
Abstract
We report a case of a 67-year-old woman with rheumatoid arthritis with yellow nail syndrome (YNS) that was caused by bucillamine. All three signs (yellow fingernails, lymphatic edema, and bronchiectasis) of YNS manifested, with characteristic timing, first with the nails turning yellow after when bronchiectasis was noticed. We reviewed 10 case reports from Japan and compared the periods until the appearance of yellow nails after starting bucillamine treatment, as well as those until lung disease and leg edema appeared.
Introduction
Yellow nail syndrome (YNS) is a rare disease associated with pulmonary complaints, mainly bronchiectasis, as well as yellow nails and lymphatic edema. The pathogenesis of YNS remains obscure. However, there is a report describing the role of impaired lymphatic drainage in the pathogenesis of YNS. 1 Bucillamine (N-(2-mercapto-2- methyl-propanoyl)-L-cysteine) is a slow-acting anti- rheumatic drug, with two S-H bonds in its chemical structure. 2 An open trial of bucillamine treatment (300 mg/day after meals for 16 weeks) was conducted in 11 patients with rheumatoid arthritis (RA) who had previous therapeutic failure with gold salts and/or D-penicillamine. The results of this trial seem to indicate that bucillamine is possibly of value as a slow-acting anti-rheumatic drug in some patients for whom gold salts or D-penicillamine therapy has failed previously. 3 There have been no case reports in Japan of bucillamine-induced YNS in RA in which pleural effusion appeared before the onset of yellow nails. There is a concern regarding the diagnosis of YNS when respiratory organ involvement appears early without yellowing of the nails because the yellowing of the nails is usually indicative of the YNS diagnosis. When mild pleural effusion occurs while administering bucillamine, it is necessary to consider the possibility of YNS. We encountered a case in which lung involvement preceded the appearance of yellow fingernails. This case is discussed here, along with a review of the relevant literature.
Case Report
A 67-year-old woman was admitted to our hospital for pain in the left dorsal region that had been present since July 2004, and an increase in pleural effusion on X-rays was documented in September 2004 (Fig. 1A). She became aware of swelling of both hands and elbows in April 1999. Rheumatoid arthritis was diagnosed in our hospital in January 2000, and she was started on bucillamine at 200 mg per day in June. A slight amount of pleural effusion was found on her chest X-rays in August 2001 (Fig. 1B), and she was hospitalized. The amount of pleural effusion was too small to puncture, and nothing else could be done except patient follow-up. A chronic productive cough appeared in August 2002. Leg edema also became marked. Yellow nails were noted in January 2003. No further changes were found, and she continued taking the medication until she was hospitalized in 2004. During this period, the RA was wholly suppressed by bucillamine.
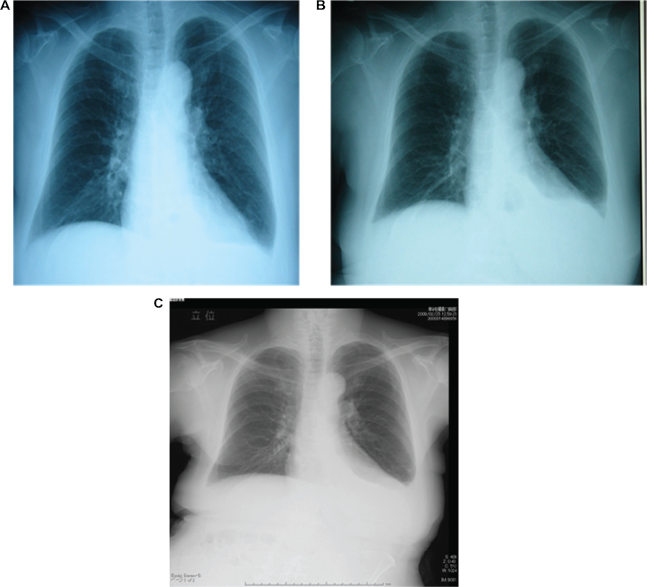
Chest X-rays in August 21, 2001 (
The patient's temperature was 35.1 °C, blood pressure 132/78 mmHg, and pulse 78 bpm. Her heart sounds were normal, but her breath sounds were decreased on the left. All of her nails were yellow (Fig. 2A). Nonpitting edema of both lower limbs was noted (Fig. 3A). There was no apparent swelling or tenderness of the joints.

Appearance of nails. All of the patient's nails were yellow. July 2004 (
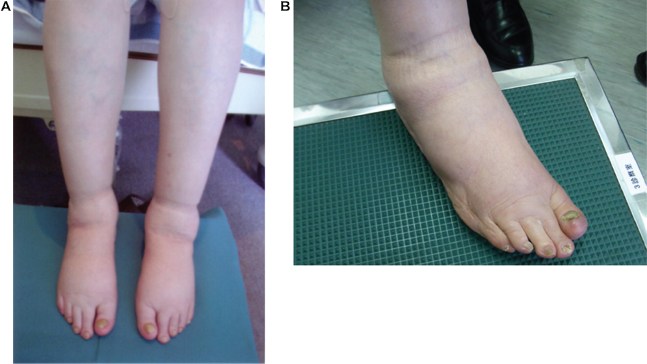
Bilateral lower limb edema and yellow toenails. Nonpitting edema of both lower limbs was noted. July 2004 (
X-rays obtained at the time of hospitalization revealed a diminished left costophrenic angle that had advanced, compared with earlier images. Left pleural effusion was documented by a chest CT scan. Blood tests revealed no decreased liver functions or renal functions (Table 1). Urinary protein was also negative. A thoracentesis was performed, and the pleural fluid was slightly yellow and hazy because of the lymphocyte response. The specific gravity of the effusion was 1.037. The Ribalta reaction was positive for exudative fluid from the effusion. The patient's rheumatoid factor was negative, and the cytology was class 2. Cultures for bacteria, including acid-fast species, were negative (Table 2). The patient was diagnosed with YNS associated with bucillamine, based on her lymphocytic pleural effusion, leg edema, and yellow nails. Bucillamine was discontinued. The total dose of Bucillamine is 29200 mg. It has not improved it though it treated with the Vitamin E. The yellowing of her nails (Fig. 2B), pulmonary effusion (Fig. 1C) and leg edema persisted (Fig. 3B) in February 2009.
Blood tests.

Pleural effusion.

Discussion
The concept of YNS began with a report on a patient with yellow nails and lymphatic edema, but eventually another 13 cases were identified by Samman and White in 1964. 4 YNS was assumed to be a disease that had three signs: refractory pleural effusion, yellow fingernails, and lymphatic edema (which was added by Emerson in 1966). 5 In 1972, Hiller reported that YNS was associated not only with pleural effusion but also with various other pulmonary complaints, including bronchiectasis and pneumonia. 6 Although yellow nails, lymphatic edema, and pulmonary complaints are the three recognized symptoms of YNS, rarely are all three present. However, in 1972, Hiller et al reported that the presence of yellow nails and one other condition was insufficient for a diagnosis of YNS. 6 In 1979, Mattingly reported three cases that suffered concomitant RA. 7 In a series of 97 patients reviewed by Nordkild in 1986, yellow nails were present in 99% of subjects and were the first symptom in 37%. Lymphedema was present in 80% and was the first symptom in 34%. Respiratory tract involvement was present in 63%; it was the first symptom in 29%. 8 As a modification of the characteristic nail criterion, a form of YNS can be diagnosed based on nail thickening that shows a strong curve transversely or longitudinally, color changes (light yellow and light green have been observed, usually in all nails) and nail detachment. The rate of nail growth diminishes to 0.1 to 0.25 mm per week or less with this syndrome, versus the normal rate of 0.5 to 2.0 mm per week. 9
Lymphatic edema might be present in 80% of all patients; it can affect the arms and face but is usually seen in the lower limbs. There was a report attributing yellow nails to abnormalities of the lymphatic vessels. 10 Failure to form lymph or an inherent dysfunction of lymphatic vessels would be the mechanism underlying lymphatic edema, because lymph cannot flow normally when permeability is altered by infection, raising the possibility of so-called “lymph dropsy”. 11
In a recently published case series, pleural biopsy specimens were available for 7 of 41 patients. 1 Although chronic pleural inflammation was again noted, lymphatic vessels appeared grossly normal. Functional lymphatic disorder, rather than structural disease, is currently favored as the shared pathogenic mechanism for the development of pleural effusions and lymphedema. 12 Persistent cough and phlegm production following the onset of the chronic phase are assumed to be the main complaints reflecting pulmonary pleural effusion, bronchial tube involvement, and pulmonary irritation. The diagnosis of bronchiectasis with chronic bronchitis is based on these symptoms. Although, pleural effusion fluid is documented in approximately in 30% of cases. Although many cases show bilateral involvement, one-sided disease does occur. There is also a report describing organized pneumonia as a cause and the efficacy of steroid therapy. 13
Other cases with a history of bucillamine treatment, such as our present patient, have been reported. In 2006, Tanaka et al 14 reviewed 33 cases in Japan treated with disease modifying anti-rheumatic drugs. Shortly thereafter, 28 cases with bucillamine use were reported, and the duration from starting use until disease appearance was 17.5 months on average. Twenty-three of these cases showed amelioration of the disease with discontinuation of the medication or a dose reduction. Yellowing and thickening of the nail plate resulting from bucillamine ingestion were thought to be caused, in part, by the interruption of the process of synthesizing keratin because bucillamine disrupts the formation of a principal ingredient of the nail plate. In the process of nail plate formation, cysteine, which has an S-H radical, becomes cysteine with the formation of an S-S bond and is thereby ultimately changed into keratin. It is thought that the similarity in the chemical structure of bucillamine to cysteine is related to its medicinal action, i.e. bucillamine would presumably alter the composition of keratin because of its structure being similar to that of cysteine (Fig. 4).
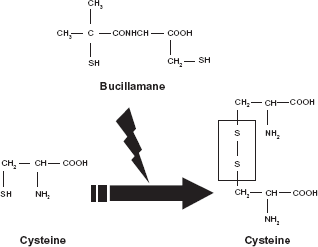
Actions of bucillamine on nail plate. It is thought that the similarity in chemical structure of bucillamine to cysteine is related to its medicinal action, i.e. bucillamine would presumably alter the composition of keratin because of its structure being similar to that of cysteine.
As to the disease onset of YNS, the three characteristic signs do not develop simultaneously, and all three may fluctuate in severity. Some cases initially manifest only yellow nails,
4
but others in which yellowing appear several years, even decades, after edema or lung disease have also been reported.
5
We reviewed 10 reports of Japanese cases in which signs of this condition were followed temporally and compared the periods from starting bucillamine until the appearances of yellow nails, pulmonary disease, and leg edema.14–21 These 10 specific reports were chosen because 1) all three symptoms were found, and 2) they reported how long it took for the three symptoms to appear after taking bucillamine. The average period until the onset of lower limb edema was 13.5
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material. Written consent was obtained from the patient for publication of this study.