
Abstract
Ureteritis cystica is an uncommon cause of acute renal pain. The aetiology remains unclear and the diagnosis may be difficult to establish. We report the case of a 29 year old woman with a history of repeated urinary tract infections presenting with acute renal colic in the absence of lithiasis. We review the diagnostic tools available to make the diagnosis and the recent pertinent literature.
Introduction
Ureteritis cystica (UC) is usually suspected when defects of filling are seen in the ureter in contrasted images of the urinary tract. Although is the condition is usually an incidental finding during the evaluation of the urinary tract, it presents occasionally with acute flank pain. Differential diagnosis with lithiasis and neoplasms requires a thorough evaluation. The case described here illustrates this rare form of presentation. We describe the imaging and endoscopic investigations leading to the diagnosis of UC.
Case Report
A 29 year old female presented with acute right renal colic. There was no haematuria or past history of urolithiasis. She had had recurrent urinary tract infections. She did not smoke. Past medical history and review of systems was otherwise unremarkable.
A urinalysis showed a pH of 6, was positive for haemoglobin and leukocyte esterase (++). The sediment showed 53.6 epithelial cells/µL and 1590 bacteria/µL. The blood count and serum creatinine were within normal limits. An abdominal roentgenogram showed no abnormal calcifications.
An intravenous urogram was performed to rule out the presence of radiolucent stones. Bilateral renal morphology and function were normal including a normal left ureter. In the distal right ureter there were multiple defects of filling and moderate dilatation. The cystogram phase was normal (Fig. 1).

IVU.
Voided urinary cytology was negative for malignant cells. Ureteroscopy revealed multiple bulky lesions in the distal right ureter. Cytology of the ureteral washings was also negative for malignant cells.
To further refine the diagnosis computerized axial tomography (CT) and urological magnetic resonance (MRU) were performed. Both studies showed that the right ureter was occupied from the crossing of the iliac vessels to the bladder by material with characteristics soft tissue. On MRU there was low enhancement after the administration of gadolinium. These findings were compatible with ureteritis cystica, polyposis or neoplasia. There was no evidence of retroperitoneal, iliac or inguinal lymphadenopathy, or hepatic lesions (Figs. 2 and 3).

CT scan.

MRU.
In view of these findings, we performed a follow-up ureteroscopy 1 month later. It showed partial regression of the lesions. A biopsy was negative for cancer.
With the presumptive diagnosis of ureteritis cystica, we opted for observation with annual follow-up. Urinary tract infections were treated with antibiotics. At 1 year follow-up the patient remains asymptomatic and free of urinary tract infections, haematuria or renal pain.
Discussion
Ureteritis cystica is defined as the cystic transformation of the epithelial nest of Brunn, with the appearance of numerous cysts containing clear fluid with sizes between 1 and 10 mm with fattened epithelial walls. It is considered of the result of irritation in nonspecific chronic inflammations. 1 Other etiological factors that have been postulated include bilharziasis, vitamin A excess and increased immunoglobulin A. None of these factors have been proven to play a specific role. 2
Ureteritis cystica is an infrequent condition which is predominantly found in adults females, 3 but also reported to occur in men and children. Although usually unilateral, bilateral cases have been described. 4
The location of the cysts is predominantly in the proximal ureter, but they can be found at any level of the urothelium. When present in the bladder they are referred to as cystitis cystica. The lesions are benign with low potential for degeneration, although occasionally it has been associated with bladder carcinoma or renal carcinoma. 4
The clinical presentation is variable. Ureteritis cystica is usually detected during the evaluation of urinary tract infections (82%), lithiasis (53%) or haematuria (52%).5–7
The most commonly used imaging techniques are excretory urography and retrograde pyelography. In these imaging studies one can observe numerous defects of filling with well-defined, rounded smooth contours often with a “scalloping” appearance. 7 In cases where the diagnosis is uncertain, as was the case in our patient, CT scan and MRU can be used to better define the nature of the lesions, their extent, the presence of other abnormalities. Other lesion that can have a similar appearance include, (radiolucent stones, clots, veins, air bubbles, tuberculous ureteritis). 8
When the imaging studies are not conclusive, ureteroscopy plays a fundamental roll in the ability to directly visualize the cystic formations and to take biopsies in order to realize an anatomo-pathological analysis. 7 In fact, many authors consider endoscopic diagnosis as the most appropriate in these cases. 6
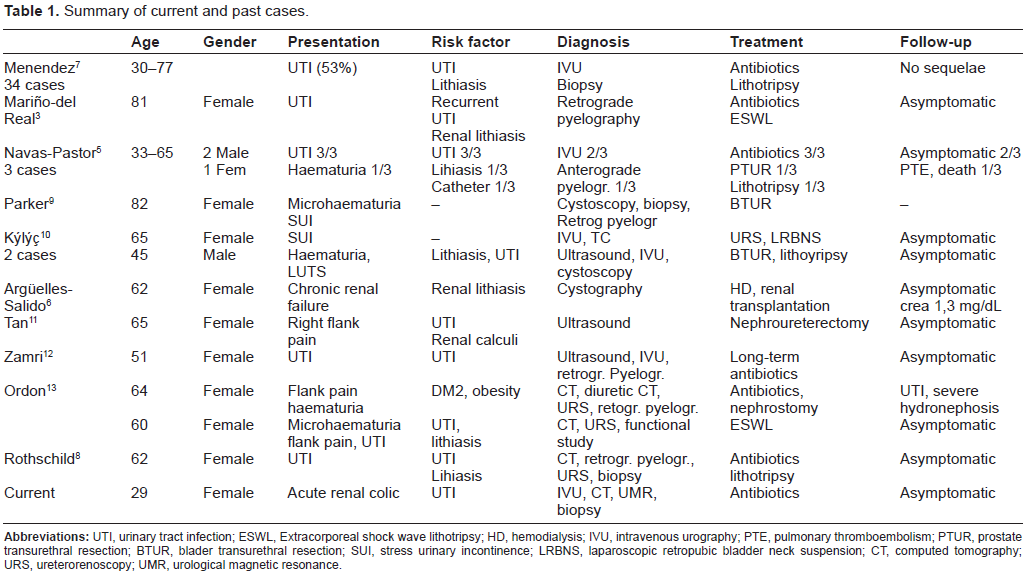
The treatment consists of eliminating the process which is causing the inflammation (infection, lithiasis), although in those cases in which obstruction other measures may be appropriate. In Table 1 we summarise the reported cases of this condition.
Summary of current and past cases.
Conclusions
Ureteritis cystica is a benign condition often associated to other urological diseases. Imaging studies should be complemented with ureteroscopy and biopsy when indicated when tumour is suspected. Treatment of the underlying cause and watchful observation are the mainstays of management. The case presented is unique because it presented with acute renal colic.
Author Contributions
Wrote the first draft of the manuscript: BPF, MFLG. Contributed to the writing of the manuscript: MHP, MMI. Agree with manuscript results and conclusions: JMSA, FJDA. Jointly developed the structure and arguments for the paper: BPD, MFLG. Made critical revisions and approved final version: JMSA, FJDA. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.