
Abstract
Familial Mediterranean Fever (FMF) is a recurrent disease characterized by inflammatory process effecting synovial membranes such as peritoneum, pericardium and joints. It usually presents with acute abdominal pain. Intestinal obstruction secondary to adhesions may be observed in FMF patients. Sometimes diagnosing intestinal obstruction can be a challenging problem. We were presented a patient with FMF and adhesive intestinal obstruction. He was operated on after 10 days of symptoms. Delay in diagnosis and treatment of the case discussed with literature review.
Introduction
FMF is an inflammatory disease with recurrent attacks. Patients are usually presented with fever, abdominal pain, arthralgia and chest pain. Although it can be observed worldwide, most of the patients are originated from Middle East and Mediterranean region. 1 FMF is an inherited disease with autosomal recessive trait. The disease is caused by mutations in the MEFV gene which is related to regulation of inflammatory process. Approximately 95% of patients with FMF have peritoneal involvement. 2 Acute abdominal attacks are a serious problem. They can cause unnecessary laparotomies specially with the mistaken diagnosis of appendicitis. Recurrent peritonitis may also result in intraabdominal adhesion formation with intestinal obstruction.
In this report, a patient operated due to adhesive intestinal obstruction with FMF was presented. Delay in diagnosis and treatment were discussed with literature review.
Case
Twenty-four year old Turkish man, presented with history of nausea, vomiting and weight loss in the last ten days. His medical history was remarkable only in the diagnosis of FMF. He had been diagnosed as FMF without any genetic testing, only clinical findings. He was receiving colchicine treatment. He had been followed-up as an acute FMF attack in a different hospital before admission to our clinic. On physical examination, he was pale and lean in appearance. The arterial blood pressure was 100/60 mm-Hg with the pulse rate of 78/minute- rithmic. The abdominal examination revealed minimally distended abdomen with tenderness in all quadrants. There were no rebound tenderness and defence in abdominal palpation. Bowel sounds were hipoactive. The rectum was empty in rectal examination. Laboratory results were as follows: White blood cell count: 12,200/mm3 (2000–10,000 mm3), CRP: 138.2 mg/dl (0–5 mg/dl), ESR: 23 mm (1 hour), 52 mm (2 hour). Other laboratory tests including glucose, urea, creatine and electrolytes were normal. There was a small bowel air-fluid level in abdominal x-ray on right side (Fig. 1). Dilated intestinal loops were detected in abdominal ultrasonography. The patient was hospitalized. He was given intravenous fluids (Isotonic 1000 cc and Isolyte 1000 cc solutions) before operation. He underwent laparotomy. On exploration, jejenal loops were found dilated. There were intrabdominal adhesions in between liver and peritoneum. There was an adhesion formation in small intestine causing total intestinal obstruction about 70–75 cm distal to the Treitz ligament (Fig. 2). The small intestine and mesentery were normal without any ischemia or necrosis. The bridectomy was performed. Parenteral nutrition with Kabiven Peripheral infusion emulsion (3.7 ml/kg/hour) was started postoperatively. Paralytic ileus that has been developed after surgery was treated with mobilization, restricting oral intake and fluid resuscitation. Then the patient was discharged uneventfully.

Air-fluid level in abdominal x-ray.

Adhesion, causing bowel obstruction in exploration.
Discussion
FMF is a disease that can mimic acute abdomen. Peritonitis is one of the major component of the disease. The effected patients are usually presented with acute abdominal pain during an attack. Unnecessary laparotomy with the diagnosis of appendicitis is not rare. Tunca M had been reported that the most common surgical operation performed in FMF patients was appendectomy with the frequency of 19%. 3 In other studies, the appendectomy rate had been found as 9% in patients with FMF. 4 The pathological examination of these cases showed that 4% of appendix were normal without any inflammation signs. Schwabe AD et al reported that about 86% of operations performed in FMF patients were non-therapeutic. 5
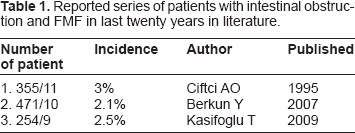
Intraabdominal adhesions secondary to recurrent peritonitis are common in FMF. A sterile exudate is usually found in these patients when laparotomy is performed. It was thought that these exudates are the main cause of adhesion formation. A clinical study reported by Ciftci et al revealed that intestinal obstruction can be detected in 3% of patients with FMF. 6 Berkun Y reported that small bowel obstruction rate was 2.1% in FMF patients without prior abdominal surgery. 7 Multiple laparotomies also increase secondary adhesion formation in FMF patients. Reported series of patients with intestinal obstruction and FMF in last twenty years in literature were seen in Table 1.
Reported series of patients with intestinal obstruction and FMF in last twenty years in literature.
While most of the adhesions are benign in nature, some may cause serious intestinal obstruction with strangulation and perforation. Tırele AG reported two patients with intestinal necrosis after adhesive intestinal obstruction due to FMF peritonitis. 8 Our patient was suffering from intestinal obstruction for about ten days. There was no intestinal strangulation at laparotomy. Early diagnosis and intervention decrease the morbidity and mortality in these patients.
The diagnosis of intestinal obstruction in FMF patient may be difficult. Our patient had been treated as an acute FMF attack for ten days. The signs and symptoms of intestinal obstruction and acute attack are same. Nausea, vomiting and abdominal pain are common symptoms in acute attack and intestinal obstruction. Acute phase reactants such as CRP and sedimentation rate are increased in both cases. While acute FMF attacks usually subside within 12–24 hours, intestinal obstruction usually deteriorates within the time. Ultrasonography and computed tomography can detect bowel obstruction. There was dilated intestinal segments in our case in ultrasonography. The level of the obstruction also effects the clinical picture. Our patient was presented with only nausea and vomiting. The abdominal distention was minimal. Abdominal x-ray was normal except a small bowel air-fluid level on right side. The obstruction was near to Treitz ligament. Upper level intestinal obstructions may be presented with hidden clinical signs. It is also important to point out that using colchicine is not a guarantee for prevention of adhesion formation. Berkun et al stated that spontenous or post-surgical adhesive obstructions can be seen under colchicine treatment.
Our patient was also using colchicine for 4 years. As a consequence, FMF is a recurrent disease that should always be remembered in acute abdominal conditions. Intestinal obstruction secondary to FMF peritonitis can be encountered even under colchicine treatment. The diagnosis of intestinal obstruction can be difficult due to confusion with acute attack. Bridectomy is sufficient in most of the cases.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material. Written consent was obtained from the patient or relative for publication of this study.