorder in patients diagnosed with iron deficiency anemia. The decreased platelet counts commonly found iron deficiency anemia is rarely reported in clinical practice. The exact mechanism of the occurrence of thrombocytopenia in iron deficiency anemia remains unclear. In this case report we discuss a triad of symptoms seen in the African American population: Iron deficiency anemia, menorrhagia and thrombocytopenia.
Case presentation
A 40 year old multiparous African-American woman presented with heavy vaginal bleed, severe anemia (3.5 g/dL) and thrombocytopenia (30,000/mm3). The peripheral blood smear showed marked microcytic hypochromic cells with decreased platelets counts. After excluding other causes of thrombocytopenia and anemia, increased red cell distribution width and low iron saturation confirmed the diagnosis of iron deficiency anemia. Treatment for iron deficiency anemia was initiated with intravenous and oral iron supplements. Two months following treatment of iron deficiency anemia, the triad of manifestations resolved and patient remained stable.
Conclusion
Profound degree of iron deficiency anemia can present with thrombocytopenia and severe menorrhagia. Iron replacement should be the main treatment goal in these patients. This case report further supports the 2 compartment model of the role of iron in maintaining platelet counts.
Introduction
Iron deficiency anemia is the second most common nutritional deficiency in the United States with an estimated 3.3 million females in their reproductive life affected by iron deficiency. 1 Almost all patients with iron deficiency will have normal or elevated platelet counts, some higher than 1000 × 109/L at diagnosis, however, thrombocytopenia in association with iron deficiency is rarely reported.2,3 The exact mechanism of thrombocytopenia is not well understood and is postulated to have a role in alteration in the activity of iron-dependent enzymes in megakaryocytes and thrombopoiesis. 4 In 1978, Beard and colleague 5 first noticed the triad of combination of iron deficiency anemia, thrombocytopenia and heavy vaginal bleeding in alpha-1 thalassemia trait patients. Later on, Berger and colleagues 6 noticed a similar triad of symptoms without any hemoglobinopathy. Since then, very few cases have reported this triad. The purpose of this case report is to explore the triad further for the combination of iron deficiency anemia, heavy vaginal bleeding and thrombocytopenia and to define whether iron supplements is an effective approach to treat all three manifestations together.
Case Summary
A 40 year-old African American woman was admitted to the intensive care unit for heavy vaginal bleeding that lasted 4 days. Vaginal bleeding was associated with lightheadedness, palpitation, weakness and fatigue. She reported a seven year history of uterine leomyomas that caused recurrent episodes of menorrhagia. Due to inadequate iron supplemention, she consequently developed iron deficiency.
Physical examination revealed a blood pressure 110/70 mmHg, a heart rate of 105 bpm, a respiratory rate of 18 breaths/min, and a temperature of 98 degrees Fahrenheit. She appeared pale; no icterus, petechiae, ecchymosis, or purpuric lesions noted. She had no lymphadenopathy. Lungs were clear to auscultation. Cardiac examination revealed cardiac grade 2/6 to 3/6 systolic flow murmur. The liver span was 9 cm and spleen was not palpable. Pelvic examination showed vaginal bleeding. No bleeding from any other site was observed.
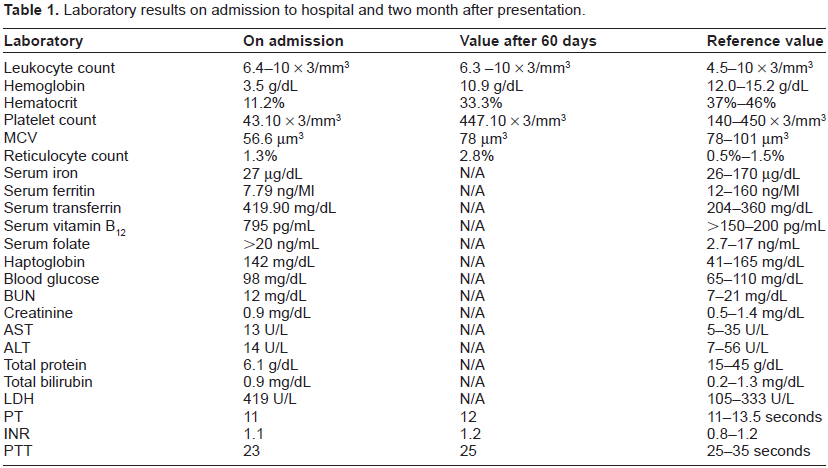
Initial laboratory data is summarized in Table 1. Her Hemoglobin level was 3.5 g/dL (normal range; 12.1–15.1 g/dL) and platelet count was 30,000/mm3 (normal range: 150–400 × 109 per liter). Mean corpuscular volume (MCV) was 56.6 femtolitre (normal range; 80–100 femtolitre) and Red cell distribution width (RDW) was 37.6; (normal range; 11%–15%). Reticulocyte count on admission was 1.3% (normal range; 0.5%–1.5%). Iron studies revealed serum iron 27 µg/dL (normal range; 50–170 µg/dL) serum ferritin 7.79 ng/dL (normal range; 12–150 ng/mL), serum transferring 419.9 mg/dL (normal range 204–360 mg/dL), percent saturation was 4%. Results of the iron studies were consistent with iron deficiency anemia. The peripheral blood smear showed marked microcytic hypochromic cells with decreased numbers of platelets. No platelet clumping was noticed (Figure 1A and B).
Laboratory results on admission to hospital and two month after presentation.

(
Her coagulation parameters were normal. Work up for systemic lupus erythematosus, HIV, immune and non-immune mediated thrombocytopenia, thrombotic thrombocytopenic purpura was unremarkable. Ultrasound of pelvis showed an anteverted uterus with heterogenous parenchyma and calcified anterior myoma and 0.44 cm ecchodense wall thickness with adenomyosis.
The patient was administered four units of packed red blood cells, two doses of intravenous iron sucrose complex 125 mg for two consecutive days, oral iron sulphate tablets 325 mg three time a day, vitamin C 500 mg orally daily and Northindorne 10 mg orally three times a day.
On day 5, she was discharged home with hemoglobin of 10.3 and platelet count 79,000/mm3. Upon discharge the patient was advised to take oral iron supplements and proceed with hysterectomy. Sixty days after iron supplementation and post-hysterectomy, platelet count improved to 4,47000/mm3, hemoglobin increased to 10.9 g/dL and reticulocyte count 2.8% (normal range; 0.5%–1.5%). Figure 2A and B describes the platelets counts and hemoglobin trend after inititating iron therapy.

Response to iron therapy plotted against time.

Hemoglobin level after iron supplementation.
The resolution of severe symptomatic anemia along with thrombocytopenia following iron supplementation strengthens the hypothesis that iron therapy plays an important role in improving iron deficiency anemia associated thrombocytopenia.
Discussion
Iron deficiency anemia has been known to be associated with reactive thrombocytosis.2–4 In this report we discussed the rare ocurrence of menorrhagia, thrombocytopenia and iron deficiency anemia that is rarely reported in the literature.5,6 This report further illustrates that iron deficiency anemia treatment with iron supplements can correct the associated decrease in platelet counts. The resolution of thrombocytopenia with iron supplementation will occur provided other causes of thrombocytopenic disorders are excluded such as acute hemorrhage, hemolysis, chronic inflammatory disorders, trauma, folate deficiency and Vitamin B12 deficiency and thrombotic thrombocytopenic purpura.
Polette et al 8 have demonstrated in animal models that iron, a key element in lipid peroxidation, plays an important role in platelet aggregation. Iron produces oxygen free radicals that induce the release of arachidonic acid and thromboxane A 2 from platelet phospholipids. Barradas et al 9 demonstrated that iron chelators such as deferoxamine inhibited platelet aggregation, production of thromboxane and lipoxygenase activity suggesting platelet aggregation is dependent on iron.
In patients with menorrhagia, inadequate contraction of spiral arterioles in the endometrium leads to qualitative and quantitative platelet dysfunction causing prolonged period of heavy menstrual flow. 10 In order to understand possible interactions between iron deficiency anemia, platelet behavior and menorrhagia, Akoy et al 11 evaluated the effect of iron therapy on platelet function among women with menorrhagia. They found iron deficiency anemia in women caused arachidonic acid induced platelet dysfunction through iron-containing enzymes may give rise to increased menstrual blood loss, which can be reversed through iron repletion. Kiem et al 12 showed that iron is present in platelets in a concentration of approximately 12.28 µg/g, further supporting the hypothesis of Karpatkin and colleagues 13 that iron may have a functional role in controlling platelet production.
A 2-compartment model has been designed to study the role of iron in maintenance of platelet counts and reactive thrombocytosis. 14 The two main components include the “inhibitor” compartment and the “essential component.” In the “inhibitor” compartment, iron either directly or indirectly inhibits the rise in platelet count above steady state levels via an unknown mechanism. This postulated mechanism accounts for thrombocytosis that occurs following iron depletion through blood loss or an iron-deficient diet. In the “essential component” compartment of the model, iron is required in the synthesis or production of platelets. During iron depletion, thrombopoiesis will begin until sufficient iron is available in the “essential” compartment for synthesis of platelets. This supports the two compartment model of iron's role in maintaining platelet counts. 14
In our case, patient had severe iron deficiency, as manifested by hemoglobin level of 3.5 g/dL and thrombocytopenia 30,000/mm3. Therefore, at the time of initial presentation, iron stores of the essential component compartment were exhausted and thrombocytopenia ensued. When iron was replaced in the form of packed erythrocyte transfusions and iron supplementation, thrombopoiesis occurred and the platelet count returned to normal. Finally, she progressed to thrombocytosis owing to secondary overshoot resulting from the function of iron in the inhibitor compartment. Our patient did not require any platelet transfusion.
An increasing reticulocyte count is a reliable way to confirm iron responsiveness during the initial period of observation and supplementation. In patients with concomitant thrombocytopenia, a rapid rise in the platelet count also can serve as evidence of an appropriate hematological response to iron replenishment. Similar to our case, Ganti et al 15 had a case of a 39 year female Jehovah's Witness with a 10 month history of menorrhagia and pancytopenia and severe iron deficiency. Since blood transfusion was not allowed, she was started on intravenous iron replacement therapy which caused initial leucopenia and thrombocytopenia which recovered upon continuing iron supplementation Again such finding in similar cases clarifies the potential role of iron in thrombocytopenia associated with iron deficiency anemia.
Conclusion
Iron supplements can improve iron deficiency anemia, platelet counts and menorrhagia. This case further supports the two compartment iron's role in maintenance of platelet counts. Physicians should be aware of unexplained menorrhagia with normal coagulation profile. Patients can present with severe iron deficiency anemia and thrombocytopenia. It is highly desirable that life threatening conditions like thrombotic thrombocytopenic purpura and other causes of thrombocytopenia should be excluded. Future studies should focus more on the hemoglobin and iron levels cut off to determine which subset of patient's population can present with thrombocytopenia.
Author Contributions
Conceived and designed the experiments: RI, AK, SR, MK, OM, EH, MZ. Analysed the data: RI, AK, SR, RD. Wrote the first draft of the manuscript: RI, AK, SR, MK, RD, EH, AG, OM, MZ. Contributed to the writing of the manuscript: RI, AK, SR, MK, EH, AG, OM, MZ. Agree with manuscript results and conclusions: SR, EH, RD, AG, MZ. Jointly developed the structure and arguments for the paper: RI, AK, SR, MK, EH, AG, OM, MZ. Made critical revisions and approved final version: RI, AK, SR, MK, EH, AG, OM, MZ. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Written consent was obtained from the patient for publication of this case report and any accompanying images