
Abstract
Tetralogy of Fallot is the most common form of cyanotic congenital heart disease. Survival after the age of 12 years without corrective surgery is rare. We present the case of a 25 year-old man with uncorrected tetralogy of Fallot. Possible reasons for the longetivity in this patient are left ventricular hypertrophy and systemic to pulmonary shunting through internal mammary arteries.
Introduction
Tetralogy of Fallot is the most common form of cyanotic congenital heart disease accounting for about 10% of all cases of congenital heart diseases. 1 It consists of interventricular septal defect, right ventricular outflow tract obstruction, an overriding aorta and right ventricular hypertrophy. Without corrective surgery, few patients with tetralogy of Fallot reach adulthood with an average life expectancy of 12 years. 2 We present the case of a 25-year old man with an uncorrected tetralogy of Fallot. We also review the possible factors contributing to his longetivity.
Case Report
A 25 year-old man presented to our cardiology clinic with recurrent easy fatiguability, breathlessness on moderate exertion (which is usually relieved by squatting) and palpitations from childhood. There was no history of paroxysmal nocturnal dyspnoea; neither was there pedal, facial or abdominal swellings. The patient is not a known hypertensive, diabetic or asthmatic. On examination, he was plethoric, had both central and peripheral cyanosis and grade 3 finger clubbing. There was no peripheral oedema.
Cardiovascular system examination revealed a pulse of 88 beats per minute, moderate volume and regular. The blood pressure was 100/80 mmHg, apex beat was localised in the 5th left intercostal space within the mid clavicular line and there was left parasternal heave. On auscultation, there was first and second heart sounds, loud pulmonary component of second heart sound, and grade 4/6 pansystolic murmur which was loudest at the left lower sternal edge. The chest was clinically clear.
The haematocrit was 60%. His serum electrolyte, urea and creatinine levels were normal.
Chest radiography showed an enlarged cardiac silhouette with left ventricular preponderance, leftsided aortic arch and dilated pulmonary arteries. Electrocardiography showed sinus rhythm, right atrial enlargement, biventricular hypertrophy with secondary ST-T wave abnormalities. Echocardiography showed a membranous ventricular septal defect measuring 20.9 mm with a right to left shunting of 1.12 m/second, minimal aortic override (with aortic diameter of 34.5 mm), hypertrophied septal wall measuring 14 mm in diastole, small volume left ventricular cavity with left ventricular ejection fraction in the lower limits of normal (55%). There was also right ventricular hypertrophy with the right ventricular free wall of 11.2 mm, dilated right atrium with right atrial area of 26.14 cm2, bicuspid pulmonary valve with a small pulmonary artery of 14.6 mm, subpulmonary stenosis with right ventricular outflow tract gradient of 1.15 mmHg. The patient remained clinically stable for four years after his initial presentation, but died suddenly at the age of 29 years in a private facility close to his neighbourhood from hypoxic spells.
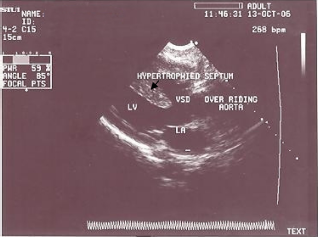
A four-chamber transthoracic echocardiography image.
Discussion
Although uncorrected tetralogy of Fallot has been reported in patients as old as 52 years to 86 years,3–8 this is the oldest patient to the best of our knowledge with uncorrected tetralogy of Fallot being reported in our environment.
Without corrective surgery 10% of patients survive to their thirties while only 3% reach their forties or older. 2 Three main factors have been identified for the longetivity in natural survivors with unoperated tetralogy of Fallot. First is the small pulmonary artery with presumed slow development of subpulmonary obstruction. 9 Another factor identified is that of left ventricular hypertrophy 10 as seen in our patient who had a interventricular wall thickness of 14 mm in diastole. It is said that left ventricular hypertrophy acts by delaying the shunting of blood from the right to left ventricle. 11 The third factor is extracardiac shunting including patent ductus arteriosus or systemic to pulmonary shunting through internal mammaries. 12 In our patient there was no demonstrable patent ductus arteriosus but there were dilated pulmonary arteries on the chest radiograph which is highly suggestive of a right to left shunt. Our patient died from hypoxic spells which has been documented as the most common cause of death in uncorrected tetralogy of Fallot. 13
Conclusion
Uncorrected tetralogy of Fallot occurring at 25 years is rare in our environment. We propose that the longetivity in this patient is partly due to left ventricular hypertrophy and possibly systemic to pulmonary shunting via internal mammary arteries.
Disclosures
This manuscript has been read and approved by all authors. This paper is not under consideration by any other journal and has not been published elsewhere. The authors state that they do not have any conflict of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
Acknowledgement
Our appreciation goes to every medical staff of Cardiology Unit, Department of Medicine, University of Abuja Teaching Hospital, Gwagwalada, Abuja. No grant was received for this work.